Vol-7, Special Issue-Number4-June, 2016, pp845-853
http://www.bipublication.com
Case Report
The Effectiveness of Group Mindfulness Training on the Quality of Life
among Patients with PTSD Caused by the War in the East Azerbaijan
Province
Naimeh Yousefi and Vida Mohammadi Heris* Department of Psychology,
Tabriz Branch, Islamic Azad University, Tabriz, Iran
ABSTRACT
Purpose: since the quality of family life is critical in multiple dimensions and stress of life both mentally and physically have major effect on humans. Having a partner with post-traumatic stress disorder (PTSD) affects the quality of life and increases the stress among couples. A major problem in this research is that if group mindfulness training can enhance the quality of life among spouses with Post-traumatic stress disorder (PTSD) or not.
Methodology: In this study, 15 participants were randomly assigned to the experimental group and 15 participants were in the control group and the World Health Organization Quality of Life Questionnaire was used to gather the related data.
Findings: After 8 sessions the results showed that group mindfulness training techniques increased the quality of life in all its dimensions except social function.
Keywords: quality of life, group mindfulness training, Post-traumatic stress disorder (PTSD)
INTRODUCTION
Human life from birth to death is facing with a lot of phenomena and events.Some of these phenomena are associated with problems having devastating effects on the individual and some damage to the status of the community which can sometimes exceed the tolerance level of individuals and led to a series of physical and mental disorders. War is one of those phenomena that problems and consequences of which can damage both the individual and the community and its effects are over the tolerance level of society. One of the most important problems of war for the people involved with it is Post-traumatic stress disorder or PTSD which is associated with unpredictable, devastating and long-term consequences for the injured person, his family and social lives of their relatives (1). Post-traumatic stress disorder is one of the anxiety disorders which occur following exposure to traumatic life events and is composed of three categories of symptoms:
adverse effects of war continues on families, especially their husbands (4).
Usually people who are suffering from PTSD have irritability, alert in the extreme, are shy and have confused dreams that harm their social relations. Marital conflicts, lack of job satisfaction, expressions of hopelessness, helplessness and feeling constantly threatened is observed among them. According to Carole, marital satisfaction (5) is compatibility in marriage meaning happy, being satisfied and satisfy the mutual needs. Compatible couples are the wives and husbands with lot of agreement with each other, satisfied with the type and level of relationships, have satisfaction about the quality of leisure time and manage their time and coordinate financial issues (6).
Family is the only institute that communicates the emotional connection between the couple, personal safety, satisfaction, strengthen and the purposefulness of life, empowerment and socialization in their environment with the members and future generations. In families of veterans with PTSD, the functions are impaired and in practice this institution cannot function properly.Studies on the symptoms of PTSD have shown that these symptoms can influencethe family relationships and in some cases, spouses of veterans feel helplessly. As the situation is prolonged with impaired veterans, the wife and her family would have serious psychological trauma (6).
Diagnostic criteria for PTSD based on DSM-IV in detail are as follows:
A. the person has been exposed to a harmful event where there have been any two following condition:
1. The person experienced an event or has seen events associated with a real danger or threat of death or serious injury, or is considered as a threat to the physical integrity of self or others.
2. The response of a person was accompanied with an intense fear, helplessness or horror. B. Harmful event experience is consistently
experienced again as one (or more) of the following ways again:
1. Frequent reminders and uncomfortable event including images, thoughts or perceptions.
2. Provoking discomfort and repetitive dreams about the incident.
3. Feeling and behaving as if the accident is being repeated (the occurrence of this incident, illusions, dissociative flashback episodes are the courses that occur in the waking state, respectively.
4. Strong psychological worries in the face of signs of internal or external association or similar harmful aspect of the event.
C. Continuous avoidance of stimuli associated with the trauma and reduce overall accountability which has never been before the accident, so that three or more of the following items can be determined
1. Trying to avoid remembering activities, places or people
2. Trying to avoid thoughts, feelings and conversations about the trauma.
3. Inability to recall an important aspect of the impact.
4. A significant decrease in interest or participation in important activities.
5. Feeling separated and strangeness in relationship with others.
6. Limitation of emotional range (not feeling romance)
7. Feel shorter future, for example, lack of expected future career, marriage, children or a normal life.
D. Symptoms of high continuous stimulation than usual (which previously did not exist) and with two or more of the following issues.
1. Difficulty in falling asleep or maintaining sleep.
2. Irritability or anger attacks 3. Difficulty in concentrating 4. Being alert
5. The increase in the reaction of a month. E. The length of the disorder symptoms of D,B
and C is longer than a month
1. Acute: if duration of symptoms is less than 3 months
2. Chronic: if duration of symptoms is 3 months or more
3. With late onset: if onset of symptoms is at least 6 months after the event (7).
Epidemiological studies show that most people will experience a traumatic event and will be faced with stressors, but only 10% will growth and continue their PTSD symptoms. The risk of disorder growth depends on the nature of the trauma.
A person with PTSD can create horror and the violence at home. PTSD patients are in positions where eventually recall the painful events, get angry and starts to panic or when they sleep and dream, remember scenes of war and wake up shouting. They drastically cause fear and confusion in their wife and other family members. If a soldier's wife wakes up in the moment, she reacts with panic intensity.These attacks can lead to sleep disturbances.The concept of secondary PTSD that has been raised in recent years, in general, refers to people wholive or work with people with PTSD. So this term includes the spouse, children, caregivers, family and therapists that are associated with the patient. Denying the problems, numbness and anesthesia have profound effect on the members of the family. Practice patterns and hiding the secrets in this family include pipe down, distrust, do not think, feel and act (8).
AzamPourafsharet al (9) have mentioned the following regarding the reactions ofthe family members of a patient with PTSD:
1. Compassion: one of the first reactions that occur for many families where one of the members is suffering from PTSD is compassion and caring. However, the compassion of a family member can have negative effects.
2. Depression: traumatic accident can be in itself one of the causes of depression in family members. Depression is very common among family members of these persons.
3. Fear: the fear of family members nay have multiple reasons. When a person with PTSD
often feels insecure and warns their family members about the possible danger, it could convey their feelings to them. On the other hand family members are constantly exposed to aggression and irritability fighter and this alert will startle them. Financial concerns and economic concerns about the involvement of members with PTSD in the outdoors with others add to the worries. 4. Avoidance: As a person with PTSD often to
bring up what had happened to them, family members also avoid to ask him anything about the incident. They may have to avoid the things he avoids because they want to stop her suffering.
5. Feelings shame and guilt: Family members may feel shame and guilt because of trauma and its consequences,. Each of them may remember blame themselves for what has happened.
6. Anger: members of the family may be very angry about the incident and the consequences affecting their lives. They are angry towards anyone who may consider it responsible for the accident and even the person with PTSD.On the other hand, their anger can be caused by aggression and anger caused by person with PTSD.
7. Negative emotions: family members sometimes have had a lot of negative emotions toward the affected member.They may think that he will never again have the same good-natured and kind.As a result, they show negative reactions to his behavior and may even hate him.
8. Alcohol and drug abuse: alcohol and drugs abuse can appear as a problem for the children of these families. Family members may be using drugs and alcohol to try to get rid of that bad feeling. On the other hand their wives may be affected due to companionship with their husbands who may turn to take drug to solve the problem and so the wives also use drug.
frequently or is experiencing nightmares. It's very difficult for family members to sleep easily, because he "has a feeling of depression or constantly worries.
10. Physical health problems: family members of the damaged person may for some reason be physically challenged. Permanent stress as a result of problems related to the impact on them can lead to many diseases such as digestive problems, stomach ulcers, headaches and muscle spasms (10).
Studies suggest that families of people with post-traumatic stress disorder, particularly their spouses, suffer from numerous psychological problems. Calhoun et al (11), in their study found that the severity of symptoms in patients with PTSD and interpersonal violence is associated with increased caregiver stress. So far no reliable study has been done on the topic of the present study. However, several studies have been conducted on the effectiveness of mindfulness training. For example, researchers trained 145 improved patients with depression with the techniques of mindfulness training and after 60 weeks of follow-up, results showed that the possibility of further depression in patients who had a high risk of recurrence (for example, three or more people who had experienced depression) is 40 percent, while this amountwas 66% among the depressed patients that had not received this training (12).
The study of Carlson et al (13) also showed a positive effect of mindfulness techniques on quality of life. They conducted a research on mindfulness-based stress reduction program concerning the effect on the quality of life of people with breast and prostatecancer. The results showed that after eight sessions of training, quality of life has increased.
Research of Walker et al (14) also showed that mindfulness-based training was effective to reduce stress, chronic pain, anxiety, prevention of recurrence of depression, generalized anxiety disorder, post-traumatic stress disorder and other similar disorders.
Sherman (15), in his study on the patients with PTSD and depression patients, using the techniques of mindfulness, showed a significant
decrease in the story, for more extended memory of the people reflecting the pattern of maladaptive cognitive processing and non-functional in them (16). Study of Dabagh et al (17) showed that mindfulness-based practices create a positive effect on states of mind and reduce anxiety and stress.
The results showed that the average quality of life of non-PTSD veterans in all of the quality of life was significantly more that wives with PTSD husbands. In other words spouses of veterans with PTSD and had lower quality of life than non-PTSD veterans' spouses.
Results of Parandeh et al (18) showed that quality of life is low and educational intervention and treatment of PTSD, can increase quality of life those with PTSD husbands.
Fenal(19), in a study showed that mindfulness techniques improved depression in patients with depression and in addition improving depression by the training leads to increased confidence in them.
Teasdale et al (20) in a study regarding the effectiveness of group mindfulness based relapse prevention depressed patients showed a return of depression in 77% of subjects with a history of three flares or more receiving corresponding training have declined significantly but it did not reduce the risk of recurrence and return in people with a history of recurrent depression twice or less.
In Iran, the study of Kaviani et al (21), to investigate the effects of mindfulness-based cognitive therapy on depression and anxiety followed for 60 days showed that depression and anxiety scores in the experimental group that received the relevant trainingwas significantly reduced compared to the control group that did not receive training.
Research Hypotheses
The main hypothesis of this study is as follows: Mindfulness training group influence the quality of life of patients with PTSD.
Secondary hypotheses of the study are as follows:
1. Mindfulness training group influence the general health of the spouses of patients with war PTSD
2. Mindfulness training group influence the social function of the spouses of patients with war PTSD
3. Mindfulness training group influence the mental health of the spouses of patients with war PTSD
4. Mindfulness training group influence the vitality and freshness of the spouses of patients with war PTSD
5. Mindfulness training group influence reducing the physical pain of the spouses of patients with war PTSD
6. Mindfulness training group influence reducing the low function of the spouses of patients with war PTSD
7. Mindfulness training group influence the emotional aspects of the spouses of patients with war PTSD
8. Mindfulness training group influence the physical function of the spouses of patients with war PTSD
METHODOLOGY
The study has a quasi-experimental design. In this study, the pretest and posttest with control group design was used. The population in this study included the wives of the patients with war PTSD in the East Azerbaijan Province who referred for the treatment of psychiatric and psychological clinics services. From among them, thirty of the patients were selected using simple random sampling method for study and were randomly assigned to two experimental and control groups (15 groups) and trained with group mindfulness techniques.In this study, quality of life questionnaire was used to collect the required data. The questionnaire was developed by the World Health Organization to examine quality of life and contains 36 main questions in the realm of physical and
psychological violence in the eight indicators related to health, physical functioning, bodily pain, low performance, general health, vitality, social functioning, emotional role and mental health and emotional).Mac Horn et al (2014) in their study reported the validity of the above mentioned questionnaire as seventy percent. The reliability and validity of the questionnaire for the first time by Montazeri et al (2005) was evaluated 4163. The reliability coefficient in 8 dimensions was 77% to 95% respectively. As well the covariance method was used in this study to analyze the data.
Procedure
Seventh and eighth sessions of mindfulness training purposes includes thoughts, paying attention to the positive and negative training the mind and thoughts and annoying and inconvenient, learning how to control entry and exit of positive and negative thoughts and behavioral effects of these thoughts and ultimately providing homework and the conclusion and implementation of the post-test training sessions.In general, the purpose of mindfulness in this study is to provide a method (cognitive - behavioral – biological method)
which gives new information about the psychological organization at the disposal of the person so the ability of individuals to control anxiety and emotional responses against multiple positions will be increased.
Findings
The data from this study can be seen in statistical tables. In the analysis the impact of control variable is taken in pre-test and post-test scores and then the two groups were compared with respect to the remaining scores.
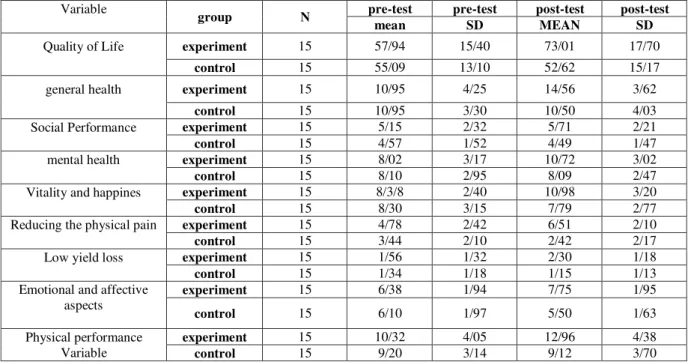
Table 1: the mean and standard deviation scores of experiment and control group at pre-test and post-test
Variable
group
N pre-test pre-test post-test post-test
mean
SD MEAN SD
Quality of Life experiment 15 57/94 15/40 73/01 17/70
control
15 55/09 13/10 52/62 15/17
general health experiment 15 10/95 4/25 14/56 3/62
control
15 10/95 3/30 10/50 4/03
Social Performance experiment 15 5/15 2/32 5/71 2/21
control
15 4/57 1/52 4/49 1/47
mental health experiment 15 8/02 3/17 10/72 3/02
control
15 8/10 2/95 8/09 2/47
Vitality and happines experiment 15 8/3/8 2/40 10/98 3/20
control
15 8/30 3/15 7/79 2/77
Reducing the physical pain experiment 15 4/78 2/42 6/51 2/10
control
15 3/44 2/10 2/42 2/17
Low yield loss experiment 15 1/56 1/32 2/30 1/18
control
15 1/34 1/18 1/15 1/13
Emotional and affective aspects
experiment
15 6/38 1/94 7/75 1/95
control
15 6/10 1/97 5/50 1/63
Physical performance Variable
experiment
15 10/32 4/05 12/96 4/38
control
15 9/20 3/14 9/12 3/70
Table 2: Summary results of covariance evaluated based on the group after controlling the variable of pre-test in post-test
Variable df F Sig. F
Quality of Life 1 10/25 0/001 0/86
general health 1 7/79 0/004 0/80
Social Performance 1 2/01 0/21 0/25
mental health 1 6/72 0/014 0/71
Vitality and happiness 1 8/89 0/004 0/80
Reduce physical pain. 1 5/87 0/020 0/63
Low yield loss 1 6/91 0/014 0/72
Emotional aspects of emotional 1 10/90 0/001 0/87
Physical performance 1 6/02 0/015 0/61
As Table 1 showed there was significant difference between the average scale of quality of life after controlling for pre-test variables in both experimental and control groups.Also according to Table (2) the results of analysis of covariance showed that based on the calculated coefficient F, the was a significant difference between the average estimated quality of life scores in experimental group and control there
functioning, bodily pain, low performance, general health, vitality, emotional role and mental health and emotionalexcept social functioning.
According to the results of covariance analysis (Table 2) since the obtained F value in the subscale variablesof quality of life including general health, vitality variable, the variable aspects of emotional excitement was significant at p< 0.01 level, this means with 99% confidence that hypotheses first, fourth and seventh are approved. So, it can be stated that the group mindfulness training enhances the quality of life in the domains relevant.
The obtained F value under the subscalesof reduces physical pain, low yield loss, mental health and physical function is significant at the level of p> 0.05.That is with 95% confidence level the third; fifth, sixth and eighth hypothesesare confirmed .So it can be said that the group mindfulness training also has an impact on these variables. However, considering the F value in social function with p>0.05, it can be concluded that the second hypothesis is rejected and the group mindfulness training had no impact on social functioning of life quality.
DISCUSSION
The results for the main hypothesis of the present study showed that mindfulness training increased the quality of life in the experimental group compared to the control group in the post-test. This finding is consistent with research results of Carmoudy et al (22), Teasdale (20), Bauer (23), Flip (24), Post and Wade (25) and is well consistent with the results of Nejati et al (26), Kazemi et al (27), Marzabadi et al (28). So, the spouses of people with untreated anxiety, stress and ignoring the mental and social needs and failure to improve quality of life cause reduction in energy sources and the creation of a variety of physical and mental problems and pressure would disable the multiple roles of the wife. Therefore, the use of group mindfulness practices is an effective way to balance up the quality of life of patients with warPTSD.
The results of the third, fourth, fifth, sixth, seventh, eighth hypotheses of the present study indicated that mindfulness training also improve
the quality of life of patients with war PTSD problems improved the subscales of the quality of life (general health, mental health, vitality, reduced physical pain, low yield loss, emotional aspects - emotional and physical function) separately. The results are in line with the studies of Carlson et al (13), Teasdaleet al (20), Golden et al (29), Sadat Kazemi (30), and Narimaniet al (31).
According to the surveys carried out by appropriate methods of training especially mindfulness-based approaches to couples, the possibility for solving and handling conflict in constructive manner is provided and so take realistic action due to actively dealing with problems. As a result, with increasing confidence, control thoughts, creating an intimate relationship, the abilities of the couples to solve problems of compatibility with the relevant conditions resulting in improved performance and increased quality of life is emphasized in all aspects of general family. However, the results of the second hypothesis indicated that that group mindfulness training techniques increased the quality of life in all its dimensions except social function for spouses of people with war PTSD and no reliable study has been found in this regard.
REFERENCE
1. Baer, R. A. (2003). Mindfulness training as a clinical intervention: A conceptual and empirical review. Clinical psychology: Science and practice. 10, 125-143.
2. Calhoun PS, Beckham JC, Bosworth HB. Caregiver burden and psychological distress in partnersof veterans with chronic posttraumatic stress disorder. J Trauma Stress 2002 15(3):205-212.
3. Carlson, L. E., Speca, M., Patel, K, D., g Goodey, E. (2003). Mindfulnrss-based stress reduction in relation to quality of life, mood, symptoms of stress and immune parameters in breast g prostat cancer outpatients psychosomatic Medicine, 65(4),571-581. 4. Carmodyjames, reed G, Kristeller Jean,
5. Carroll, E. M.(2002). Vietnam Combat veterans with posttraumatic stress disorder Analysis of marital and cohabitating adjustment. Journal of Abnormal psychology, 94, 329-337.
6. Dabaghi, P., Boulhari, J. (2009). The effect of war-related post-traumatic stress disorder, mental health, life satisfaction, marital and behavioral problems in children, Research and Science Journal seventh edition, University of Medical Sciences. 5, pp. 1-3. 7. Dezhkam, M., Aminoroaya A., comparing
the mental health of veterans Tehran psychiatric hospital wives topped with mental illness admitted to hospital Tehran Imam Hussein (AS). Tehran: Proceedings of the First Scientific Conference of the Veterans and Family, 2003.
8. Fenal, M.(2004). Cognitive-behavior therapy vs exposure therapy in the treatment of PTSD in refugees. BehavresTher, 39,83-97.
9. Flannery RB. Post traumatic stress disorder the victims guide to healing and recovery. New York: Crossroad Publishing Company; 1995.
10. Goldin PR, Gross JJ. Effects of mindfulnessbased stress reduction (MBSR) on emotion regulation in social anxiety disorder. Emotion.2010; (10): 83-91.
11. HashemZadeh, F. Fouladi, A, (2014). The effectiveness of coping with stress on marital satisfaction of spouses of people with PTSD caused by war. Journal of Research and Science, 6 (2), pp. 28-31 12. Hashemi, M. (2007). The effect of education
on marital satisfaction of spouses with Adler's approach. Master's thesis, University of Allameh, Journal of Research and Science
13. Kaviani, H.,.Alagheband, J., The effect of mindfulness-based cognitive therapy on depression and anxiety. Journal of Clinical Psychology (2011), third number, first year, pp. 37-34.
14. Kazemi, A. (2012). The effectiveness of training mindfulness-based cognitive strategies in the secondary traumatic stress disorder and psychological problems of
spouses of patients with post-traumatic stress disorder, Journal - management thought and behavior. Volume VI, Issue 23, pp. 42-31
15. Kazemi, A. Sadat. BaniJamali, S., Ahadi, H., Farokhi, N., (2012). Efficacy of cognitive strategies - behavioral secondary traumatic stress disorder (STSD) and psychological problems of spouses of veterans with chronic PTSD due to war. Journal of Medical Sciences, Islamic Azad University, Volume 22, Issue 2, pp 122-129 16. Marzabadi, E., Moghtadaee, K., Ariapour, S.,. (2013). the effectiveness of mindfulness training on psychological symptoms in veterans with post-traumatic stress disorder, Journal of Behavioral Sciences, Volume 7, Issue 1, pp. 74-67
17. Mirzaee J. Karami, G. (2007). Comprehensive guide theoretical and practical Traumatic Stress Disorder. Publishing Foundation. First Edition.
18. Najati, V., Amini, R., Zabihzadeh, A., Masoumi., M., Maleki,G., Shoaiee, F. (2011). Mindfulness as effective quality in blind veterans. Journal - Veteran Medical of Issue 11, pp. 7-1.
19. Narimani, M., Ariapour, S., Abolqasemi, A., Ahadi, B.. (2012). Effectiveness of training mindfulness and emotion regulation of emotion and creating spouses of chemical devotees, Journal of Medical Sciences, Year 15, No. 2, pp. 118-107.
20. Parandeh A., Haji Amini, Z., Maliki, A., the effect of muscle relaxation training on the quality of life of people with PTSD. Journal of Behavioral Sciences. (2009), 3(4), pp 312-314
21. Philippot, p. (2004). Aqualitative study of mindfulness based cognitive therapy for depression. Clinical psychojogy, Science and practice, 15,201-221.
22. Post Brian C, Wade Nathaniel G. Religion and Spirituality in Psychotherapy: A practice-Friendly Review of Research. Journal of Clinical Psychology: in Session. 2009; 65: 131-146
marital satisfaction among wives of veterans with PTSD. Journal of Psychology, 1st edition
24. Rezai, M., Younesi., J. (2010) impact of Emotionally Focused Couple Therapy on improving communication patterns with ptsd of war veterans and family Hmsranshan.fslnamh sixth Pzhvhy.sal 21.s Number Page 46-44.
25. Roth, B., & Robbins, D. (2004). Mindfulness-based stress reduction and health related quality of life. Psychosomatic medicine, 66 (1), 113-123.
26. Sadock B, Sadock V, Synopsis of Psychiatry: Behavioral science/clinical psychiatry, Shahreab-Ayandesazan publication, Tehran 2007
27. Sherman, M., Zanoti, D., &Jons, D. E. (2005). Key elements in couple therapy with veterans with combat post-traumatic stress disorder. Professional Psychology: Research & Practice, 36(6),479-490.
28. Sinha,P:&Mukerjec,N.(1990).Marital adjustment and space orientation ,Journal of Social Psychology,130(5)-633-639.
29. Taylor LC, Lemon P. Fundamental and nursing: The Art and science of nursing care. Philadelphia: Lippincott; 2011.
30. Teasdale, j.d., segal, z.v., Williams, j. M.G., rideway, v . A., g Soulsby, j. M. (2000) prevention of relapse recurrence in major depression mindfulness-based cognitive therapy. journal of consulting and clinical psychology,68,615-623.
31. Witkiewitz, K., Marlatt, A., g Walker, D. (2005). Mindfullness-based relapse prevention for alcohol and substance use disorder: The meditation tortoise wins the race. Journal of cognitive psychotherapy, 19, 221-229.