rev bras hematol hemoter. 2015;37(5):287–289
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Scientific
Comment
The
importance
of
hemoglobin
A
2
determination
夽
Maria
Stella
Figueiredo
∗UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received24June2015 Accepted7July2015 Availableonline21July2015
Hemoglobin(Hb)A2(␣2␦2)constituteslessthan3%ofthetotal
hemoglobin(Hb)inadultsand hasalmostnophysiological importance.1Ontheotherhand,thedeterminationofHbA
2
isanimportanttooltodiagnosethe beta-thalassemia trait (BTT).1,2 Althoughindividuals with BTTdonotneed treat-ment,theaccuratedetectionofthecarrierstateisimportant ingeneticcounselingtodetermineriskofhavingachildwith amajordisease.3
ElevatedlevelsofHb A2andmicrocytosis aresuggestive
ofthediagnosisofBTT.However,BTTmaybepresent with normallevelsofHbA2 asafewcasesof-thalassemiaare
notassociatedwithelevatedHbA2,andbecauseofthe
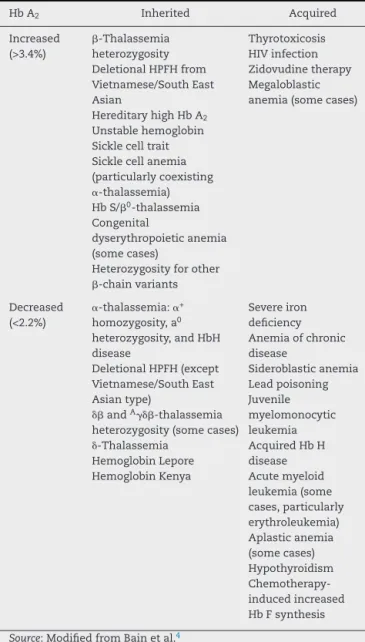
asso-ciation of BTT with iron deficiency or with ␣-thalassemia (␣-Thal).1,2,4–6 There are many other factors, inherited or acquired,thatcaninterfereinHbA2levels(Table1).3,4
HbA2canbemeasuredbyseverallaboratorialmethods,but
thesemethodshavedifferencesinaccuracy.7Cationexchange high performanceliquid chromatography(HPLC), microcol-umnchromatography,andcelluloseacetateelectrophoresis withelutionareconsideredacceptablemethodstodiagnose BTT,whereas celluloseacetate electrophoresis followed by scanning densitometry is not.2 The accuracy of cellulose acetateelectrophoresis withelution dependson the train-ingandexperienceofthelaboratorytechnicianwhoperforms
夽
SeepaperbyFonsecaetal.onpages296–301.
∗ Correspondenceto: Hematology andBlood TransfusionDivision, Escola Paulista de Medicina,UniversidadeFederal de SãoPaulo (UNIFESP),RuaDr.DiogodeFaria,824,0437-002SãoPaulo,SP,Brazil.
E-mailaddress:[email protected]
thetest,andmicrocolumnchromatographycangiveproblems withco-elutionofsomeHbvariants.7
Recentstudieshaveconfirmedthehigherqualityof auto-matedHPLCinthemeasurementofHbA2comparedtothe
othermethods,8,9whichiswhythishasbecomethemethod ofchoice.Ontheotherhand,inautomatedHPLC,the mea-surementofHbA2 isinaccuratewhenHbSispresent.2,3,10
AstheamountofHbSisrelatedtothedegreeofinaccuracy, levelsarehigherinpatientswithsicklecellanemia(SCA)or HbS/-thalassemia(S-Thal)thaninsicklecelltrait.2Thus, theamountofHbA2doesnotindicateBTTwhenHbAand
betagenevariantsarefoundtogether.11Furthermore,when betagenevariantsarepresentwithoutHbA,thediagnosisof concomitantBTTisnotnecessarilyassociatedtotheelevation ofHbA2andsofurtherinvestigationsusingfamilystudiesor
DNAanalysisarenecessary.10
Asmentionedabove,␣-Thaliscapableofinterferinginthe determinationofHbA2.4Individualswiththe␣0-thalassemia
traitorhomozygousfor␣+-thalassemiahavelowerlevelsof HbA2,buttheinfluenceofthecoinheritanceof␣-Thal and
BTTonHbA2levelsisuncertain.6
InBrazil,theincidenceof␣-Thalvariesfrom0.11to0.22% dependingonthegeographicalregionstudied.12–15Itiswell knownthattheassociationof␣-ThalandSCAiscommonin
http://dx.doi.org/10.1016/j.bjhh.2015.06.002
288
revbrashematolhemoter.2015;37(5):287–289Table1–Causesofvariationinthepercentageof hemoglobinA2.
HbA2 Inherited Acquired
Increased (>3.4%)
-Thalassemia heterozygosity DeletionalHPFHfrom Vietnamese/SouthEast Asian
HereditaryhighHbA2
Unstablehemoglobin Sicklecelltrait Sicklecellanemia (particularlycoexisting
␣-thalassemia) HbS/0-thalassemia Congenital
dyserythropoieticanemia (somecases)
Heterozygosityforother
-chainvariants
Thyrotoxicosis HIVinfection Zidovudinetherapy Megaloblastic anemia(somecases)
Decreased (<2.2%)
␣-thalassemia:␣+
homozygosity,a0
heterozygosity,andHbH disease
DeletionalHPFH(except Vietnamese/SouthEast Asiantype)
␦andA␥␦-thalassemia
heterozygosity(somecases)
␦-Thalassemia HemoglobinLepore HemoglobinKenya
Severeiron deficiency Anemiaofchronic disease Sideroblasticanemia Leadpoisoning Juvenile myelomonocytic leukemia AcquiredHbH disease Acutemyeloid leukemia(some cases,particularly erythroleukemia) Aplasticanemia (somecases) Hypothyroidism Chemotherapy-inducedincreased HbFsynthesis
Source:ModifiedfromBainetal.4
Hb A2 – hemoglobin A2; HPFH: hereditary persistence of
fetal hemoglobin; HIV: human immunodeficiency virus; HbH: hemoglobinH;HbF:hemoglobinForfetalhemoglobin.
Brazil.16–18SinceSCAisconsideredapublichealthproblemin Brazilandduetotheclinicalsignificanceof␣-Thalinrespect tothisanemia,diagnosisisimportant.19–21However,diagnosis ismainlyachievedbymoleculartechniquesthatareexpensive andnoteasilyaccessible.Itisalsoimportanttoremember thattheco-inheritanceof␣-ThalandSCAresultsinincreased levelsofHbA2 asmeasuredbyautomatedHPLC,andcould
resultinamisdiagnosisofS-Thal.4
There lies the importance of the paper entitled “Hemoglobin A2 values quantified by high performance
liquid chromatography inpatients with sickle cell disease, and the influence of the presence of alpha-thalassemia” written by Fonseca et al. and published in this edition of theRevistaBrasileiradeHematologiaeHemoterapia.22 The authorsdemonstratethatHbA2wasoverestimatednotonly
inindividualswithHbSbutalsoinpatientswithHbC,and thattheHbA2levelwasinfluencedbythegenotypeof␣-Thal.
In conclusion, ina country with a high degree of mis-cegenation suchasBrazil,notonlythediagnosis ofdouble heterozygousstates,suchasS-Thal,butalsothediagnosisof co-inheritanceofSCAwith␣-Thalshouldbecarriedout care-fully,takingintoconsiderationthelimitationsoftheavailable laboratorytechniques.FamilystudiesorDNAanalysis,when possible,aredesirabletoconfirmthecorrectdiagnosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.SteinbergMH,AdamsJG.HemoglobinA2:origin,evolution,
andaftermath.Blood.1991;78(9):2165–77.
2.HeadCE,ConroyM,JarvisM,PhelanL,BainBJ.Some observationsonthemeasurementofhaemoglobinA2andS
percentagesbyhighperformanceliquidchromatographyin thepresenceandabsenceofalphathalassaemia.JClin Pathol.2004;57(3):276–80.
3.GiambonaA,PassarelloC,RendaD,MaggioA.The significanceofthehemoglobinA(2)valueinscreeningfor hemoglobinopathies.ClinBiochem.2009;42(18):1786–96.
4.BainBJ,WildBJ,StephensAD,PhelanLA.Variant
hemoglobins:aguidetoidentification.1sted.WestSussex, UK:Wiley-Blackwell;2010.
5.Saleh-GohariN,KhademiBamiM,NikbakhtR,Karimi-Maleh H.Effectsofalpha-thalassaemiamutationsonthe
haematologicalparametersofbeta-thalassaemiacarriers.J ClinPathol.2015;68(7):562–6.
6.DenicS,AgarwalMM,AlDabbaghB,ElEssaA,TakalaM, ShowqiS,etal.HemoglobinA2loweredbyirondeficiencyand
alpha-thalassemia:shouldscreeningrecommendationfor beta-thalassemiachange?ISRNHematol.2013;2013:858294.
7.ColahRB,SurveR,SawantP,D’SouzaE,ItaliaK,
PhanasgaonkarS,etal.HPLCstudiesinhemoglobinopathies. IndianJPediatr.2007;74(7):657–62.
8.AnagnostopoulosK,TentesI,KalleasC,MargaritisD,ToliA, PendilasD,etal.EffectofHbSinthedeterminationofHbA2
withtheMenariniHA-8160analyzerandcomparisonwith otherinstruments.IntJLabHematol.2009;31(6):665–72.
9.PaleariR,GulbisB,CottonF,MoscaA.Interlaboratory comparisonofcurrenthigh-performancemethodsforHbA2.
IntJLabHematol.2012;34(4):362–8.
10.ShokraniM,TerrellF,TurnerEA,AguinagaMD.
ChromatographicmeasurementsofhemoglobinA2inblood
samplesthatcontainsicklehemoglobin.AnnClinLabSci. 2000;30(2):191–4.
11.GiordanoPC.Editorial:measurementofHbA2.IntJLab
Hematol.2012;34(4):335.
12.SilvaCdeA,BaldimLB,NhoncanseGC,EstevaoIdaF,Melo DG.NeonatalscreeningforhemoglobinopathiesinSao Carlos,SaoPaulo,Brazil:analysisofaseriesofcases.RevPaul Pediatr.2015;33(1):19–27.
13.deMedeirosAlcoforadoGH,BezerraCM,AraújoMouraLemos TM,deOliveiraDM,KimuraEM,FerreiraCostaF,etal. Prevalenceofalpha-thalassemia3.7kbdeletionintheadult populationofRioGrandedoNorte,Brazil.GenetMolBiol. 2012;35(3):594–8.
revbrashematolhemoter.2015;37(5):287–289
289
determinantsinsouthBrazil:importanceforthediagnosisof microcyticanemia.GenetMolBiol.2010;33(4):641–5.
15.AdornoEV,CoutoFD,MouraNetoJP,MenezesJF,RêgoM,Reis MG,etal.HemoglobinopathiesinnewbornsfromSalvador, Bahia,NortheastBrazil.CadSaudePublica.2005;21(1): 292–8.
16.LyraIM,Gonc¸alvesMS,BragaJA,GesteiraMdeF,CarvalhoMH, SaadST,etal.Clinical,hematological,andmolecular characterizationofsicklecellanemiapediatricpatientsfrom twodifferentcitiesinBrazil.CadSaudePublica.
2005;21(4):1287–90.
17.FigueiredoMS,KerbauyJ,Gonc¸alvesMS,ArrudaVR,SaadST, SonatiMF,etal.Effectofalpha-thalassemiaandbeta-globin geneclusterhaplotypesonthehematologicalandclinical featuresofsickle-cellanemiainBrazil.AmJHematol. 1996;53(2):72–6.
18.DeLemosCardosoG,GuerreiroJF.Molecularcharacterization ofsicklecellanemiaintheNorthernBrazilianstateofPara. AmJHumBiol.2010;22(5):573–7.
19.dePaivaeSilvaRB,RamalhoAS,CassorlaRM.Sicklecell diseaseasapublichealthprobleminBrazil.RevSaude Publica.1993;27(1):54–8.
20.DomingosIF,FalcãoDA,HatzlhoferBL,CunhaAF,SantosMN, AlbuquerqueDM,etal.Influenceofthebetashaplotypeand alpha-thalassemiaonstrokedevelopmentinaBrazilian populationwithsicklecellanaemia.AnnHematol. 2014;93(7):1123–9.
21.Camilo-AraujoRF,AmancioOM,FigueiredoMS, Cabanas-PedroAC,BragaJA.Molecularanalysisand associationwithclinicalandlaboratorymanifestationsin childrenwithsicklecellanemia.RevBrasHematolHemoter. 2014;36(5):334–9.
22.FonsecaSF,AmorimT,Purificac¸ãoA,GoncalvesMS,Boa-Sorte N.HemoglobinA2valuesquantifiedbyhighperformance