Arq Neuropsiquiat r 2005;63(3-B):757-760
1Laborat ório de Neurociências. Núcleo de Pesquisas Tecnológicas/ Universidade de M ogi das Cruzes (NPT/UM C), M ogi das Cru z e s ,
S P, Brasil; 2Laborat ório de Neurologia Experimental. Universidade Federal de São Paulo/Escola Paulista de M edicina (UNIFESP/EPM ),
São Paulo SP, Brasil; 3Inst it ut o de Nef rologia de M ogi das Cruzes, SP, Brasil: FA E P, PRONEX, CNPq, and FAPESP support ed t his w ork.
Received 21 February 2005, received in f inal f orm 5 M ay 2005. Accept ed 16 June 2005.
Dr. Fulvio Alexandre Scorza - Rua Botucatu 862 / Disciplina de Neurologia Experimental UNIFESP - 04023-900 São Paulo SP - Brasil. E-mail: [email protected]
Epilepsy is charact erized by chronic re c u rre n t p a roxysmal changes in neurological functions c a u s e d by abnormalit ies in the electrical activity of the b r a-i n1. As epilepsy is considered to involve hypere x c i t
a-ble neurons, a basic assumption in epilepsy re s e a rc h links t he pat hogenesis of epilepsy and t he gener-ation of synchronized neuronal act ivity w it h an i m-balance bet w een inhibit ory [g-aminobut yric acid (GABA)-mediated] and excitatory
(glutamate-medi-ated) neurotransmission in f avor at the latt er2.
Ap-p roximately 2 million Ap-persons in t he Unit ed St at es have epilepsy3 , 4and each year, 100,000 new cases o f
epilepsy are diagnosed in the Unit ed St at es3 , 5. The
most commonly re p o rted etiological factors are s t ro-ke, t umors, alcohol, head injuries, congenit al f ac-t ors and neuro i n f e c ac-t i o n s6. In Brazil, neurocyst
icer-cosis is t he most f requent ly identif ied cause of epi-l e p s y7. Bergen and colleagues8re p o rted an
estima-SEIZURE OCCURRENCE IN PATIENTS WITH
CHRONIC RENAL INSUFFICIENCY IN
REGULAR HEMODIALYSIS PROGRAM
Fulvio Alexandre Scorza
1,2, Marly de Albuquerque
1,2, Ricardo Mario Arida
1,2,
Roberta Monterazzo Cysneiros
2, Tânia Maria Guedes Henriques
1,
Carla Alessandra Scorza
2, Jener Cruz
3, Silvana Kesrouani
3,
Rui Alberto Gomes
3, Esper Abrão Cavalheiro
2ABSTRACT - Hemodial ysis-associat ed seizure is a complicat ion of hem odialysis. This re p o rt describes t he occurrence of seizures in patients wit h end st age renal disease on dialysis t herapy at t he Nephrology Inst itu-t e of Mogi das Cruzes, São Paulo Situ-t aitu-t e, Brazil. A re itu-t rospecitu-t ive medical hisitu-tory of 189 paitu-t ienitu-t s w as re v i e w e d t o invest igat e t he occurrence of convulsive seizures during dialyt ic program. Seven pat ient s w it h hist ory of seizures w ere select ed but f ive of t hem w ere included in our st udy. Three pat ient s present ed generali-zed t onic-clonic seizures, one had partial seizure w ith secondary generalization, and one presented unclassi-f ied seizure. Three pat ient s present ed seizure just dur ing t he dialysis (unique seizure) and one ounclassi-f t hem p resented convulsive st at us epilept icus. The t w o ot her pat ient s had already present ed seizures prior t he beginning of dialysis. We conclude t hat seizures in renal f ailure could be considered as occasional event s t hat do not usually become chronic.
KEY WORDS: seizures, epilepsy, dialysis, renal f ailure.
O c o rrência de crises epilépticas em pacientes com insuficiência renal crônica em pro g r a m a dialítico regular
RESUM O - Convulsões durant e o t rat ament o dialít ico podem const it uir uma complicação da hemodiálise. Esse art igo descreve a ocorrência de crises em pacient es em est ágio f inal de insuf iciência renal crônica sob t rat ament o dialít ico no Inst it ut o de Nef rologia de M ogi das Cruzes, São Paul o, Brasil. Foram revist os os p ront uários de 189 pacientes, com o objet ivo de invest igar a ocorrência de crises convulsivas durant e o t ra-t amenra-t o dialíra-t ico. Dos sera-t e pacienra-t es selecionados com hisra-t ória de crises, cinco concordaram em parra-t i c i p a r de nosso est udo. Três pacientes apresentaram crises generalizadas tônico-clônicas, um apresent ou crise p a r-cial com generalização subseqüent e e um apresentou crise inclassificada. Três pacient es apresent aram crises apenas durant e o processo dialítico (crise única) sendo que um deles apresent ou st at us epilept icus convulsi-vo. Os out ros dois pacient es já haviam apresent ado crises ant es do início do t rat ament o dialít ico. Nós con-cluímos que as crises convulsivas que ocorrem em pacientes com falência renal podem ser consideradas c o m o event os ocasionais e que usualment e não se t ornam crônicas.
758 Arq Neuropsiquiat r 2005;63(3-B)
t ed incidence of seizure of approximat ely 10% in patients w it h chronic renal failure. M ore o v e r, Plum and Posner9also not ed t hat convulsions occurred
in one third of patients with end-stage renal dise a s e (ESRD) and was frequently a pre t e rminal event. T h e s e i z u res in t hese series usually w ere generalized tonic-clonic type, how ever, the mechanism of re d u-ced seizure threshold in renal failure is still u n k n o w n . Hemodialysis-associat ed seizure (HAS) is a com-m on cocom-mplicat ion of hecom-modialysis1 0. HAS occurs
in 7% to 50% of children w ith ESRD, and their sei-z u res are usually re p o rted as generalisei-zed t oni c-clonic seizure s1 1. On the ot her hand, non-convuls i v e
s e i z u res appear t o be rare1 2 , 1 3. Risk f actors f or HAS
include young age, prior hist ory of seizures, malig-nant hypertension, microvascular diseases, ure m i c encephalopathy and card i o m y o p a t h y. M ore o v e r, i n-duced brain w at er disequilibrium, hypocalcaemia, uremic t oxins, t he use of acet at e in t he dialysat e, int racranial hemorrhage due t o syst emic heparini-zation, treat ment w ith recombinant ery t ro p o i e t i n , hem odinam ic and m et ab olic def ect s, and dru g s such as penicillin and theophilline are also conside-red responsible f or HAS1 1 , 1 4 , 1 5. The eff icacy of ant
i-convulsant drugs in t reat ing or prevent ing HAS is not w ell def ined1 0 , 1 6. Diazepam is a non-dialyzable
ant iconvulsant dru g1 7and t he administ rat ion of
oral diazepam (0.3-0.5 mg/kg per dose) 30 minu-t es bef ore each hemodialysis session may help minu-t o p revent re c u rrence of HAS1 0. On t he ot her hand,
readily dialyzable ant iepilept ic drugs such as phe-nobarbital may increase the risk of HAS1 6 , 1 8. Despite
t hese observat ions, several lines of evidence sup-p o rt the idea that anaemia is one of t he major lim-it at ions t o reh abi llim-it at ion i n pat ient s w i t h ESRD. The efficacy of recombinant human erit hro p o i e t i n in t he t reat ment of renal anaemia is w ell est abli-shed. How ever, this therapeut ic approach has been associated with serious untow ard eff ect s: incre a s e d risk of hypertension, not infrequently accompan i e d by hypert ensive encephalopat hy and seizure s1 9 , 2 0.
Based on t hese f act s, t he aim of our st udy w as to investigate the occurrence of seizures in patients w it h ESRD under regular hemodialysis program.
METHOD
A re t rospect ive medical hist ory of 189 pat ient s w as review ed t o in vest i g at e t h e o ccu rrence o f co nvu lsive s e i z u res in dialysis pat ient s at t he Nephrology Inst it ut e of Mogi das Cruzes. From 189 patients under dialytic tre a t-ment , 7 had suff e red some type of convulsive seizure and w e re invited t o part icipate in t he study, but only 5 patients had agreed t o part icipat e. They w ere 4 males and 1 f
e-male, wit h a mean age of 42 years (range 20 t o 72 years old). The f ive patient s have severe systemic arterial hyper-t ension and w ere using anhyper-t ihyperhyper-t ensive drugs. In our clinic, all patient s have monthly evaluat ion of t ot al cal-cium and were receiving aluminum hydroxide. The solu-t ion for solu-t he dialysolu-t ic solu-t reasolu-t mensolu-t consolu-t ains 0.89 gr. of NaCl/5 L, wit h a calcium concent rat ion of 3.5 mEq/L.
All pat ient s w ere evaluat ed for init ial disease, dura-t ion, dura-type and f requency of HAS and dura-t hen submidura-tdura-t ed dura-to clinical and neurological examinat ion. The mean t ime o f dialysis treat ment and t he elect roencephalography (EEG) w as analysed in all pat ient s. The seizures w ere classified a c c o rding the Commission on Classification and Te rm i n o-logy of Int ernational League Against Epilepsy2 1. The
pos-sible seizure t riggering fact ors, such as the use or w ith-draw al of medications, sleep deprivation, art erial hyper-t ension, inf echyper-t ions, and elechyper-t rolyhyper-t ic misbalance, especial-ly hypocalcaemia, w ere also invest igat ed.
RESULTS
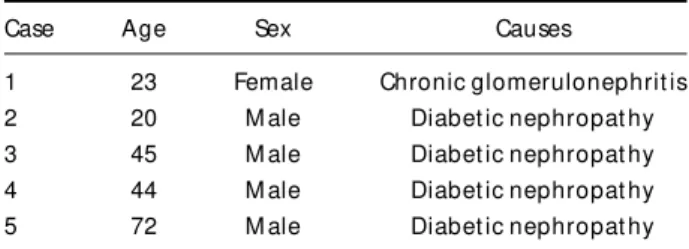
In our st udy w e analyzed t he dat a of 5 out of 189 pat ient s re c ruit ed under dialyt ic t reat ment at t he Nephrology Inst it ute of M ogi das Cruzes. All 5 pat ient s had severe syst emic arterial hypert e n s i o n and w ere using ant ihypert ensive drugs. These pa-t ienpa-t s w ere also using anpa-t iepilep pa-t ic drug (pheni-t oin 200 mg/daily) and CaCO3 (1500 mg/daily). The mean age of beginning of dialysis was 25 years. T h e mean durat ion of dialyt ic t reat ment w as 5.8 years (range 2 t o 12 years). The causes of renal f ailu re w e re diabet ic nephropat hy (4 patient s) and chro n-ic glomerolonephrit is (1 pat ient ) (Table 1). All pa-t ienpa-ts had normal aluminum plasma levels and w e-re not aff ected by ot her clinical pictue-res t hat could be led t o possible aluminum intoxication. The signs of Chvost ek and Trousseau w ere absent in all pa-t ienpa-t s and pa-t he neurological examinapa-t ion w as nor-mal in 4 patients, but one presented pyramidal s y n-d r om e (lef t h em ip aresia w i t h pyram i n-dal sig ns), w it h abnormal CT scan (hipodensit y on right t em-poral lobe).
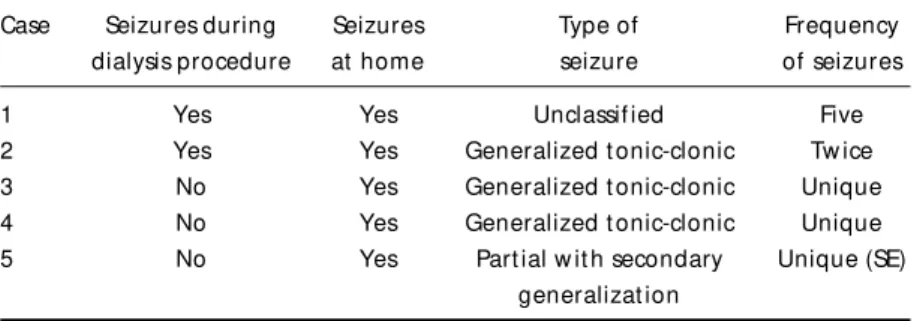
The seizure hist ory of t he f ive pat ient s is list ed on Table 2. Brief ly, three pat ient s present ed gene-ralized t onic-clonic seizures, one presented part i a l
Table 1. Causes of renal failure.
Case Age Sex Causes
1 23 Female Chronic glomerulonephrit is
2 20 M ale Diabet ic nephropat hy
3 45 M ale Diabet ic nephropat hy
4 44 M ale Diabet ic nephropat hy
Arq Neuropsiquiat r 2005;63(3-B) 759
s e i z u re. w it h secondary g eneralizat ion, and one p resent ed unclassif ied seizure. All patient s had sei-z u res at home, t w o pat ient s had seisei-zures during dialysis p ro c e d u re and one of t hem had pre s e n t -ed convulsive st at us epilept icus. Tw o pat ient s had a l ready present ed seizures prior t he beginning of dialysis treatment; one of them w it hout detectable s t ruct ural cent ral n ervous syst em lesion, and t he ot her show ed hipodensit y on right t emporal lobe (vascular cerebral disease). All pat ient s pre s e n t e d n o rmal int erict al EEG. At t ime of seizure, none of t hem present ed inf ect ion, elect rolyt ic misbalance (hypocalcemia), sleep deprivat ion or w er e using t heop hi l l in . Al l p at i en t s h ad an em ia an d w ere using erit hropoet in.
DISCUSSION
Our st udy evaluat ed t he occurrence of seizure s in patients w ith ESRD under hemodialysis pro g r a m . It has long been believed t hat seizures are re l a t i v e-ly common events among patients with systemic d i-seases. HAS are commonly caused by met abolic e n-c e p h a l o p a t h y, h ypert ensive n-crisis, in f en-ct ion, an d dialysis disequilibrium1 3. We observed the occurre
n-ce of HAS in only 2% of our pat ient s. In t his w ay, our data are not in agreement w ith previous studi-es, w hich related an estimated incidence of seizure of approximat ely 10% in patient s w it h chronic re-nal f ailure8.
The mechanism of reduced seizure t hre s h o l d in renal f ailure is unknow n. One possibilit y is t he presence of proconvulsive met abolit es, including guanidinosuccinic acid, creat inine, and creat ine in human subjects2 2. M ore o v e r, t he epilept ogenic
po-t ency of po-t hese compounds w as f urpo-t her supporpo-t e d by animal st udies23.
In spit e of report s t hat prior hist ory of seizure did inf luence t he risk of seizures among pat ient s receiving hemodialysis1 1, w e did not observe
high-er risk in our patients w ho had prior hist ory of
epi-l e p s y. It is dif f icuepi-lt t o make comparisons bet w een our w it h ot her st udies since diff e rent f act ors may inf luence t he analysis, such as t he age of t he sub-ject s, t ype of seizures and risk f act ors f or HAS as previously ment ioned.
It has lo ng been believed t hat in t he absence of prior clinically detected stroke, hypertension, p a r-t icularly severe and unconr-t rolled; increase r-the risk of unprovoked seizures in older individuals2 4.
Con-v e r s e l y, some st udies did not f in d an associat ion betw een hypertension and seizures in the absence of clinically detected stro k e2 5 , 2 6. In addition,
hyper-t ension per se can induce alhyper-t erahyper-tions in hyper-the human brain m orphology2 7, in creasing t he risk f or clin
i-cally apparent brain dysf unction (e.g. epilepsy). In t his w ay, despit e a high prevalence of hypert e n s i-ve diseases in p at ient s w it h ESRD and t he stro k e been one of the commonly re p o rted etiological f a c-t ors, jusc-t one of our pac-t ienc-t s c-t hac-t presenc-t ed seizu-res had preceding cerebrovascular st roke.
It has also been observed t hat anaemia is one o f t he major limit at ions t o rehabilit at ion in pat ient s w it h ESRD and the efficacy of recombinant human e r i t h ropoiet in in t he t reat ment of t his condit ion is w ell established. All our patients presented anae-mia and w ere using erit hropoet in. This t herapeu-t ic approach has been associaherapeu-ted w iherapeu-th seizures and could just if y t he seizures in our pat ients t hat w ere using erit hropoet in19,20.
At t he present moment , t he eff icacy of ant ie-pileptic drugs in t reat ing or preventing HAS is not w ell def ined. How ever, t he administ rat ion of oral diazepam, a non-dialyzable drug, (0.3 - 0.5 mg/kg per dose) 30 minut es before each hemodialysis ses-sion has been shown t o prevent t he re c u rrence of H A S1 6. In our st udy, all pat ient s w ere using
pheni-t oi n (200 m g /d ai ly) w hi ch i s i n agreem enpheni-t w ipheni-t h Rust and Chun16, w ho demonst rat ed t hat t he use
of phenobarbit al, a dialyzable drug, did not pre-vent t he HAS.
Table 2. Seizure history.
Case Seizures during Seizures Type of Frequency dialysis procedure at home seizure of seizures
1 Yes Yes Unclassif ied Five
2 Yes Yes Generalized t onic-clonic Tw ice
3 No Yes Generalized t onic-clonic Unique
4 No Yes Generalized t onic-clonic Unique
5 No Yes Part ial w it h secondary Unique (SE)
760 Arq Neuropsiquiat r 2005;63(3-B)
We conclude t hat seizures in r enal f ailure can be considered as an occasional event s t hat do not usually become chronic and information on the m a-nagement of seizures in renal failure should be d i s-seminat ed among prof essionals t reat ing syst emic diseases.
Acknowledgments – The au t h o rs w ou ld li ke t o t hank Dr. Paulo Gomes (Universit y of M ogi das Cruzes) f or his suggest ions.
REFERENCES
1. Dichter MA. Emerging insights into mechanisms of epilepsy: implica-tions for new antiepileptic drug development. Epilepsia 1994;35(Suppl 4):S51-S57.
2. Dalby NO, Mody I. The process of epileptogenesis: a pathophysiologi-cal approach. Curr Opin Neurol 2001;14:187-192.
3. Annegers JF. Epidemiology of epilepsy. In Wyllie E, (ed). The tre a t m e n t of epilepsy: principles and practice, 2nd ed. Baltimore: Williams & Wi l-kins, 1997:165-172.
4. Hauser WA, Hesdorffer DC. Epilepsy: fre q u e n c y, causes and consequen-ces. New York: Demos, 1990.
5. Begley CE, Annegers JF, Lairson LB, Reynolds TF. Epilepsy incidence, p rognosis, and use of medical care in Houston, Texas, and Rochester, Minnesota. Epilepsia 1998;39(Suppl 6):S222.
6. Halatchev VN. Epidemiology of epilepsy: recent achievements and fu-ture. Folia Med (Plovdiv) 2000;42:17-22.
7 . Basch EM, Cruz ME, Tapia D, Cruz A. Prevalence of epilepsy in a migrant population near Quito, Ecuador. Neuroepidemiology 1997;16:94-98. 8. B e rgen DC, Ristanovic R, Gorelick PB, Kathipalia S. Seizures and re n a l
failures. Int J Artif Organs 1994;17:247-251.
9 . Plum F, Posner JB. Metabolic brain diseases causing coma. In Plum F, Pos-ner JB (eds). The diagnosis of stupor and coma. Philadelphia: Davis, 1972. 10. Sönmez F, Mir S, Tütüncüoglu S. Potential prophylatic use of benzodia-zepines for hemodialysis-associated seizures. Pediatr Nephrol 2000; 14:367-369.
11. Glenn CM, Astley SJ, Watkins SL. Dialysis associated seizures in chil-dren and adolescents. Int J Pediatr Nephrol 1992;6:182-186.
12. Tanimu DZ, Obeid T, Awada A, Huaib S, Igbal A. Absence status; an overlooked cause of acute confusion in hemodialysis patients. J Nephro l 1998;11:146-147.
13. Chow KM, Wang AY, Hui AC, Wong TY, Szeto CC, Li PK. Noncon-vulsive status epilepticus in peritoneal dialysis patients. Am J Kidney Dis 2001;38:400-405.
14. Swash M, Rowan AJ. Electroencephalographic criteria of hypocalcemia and hypercalcemia. Arch Neurol 1972;26:218-228.
15. Schwartz RD. Hemodialysis associated seizures. In Nissensen AR, Fine RN (EDS) Dialysis therapy. Philadelphia Hanley Balfus, 1993:88-90. 16. Rust RS, Chun WMR. Interrelationships between renal and neuro l o
g-ic diseases and therapies. In Swaiman KF, (ed). Pediatrg-ic neuro l o g y : Baltimore: Mosby, 1994:815-816.
17. Sinaiko AR, O’ Dea RF. Use of drugs in renal insuff i c i e n c y. In Edelmann CM, (ed). Pediatric kidney disease. Boston Little Brown, 1993:991-993. 18. Burwen DR, Olsen SM, Bland LA, A rchino MJ, Reid MH, Jarvis, WR. Epidemic aluminium intoxication in hemodialysis patients traced to use of an aluminium pump. Kidney Int 1995;48:469-474.
19. Massetani R, Galli R, Calabrese R, Sartucci F, Rindi P, Severino B, Murri L. Status epilepticus in chronically dialyzed patients treated with ery-thropoietin. Riv Neurol 1991;61:215-218.
20. Beccari M. Seizures in dialysis patients treated with recombinant ery-t h ropoieery-tin: review of ery-the liery-teraery-ture and guidelines for prevenery-tion. Inery-t J Artif Organs 1994;17:5-13.
2 1 . Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for revised clinical and electro e n c e p h a l o g r a p h-ic classifh-ication of epilepth-ic seizures. Epilepsia 1981;22:489-501. 22. De Deyn PP, Mac Donald RR. Guanidino compounds that are incre a s e d
and cere b rospinal fluid in brain of uraemic patients inhibit GABA a n d glycine responses on mouse neurons in cell culture. Ann Neurol 1990; 28:627-633.
2 3 . D’Hooge R, Pei YQ, Marescau B, De Deyn PP. Convulsive action and to-xicity of uremic guanidino compounds: behavioral assessment and re-lation to brain concentration in adult mice. J Neurol Sci 1992;12:96-105. 24. H e s d o r ffer DC, Hauser WA, Annegers JF, Rocca WA. Severe, uncontro
l-led hypertension and adult-onset seizures: a case-control study in Ro-chester, Minnesota. Epilepsia 1996;37:736-741.
25. Ng SK, Hauser WA, Brust JC, Susser M. Hypertension and the risk of new-onset unprovoked seizures. Neurology 1993;43:425-428. 2 6 . S h a p i ro IM, Neufeld MY, Korczyn AD. Seizures of unknown origin