w w w . r b o . o r g . b r
Original
article
Radiographic
study
on
the
anatomical
characteristics
of
the
proximal
femur
in
Brazilian
adults
夽
Tércio
Henrique
Soares
de
Farias
a,∗,
Vinícius
Quadros
Borges
a,
Eduardo
Soares
de
Souza
a,
Natália
Miki
b,
Fernando
Abdala
aaHospitalMunicipalDr.CárminoCaricchio,SãoPaulo,SP,Brazil
bDepartamentodeOrtopediaeTraumatologia,FaculdadedeMedicina,UniversidadeFederaldeSãoPaulo(Unifesp),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30October2013 Accepted5December2013 Availableonline18February2015
Keywords:
Femur/anatomyandhistology Femur/physiology
Radiography
a
b
s
t
r
a
c
t
Objective:ToascertainthegeometryofthefemurintheBrazilianpopulationbymeansofa radiographicstudyandtocorrelatethevalueswithregardtosexandright/leftside.
Methods:Five hundred anteroposterior radiographs of the pelvis of skeletally mature patients(250ofeachsex)whodidnotpresentanyosteoarthrosis,fracturesortumoralor infectiouslesionswereanalyzed.Thelengthandwidthofthefemoralneck,lengthofthe femoralaxis,neck-shaftangleandfemoraloffsetweremeasured.
Results:Thefollowingmeanswereobserved:36.54mmforthelengthofthefemoralneck; 37.48mmforthewidthofthefemoralneck;108.42mmforthelengthofthefemoralaxis; 130.47◦fortheneck-shaftangle;and44.4mmforthefemoraloffset.
Conclusion:Themeanvaluesforthemainmeasurementsontheproximalfemurin Brazil-iansdiffered fromthose ofprevious studies.It could also beshown thattherewas a statisticallysignificantmeandifferencebetweenmenandwomenforallthevariables,both ontheleftandontherightside,andthatthemenhadgreatermeansthanthewomen.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Estudo
radiográfico
dos
aspectos
anatômicos
do
fêmur
proximal
dos
adultos
brasileiros
Palavras-chave:
Fêmur/anatomiaehistologia Fêmur/fisiologia
Radiografia
r
e
s
u
m
o
Objetivo:Verificarageometriadofêmurdapopulac¸ãobrasileirapormeiodeestudo radio-gráficoecorrelacionarosvaloresquantoaosexoeaoladodireito/esquerdo.
Métodos:Foram analisadas 500 radiografias anteroposteriores de bacia de pacientes esqueleticamentemaduros,250decadasexo,semapresenc¸adeosteoartrose,fraturase
夽
WorkdevelopedatDr.CárminoCaricchioMunicipalHospital,SãoPaulo,SP,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](T.H.S.deFarias).
http://dx.doi.org/10.1016/j.rboe.2015.02.001
lesõestumoraisouinfecciosas.Forammensuradososvaloresdocomprimentoedalargura docolodofêmur,doeixofemoral,doângulocolodiafisárioedooffsetfemoral.
Resultados: Observou-se uma média de 36,54mm do comprimento do colodo fêmur, 37,48mmdalarguradocolodofêmur,108,42mmdocomprimentodoeixofemoral,130,47◦ doângulocolodiafisárioe44,4mmdooffsetfemoral.
Conclusão: Osvaloresmédiosdasprincipaismedidasdofêmurproximaldosbrasileiros diferemdetrabalhosprévios.Foipossívelevidenciartambémqueexistediferenc¸amédia estatisticamentesignificanteentrehomensemulheresparatodasasvariáveis,tantodolado esquerdoquantododireito,equeoshomenstiverammédiamaiordoqueasmulheres.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Thefemoralheadprojectssuperomediallyand slightly for-wardswhenitarticulateswiththeacetabulum.Theheadand neckformanangleof115–140◦(meanof126◦)withthelong
axisofthebodyofthefemur.1Theangleisgreatestatbirthand decreasesgradually,fromaround150◦innewbornstoaround
133◦at15yearsofage.Itissmallerinwomenbecauseofthe
widthofthepelvisandgreaterobliquityofthebodyofthe femur.2,3
Thefemoral head and the acetabulum ofthe hip bone growindependentlybutinsuchawaythattheydevelop con-gruently. This mechanism is influenced by forces that act externallyintheseareas.Themostimportantoftheseare bodyweightandmuscletensionforces,whichneedtohave magnitudesanddirectionsforappropriateinteractions.Any changetothecompressionforcesoranyjointincongruence willleadtodeformities.Thepressure,archingandshearing stressestowhichthefemurissubjectedareimportantin rela-tiontofractureproductionandalsodevelopmentofvarious pathologicalprocesses.4–6
Radiographicstudieshavesuggestedthatthehipaxisand thefemoralneckarebecoming longer.These changesmay increasetheriskoffracturesthroughtheincreasedlengthof theleverarm.Othernon-geometricfactorsthatmight predis-posetowardfemoralfractureshavebeenwidelydebatedin theliteratureandtheseinclude:advanced age,femalesex, osteoporosis, genetic factors (such as Colia1 Sp1 polymor-phism),smoking,alcoholabuse, previousfracturesandlow estrogenlevels.Thus,newanalysesonhowthegeometric pat-ternmightinfluencepathologicalconditionsofthefemurare pertinent.7–10
AccordingtoAmericanstatistics,morethan 250,000hip fractures occur every year and this number is expected to approximately double over the next 30 years.4 The treat-mentformostfemoralfractures issurgical. Therefore,it is importanttoknowthegeometryofthefemur,sincealarge proportionofimplantscomeinstandardsizes,selectedfrom arangesupplied bymanufacturers.For example,thePFN®
short nail (AO/ASIF) can provide inclinations of 125◦, 130◦
or135◦ betweenthescrewsoftheneckandtheaxisofthe
intramedullarynail. Choosingtheseimplants wronglymay giverisetoalterationstotheanatomyofthehipjoint.11,12
Becauseofthe clinicalimportanceofthemorphometric aspectsof the proximalfemur, a wide-ranging surveywas
conductedinordertoprovidedataonthegeometryoffemoral bonesamongBrazilians.
Theaimsofthepresentstudyweretoascertainthefemoral geometryoftheBrazilianpopulationbymeansofradiographic evaluationsandcorrelatetheparameterswithregardtosex andright/leftside.
Materials
and
methods
An observational cross-sectional study was conducted, in whichpatientswhohadundergoneradiographyonthepelvis inanteroposterior(AP)viewwereevaluated.Thepopulation comprisedof250menand250womenwhowereattendedat theemergencyserviceorintheoutpatientclinicorwardsof theorthopedicsandtraumatologyservice.Noneofthe radio-graphicimageswasproducedforoccupationalreasons.The APradiographsofthepelvisincludedinthisstudywerefrom skeletallymaturepatientswhodidnotpresentosteoarthrosis, fracturesortumoralorinfectiouslesions.
Toobtainthe radiographs,theincident raywasdirected along themedianline, justabovethepubicsymphysisand thefeetwererotatedinternallyataround15◦.Thepatientwas
positionedindorsaldecubitusandtheampoulewasonemeter fromtheframe.Thedegreeofmagnificationobtainedthrough theradiographicmethodwascorrected.
Thefemoralmeasurementsanalyzedwereasfollows:
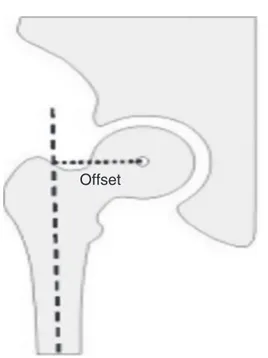
Offset–distancebetweenthecenterofrotationofthehip andalinetracedoutperpendicularlythroughthecenterof thefemoralshaft(Fig.1).
WFN–widthofthefemoralneck,i.e.thedistanceatthe mid-pointofthefemoralneck,perpendiculartoitsaxis(Fig.2). LFA –lengthofthe femoralaxis,i.e.thestraight-line dis-tancebetweentheextremitiesofthegreatertrochanterand femoralhead,inthefrontalplane(Fig.2).
LFN–lengthofthefemoralneck,i.e.thedistancein mil-limetersbetweenthelowerregionofthefemoralheadand thebaseofthegreatertrochanter(Fig.2).
NSA–neck-shaftanglecreatedbetweentheneckandshaft, which was measured in the frontal plane by means of goniometry(Fig.3).
Offset
Fig.1–Measurementoftheoffset.
softwareusedinthisstatisticalanalysiscomprisedSPSSV17, Minitab16andExcelOffice®2010.Thesignificancelevelwas
setat0.05(5%)andalltheconfidenceintervalsconstructed overthecourseofthestudywere95%.
Results
Therightandleftsideswerecomparedforallthevariables
(Table1).Thesecomparisonsweremadeseparatelyforeach
genderandforbothtogether(general).Here,thepaired Stu-dent’sttestwas used,giventhatthedatawere paired,i.e. thesamesubjectprovidedthestudylimbandhisorherown control.
Itcouldbeseenthatsomeofthecomparisonsbetweenthe sideswerestatisticallysignificant.Theresultsfrom measur-ingthewidthofthefemoralneckandoffsetpresentedmean differencesbetweenthesidesforbothsexesandingeneral.
Incomparingthelengthsofthefemoralneck,therewas onlyastatisticallysignificantdifferenceinthegeneral com-parison,withameanof36.65ontheleftside,versus36.44on therightside(p=0.048).
WFN
LFA
LFN
Fig.2–Widthofthefemoralneck(WFN);lengthofthe femoralaxis(LFA);lengthofthefemoralneck(LFN).
NSA
Fig.3–Neck-shaftangle(NSA).
Ontheotherhand,regardingthelengthofthefemoralaxis, therewasonlyastatisticallysignificantresultfromcomparing themen,suchthatthemeanfortheleftsidewas114.06,versus 114.39ontherightside.
Lastly,regardingtheneck-shaftangle,therewere statisti-callysignificantdifferencesbetweenthesidesforthewomen and ingeneral.Itneedstobehighlightedthatthe leftside alwayshadagreatermeanthantherightside.
Thesexeswerethencomparedforallthevariables.These comparisonsweremadeontherightsideandontheleftside. TheANOVAtestwasusedhere(Table2).
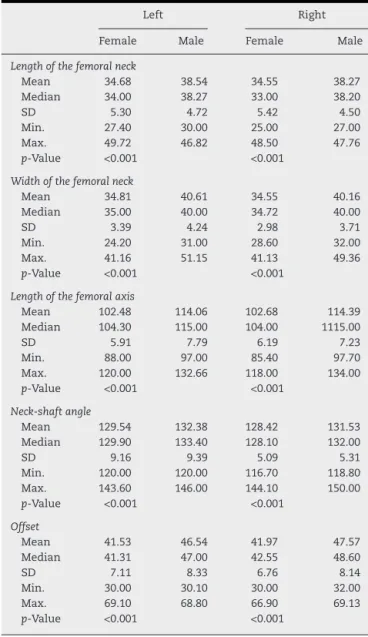
It could be seen that bothfor the left side and for the rightside,therewerestatisticallysignificantmeandifferences betweenthemenandwomenforthefivevariables.For exam-ple,withregardtotheoffsetontherightside,themeanforthe womenwas41.97,versus47.57forthemen,andwithregard totheoffsetontherightside,themeanforthewomenwas 41.53,s46.54forthemen(p<0.001).Itcouldbeseenthatforall thevariablesonbothsides,themenhadgreatermeansthan thewomen.
Discussion
Several aspectsof the geometry of the femoralneck have beenfoundtoinfluencetheriskofhipfractures.Studieshave correlatedgreaterlengthofthefemoralneckandlower val-ues forthe neck-shaft angle with greater incidenceof hip fractures.8,13,14
Population-basedstudieshaveshownthat,overtime,there hasbeenanincreaseinthelengthofthefemoralneckand adecreaseinthewidthoftheneckinthefemalepopulation andhavecorrelatedthesechangeswithanincreaseintherisk offractures.Thismayhavecontributedtowardtheone-third increaseintheincidenceofhipfractures.15,16
Fewstudiesevaluatingthegeometryoftheproximalfemur havebeenconductedinBrazil.17,18Becauseoftheimportance ofthemorphometricevaluation,alargersamplewasrecruited forthepresentstudy(250radiographsfrommenand250from women)thanwasusedinpreviousstudies.Moreover, mea-surementsofthefemoraloffsetwereincludedinthepresent study.
Table1–Comparisonofthevariableswithregardtotherightandleftsides.
Female Male General
Left Right Left Right Left Right
Lengthofthefemoralneck
Mean 34.68 34.55 38.54 38.27 36.65 36.44
Median 34.00 33.00 38.27 38.20 36.10 36.00
SD 5.30 5.42 4.72 4.50 5.37 5.31
Min. 27.40 25.00 30.00 27.00 27.40 25.00
Max. 49.72 48.50 46.82 47.76 49.72 48.60
p-Value 0.355 0.056 0.048
Widthofthefemoralneck
Mean 34.81 34.55 40.61 40.16 37.71 37.25
Median 35.00 34.72 40.00 40.00 38.00 37.00
SD 3.39 2.98 4.24 3.71 4.81 4.45
Min. 24.20 28.60 31.00 32.00 24.20 28.60
Max. 41.16 41.13 51.15 49.36 51.15 49.36
p-Value <0.001 0.001 <0.001
Lengthofthefemoralaxis
Mean 102.48 102.68 114.06 114.39 108.27 108.57
Median 104.30 104.00 115.00 1115.00 107.46 108.00
SD 5.91 6.19 7.79 7.23 9.01 8.93
Min. 88.00 85.40 97.00 97.70 88.00 85.40
Max. 120.00 118.00 132.66 134.00 132.66 134.00
p-Value 0.519 0.047 0.051
Neck-shaftangle
Mean 129.54 128.42 132.38 131.53 130.96 129.98
Median 129.90 128.10 133.40 132.00 130.00 130.00
SD 9.16 5.09 9.39 5.31 9.37 5.43
Min. 120.00 116.70 120.00 118.80 120.00 116.70
Max. 143.60 144.10 146.00 150.00 146.00 150.00
p-Value 0.023 0.103 0.006
Offset
Mean 41.53 41.97 46.54 47.57 44.03 44.77
Median 41.31 42.55 47.00 48.60 44.60 45.00
SD 7.11 6.76 8.33 8.14 8.13 7.98
Min. 30.00 30.00 30.10 32.00 30.00 30.00
Max. 69.10 66.90 68.80 69.13 69.10 69.13
p-Value 0.002 <0.001 <0.001
foundthatthemeanfortherightsidewas24.9mmandfor theleftside,24.3mm.Duthieetal.15analyzedScottish popu-lationsattwodifferenttimesandalsofoundgreaterlengthsof thefemoralneck:34.9mmand38.3mmformenand32.5mm and35mmforwomen.Theyexplainedthisdifferenceinterms ofbetter nutritionduring childhood and changes in living standardsingeneral.
Regardingthe lengthofthefemoralaxis,O’Neillet al.16 evaluatedthis infemalepopulations in1950and 1990and foundvaluesof124mmand136.2mm,respectively.Ina simi-larstudy,Reidetal.19foundvaluesof124.0mmand130.5mm, respectively. Thevalues forthe length ofthe femoral axis foundinthepresentstudyweresmallerthanthoseofthe stud-iesbyO’Neilletal.16andReidetal.19Thisdifferencecanbe explainedbythedifferentmethodologiesused,giventhatin thepresentstudy,thepelvicstructurewasnotincludedinthe analysisofthelengthofthefemoralaxis.Norwasthisdonein thestudybyMourãoandVasconcellos,17whofoundlengths of92.1mmfortherightsideand92.0mmfortheleftside.
Higher valuesfor the width ofthe femoralneck inthe Brazilian population were found here, in comparison with
thestudybyMourãoandVasconcellos,17whosevalueswere 26.7mm(±3.1)fortherightsideand26.3mm(±3.3)forthe leftside.NeitheroftheBrazilianstudiesfoundanysignificant differencesbetweenthesides.O’Neilletal.16observedthat therewasapositivecorrelationbetweenthelengthandwidth ofthefemoralneckandfoundmeasurementsof36.6mmand 39.1mmforthewidthsin1950and1990,respectively.Using similarmethodology,Reidetal.19foundmeanvaluesforthe widthofthefemoralneckof38.1mmfromradiographs per-formedonwomenin1950and38.6mmin1990.Theytherefore concludedthatthewidthofthefemoralneckhadincreased overthecourseoftime.IntheradiographicstudybyCheng etal.,4 themeanvaluesfoundforthelengthofthefemoral neckforbothsexeswere35.1mmfortheleftsideand35.5mm fortherightside.
Table2–Comparisonofthevariablesinrelationto gender.
Left Right
Female Male Female Male
Lengthofthefemoralneck
Mean 34.68 38.54 34.55 38.27
Median 34.00 38.27 33.00 38.20
SD 5.30 4.72 5.42 4.50
Min. 27.40 30.00 25.00 27.00
Max. 49.72 46.82 48.50 47.76
p-Value <0.001 <0.001
Widthofthefemoralneck
Mean 34.81 40.61 34.55 40.16
Median 35.00 40.00 34.72 40.00
SD 3.39 4.24 2.98 3.71
Min. 24.20 31.00 28.60 32.00
Max. 41.16 51.15 41.13 49.36
p-Value <0.001 <0.001
Lengthofthefemoralaxis
Mean 102.48 114.06 102.68 114.39 Median 104.30 115.00 104.00 1115.00
SD 5.91 7.79 6.19 7.23
Min. 88.00 97.00 85.40 97.70
Max. 120.00 132.66 118.00 134.00
p-Value <0.001 <0.001
Neck-shaftangle
Mean 129.54 132.38 128.42 131.53 Median 129.90 133.40 128.10 132.00
SD 9.16 9.39 5.09 5.31
Min. 120.00 120.00 116.70 118.80 Max. 143.60 146.00 144.10 150.00
p-Value <0.001 <0.001
Offset
Mean 41.53 46.54 41.97 47.57
Median 41.31 47.00 42.55 48.60
SD 7.11 8.33 6.76 8.14
Min. 30.00 30.10 30.00 32.00
Max. 69.10 68.80 66.90 69.13
p-Value <0.001 <0.001
theleftside.Silvaetal.18foundvaluesof122.5◦fortheright
sideand125.6◦fortheleftsideandexplainedthisdifference
betweenthe limbs withthe hypothesis that the dominant limb(theonethatwouldbesubjectedtomoreweight-loading) mighthaveasmallerneck-shaftanglethanthecontralateral limb.Inamulticenterprospectivestudyamongwomenover theageof60years,usingDEXA,Faulkneretal.6foundthatthe neck-shaftangleofthecontrolgroupwas126◦.Chengetal.9 foundameanvalueof125◦ inaradiographicstudy onthe
proximalfemur.
Thevaluesfoundfortheoffsetinthepresentstudywere 44.03mmfortheleftsideand44.77mmfortherightside.We didnotfindany reportsinthisregard inthe Brazilian spe-cializedliterature.18,20Ferrisetal.21analyzedthecontralateral femurofpatientswithsubcapitalfractures,transtrochanteric fracturesandosteoporosisandfoundmeanvaluesof43mm (±0.4),38mm(±0.6)and41mm(±0.6),respectively.This differ-encecanbeattributedtothemethodologyused,amongother reasons.
Conclusion
Themeanvaluesofthemainmeasurementsoftheproximal femuroftheseBraziliansdifferedfromthevaluesfoundin previous studies.Therewasastatisticallysignificant mean differencebetweenthemenandwomenforallthevariables, bothontheleftsideandontherightside.Themenpresented highervaluesthanthoseofthewomen.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.LabriciniPJ,AlvesSD,SilvaAF,GiubertiGR,HoffmannR.
Estudoanatômicodoterc¸oproximaldofêmur:impacto
femoroacetabulareoefeitoCAM.RevBrasOrtop.
2009;44(2):120–4.
2.TestutL,LatarjetA.Tratadodeanatomiahumana.Barcelona:
Salvat;1959.
3.TardieuC,DamsinJP.Evolutionoftheangleofobliquityofthe
femoraldiaphysisduringgrowth–correlations.SurgRadiol
Anat.1997;19(2):91–7.
4.PiresRE,PrataEF,GibramAV,SantosL,BellotiJC.Radiographic
anatomyoftheproximalfemur:correlationwiththe
occurrenceoffractures.ActaOrtopBras.2012;20(2):79–83.
5.RubinPJ,LeyvrazPF,AubaniacJM,ArgensonJN,EstèveP,de
RoguinB.Themorphologyoftheproximalfemur.A
three-dimensionalradiographicanalysis.JBoneJointSurgBr.
1992;74(1):28–32.
6.FaulknerKG,CummingsSR,BlackD,PalermoL,GlüerCC,
GenantHK.Simplemeasurementoffemoralgeometry
predictshipfracture:thestudyofosteoporoticfractures.J
BoneMinerRes.1993;8(10):1211–7.
7.PeacockM,TurnerCH,LiuG,ManatungaAK,TimmermanL,
JohnstonCCJr.Betterdiscriminationofhipfractureusing
bonedensity,geometryandarchitecture.OsteoporosInt.
1995;5(3):167–73.
8.QureshiAM,McGuiganFE,SeymourDG,HutchisonJD,Reid
DM,RalstonSH.AssociationbetweenColia1Sp1allelesand
femoralneckgeometry.CalcifTissueInt.2001;69(2):67–72.
9.ChengXG,LowetG,BoonenS,NicholsonPH,BrysP,NijsJ,
etal.Assessmentofthestrengthofproximalfemurinvitro:
relationshiptofemoralbonemineraldensityandfemoral
geometry.Bone.1997;20(3):213–8.
10.XuH,ZhouY,LiuQ,TangQ,YinJ.Femoralmorphologic
differencesinsubtypesofhighdevelopmentaldislocationof
thehip.ClinOrthopRelatRes.2010;468(12):3371–6.
11.BeckTJ,RuffCB,ScottWWJr,PlatoCC,TobinJD,QuanCA.
Sexdifferencesingeometryofthefemoralneckwithaging:a
structuralanalysisofbonemineraldata.CalcifTissueInt.
1992;50(1):24–9.
12.SimmermacherRK,BoschAM,VanderWerkenC.The
AO/Asif-proximalfemoralnail(PFN):anewdeviceforthe
treatmentofunstableproximalfemoralfractures.Injury.
1999;30(5):327–32.
13.SiskTD.Fracturesofhipandpelvis.In:CrenshawAH,editor.
Campbell’soperativeorthopaedics.7thed.St.Louis:Mosby;
1987.p.1719–28.
14.IsaacB,VettivelS,PrasadR,JeyaseelanL,ChandiG.Prediction
ofthefemoralneck-shaftanglefromthelengthofthe
15.DuthieRA,BruceMF,HutchisonJD.Changingproximal
femoralgeometryinnortheastScotland:anosteometric
study.BMJ.1998;316(7143):1498.
16.O’NeillTW,GrazioS,SpectorTD,SilmanAJ.Geometric
measurementsoftheproximalfemurinUKwomen:secular
increasebetweenthelate1950sandearly1990s.Osteoporos
Int.1996;6(2):136–40.
17.MourãoAL,VasconcellosHA.Geometriadofêmurproximal
emossosdebrasileiros.ActaFisiátrica.2001;8(3):113–9.
18.SilvaVJ,OdaJY,Sant’anaDM.Anatomicalaspectsofthe
proximalfemurofadultsBrasilians.IntJMorphol.
2003;21(4):303–8.
19.ReidIR,ChinK,EvansMC,JonesJG.Relationbetween
increaseinlengthofhipaxisinolderwomenbetween1950s
and1990sandincreaseinagespecificratesofhipfracture.
BMJ.1994;309(6953):508–9.
20.CaetanoEB,SerafimAG,PadovezeEH.Studyofthe
collo-diaphysealangleofthefemurofcorpsesinthe
anatomydepartmentofthePUC-SPmedicalschool.
IntJMorphol.2007;25(2):285–8.
21.FerrisBD,KennedyC,BhamraM,Muirhead-AllwoodW.
Morphologyofthefemurinproximalfemoralfractures.