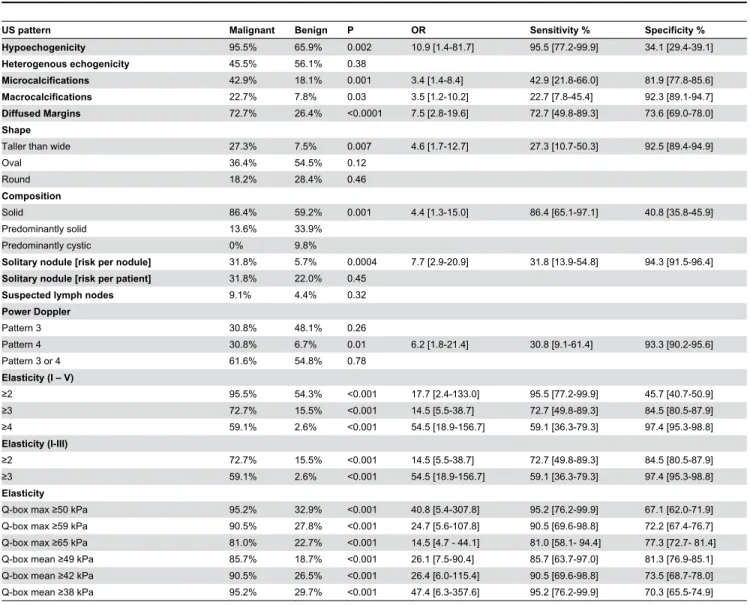
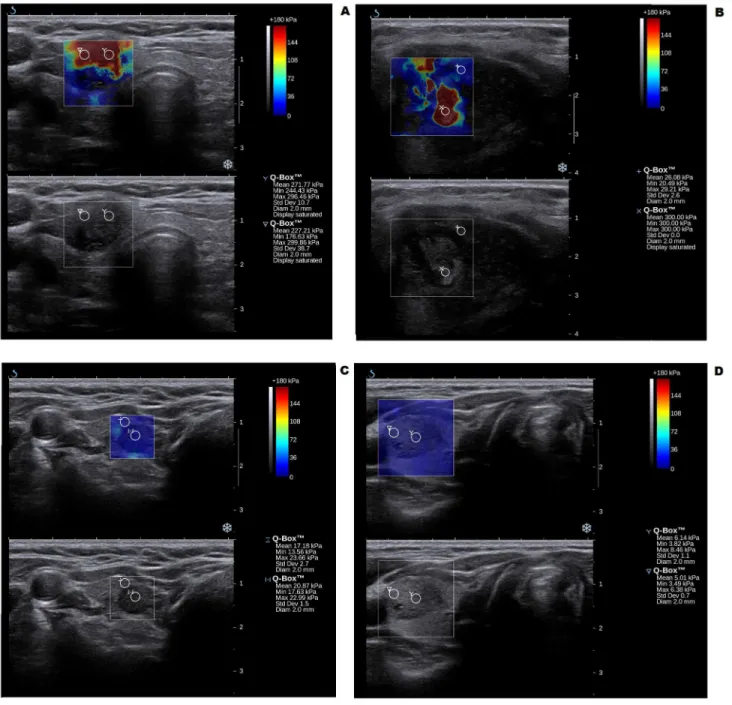
Comparison of diagnostic value of conventional ultrasonography and shear wave elastography in the prediction of thyroid lesions malignancy.
Texto
Imagem
Documentos relacionados
financeiras, como ainda por se não ter chegado a concluo entendimento quanto à demolição a Igreja de S. Bento da Ave-Maria, os trabalhos haviam entrado numa fase
Este artigo discute o filme Voar é com os pássaros (1971) do diretor norte-americano Robert Altman fazendo uma reflexão sobre as confluências entre as inovações da geração de
The probability of attending school four our group of interest in this region increased by 6.5 percentage points after the expansion of the Bolsa Família program in 2007 and
We also determined the critical strain rate (CSR), understood as the tangent of the inclination angle between the tangent to the crack development curve and the crack development
The iterative methods: Jacobi, Gauss-Seidel and SOR methods were incorporated into the acceleration scheme (Chebyshev extrapolation, Residual smoothing, Accelerated
Neste trabalho o objetivo central foi a ampliação e adequação do procedimento e programa computacional baseado no programa comercial MSC.PATRAN, para a geração automática de modelos
Ousasse apontar algumas hipóteses para a solução desse problema público a partir do exposto dos autores usados como base para fundamentação teórica, da análise dos dados
Pois quem não pode aceitar sua finitude ou se sente frustrado com o curso que sua vida tomou ou será invadido pelo desespero que o tempo é muito breve para recomeçar uma
