Dexmedetomidine decreases the in
fl
ammatory
response to myocardial surgery under
mini-cardiopulmonary bypass
N.M.H. Bulow
1,2, E. Colpo
2,4, R.P. Pereira
3, E.F.M. Correa
1,2, E.P. Waczuk
1, M.F. Duarte
1and
J.B.T. Rocha
11
Departamento de Bioquímica e Biologia Molecular, Programa de Pós-graduac¸ão em Ciências Biológicas
-Bioquímica Toxicológica, Centro de Ciências Naturais e Exatas, Universidade Federal de Santa Maria, Santa Maria, RS, Brasil
2Departamento de Cirurgia, Centro de Ciências da Saúde, Universidade Federal de Santa Maria, Santa Maria, RS, Brasil 3Departamento de Química, Programa de Pós-graduac
¸ão em Química Aplicada, Universidade Estadual de Ponta Grossa,
Ponta Grossa, PR, Brasil
4Departamento de Nutrição, Centro Universitário Franciscano, Santa Maria, RS, Brasil
Abstract
Cardiopulmonary bypass (CPB) with extracorporeal circulation produces changes in the immune system accompanied by an increase in proinflammatory cytokines and a decrease in anti-inflammatory cytokines. We hypothesize that dexmedetomidine (DEX) as an anesthetic adjuvant modulates the inflammatory response after coronary artery bypass graft surgery with mini-CPB. In a prospective, randomized, blind study, 12 patients (4 females and 8 males, age range 42–72) were assigned to DEX group and compared with a conventional total intravenous anesthesia (TIVA) group of 11 patients (4 females and 7 males). The endpoints used to assess inflammatory and biochemical responses to mini-CPB were plasma interleukin (IL)-1, IL-6, IL-10, interferon (INF)-g, tumor necrosis factor (TNF)-a, C-reactive protein, creatine phosphokinase, creatine phosphokinase-MB, cardiac troponin I, cortisol, and glucose levels. These variables were determined before anesthesia, 90 min after beginning CPB, 5 h after beginning CPB, and 24 h after the end of surgery. Endpoints of oxidative stress, including thiobarbituric acid reactive species and delta-aminolevulinate dehydratase activity in erythrocytes were also determined. DEX+TIVA use was associated with a significant reduction in IL-1, IL-6, TNF-a, and INF-g (Po0.0001) levels compared with TIVA (two-way ANOVA). In contrast, the surgery-induced increase in thiobarbituric acid reactive species was higher in the DEX+TIVA group than in the TIVA group (Po0.01; two-way ANOVA). Delta-aminolevulinate dehydratase activity was decreased after CPB (Po0.001), but there was no difference between the two groups. DEX as an adjuvant in anesthesia reduced circulating IL-1, IL-6, TNF-a, and INF-glevels after mini-CPB. Thesefindings indicate an interesting anti-inflammatory effect of DEX, which should be studied in different types of surgical interventions.
Key words: Cytokines; Systemic inflammatory response syndrome; Total intravenous anesthesia; Dexmedetomidine; Coronary artery bypass grafting surgery; Mini-cardiopulmonary bypass
Introduction
Exacerbated immunoinflammatory responses to cardio-pulmonary bypass (CPB) have been compared with systemic inflammatory response syndrome (SIRS) (1–3). Surgical
trauma, cardiac arrest, aortic cannulation, exposure of blood to nonphysiological surfaces of the cardiopulmonary bypass circuit, and ischemia/reperfusion injury trigger the excessive release of proinflammatory factors (cytokines, endothe-lins, platelet-activating factors, and endothelial and leuko-cyte adhesion molecules) (4–7). An atypical inflammatory
response observed in SIRS and after CPB has been reported to be associated with oxidative stress (4,8,9).
Anesthetic agents can exert clinical benefits during and after surgery (5,9–13). Optimistically, the ideal
anti-inflammatory anesthetic should reduce complications and mortality resulting from SIRS-like postoperative responses. Alpha 2-adrenergic receptor agonists have been used in anesthesia because of their sedative, analgesic, hemody-namic-stabilizing, and sympatholytic effects (9,14,15). In addition, the stress response to surgery can be modulated by postsynaptic centrala2-adrenergic receptor activation (16). However, only a few studies have investigated the anti-inflammatory properties of dexmedetomidine (DEX)
Correspondence: J.B.T. Rocha:<[email protected]>
after coronary artery bypass graft (CABG) surgery with mini-CPB (9,16–19).
Safe and effective agents with anti-inflammatory prop-erties to be used as anesthetics in major surgeries need to be identified (5,9). In this regard, DEX is considered as a promising candidate because a 2-adrenergic agonists have been reported to modulate inflammatory responses (13,16–19).
We hypothesize that DEX in association with a conventional total intravenous anesthesia (TIVA) (infusion of propofol and sufentanil) decreases the inflammatory response associated with CABG surgery. To test this hypothesis, we measured interleukin (IL)-1, IL-6, IL-10, tumor necrosis factor (TNF)-a, and interferon (IFN)-glevels as endpoints of inflammation in patients undergoing CABG surgery. Because the inflammatory response can trigger oxidative stress, two biochemical endpoints of oxidative stress, thiobarbituric acid reactive substances (TBARS) (20) and delta-aminolevulinate dehydratase (ALA-D) activ-ity (21), were also determined in erythrocytes.
Material and Methods
Institutional ethics review board approval (Protocol #23081.015056/2009-58, Approval #0271.0.243.000-9, Research Ethical Committee of UFSM in January 2010) and written informed consent from patients were obtained. A total of 30 clinical American Society of Anesthesiologists class II and III patients (42–72 years old) were included in
the study. They were scheduled for CABG surgery under mini-CPB and randomly assigned to the conventional TIVA (propofol/sufentanil) group (15 patients) or to the TIVA with DEX (propofol/sufentanil/DEX) (TIVA+DEX; 15 patients) group. The surgery team, surgeon, and perfusionist were the same for all of the patients. Patients were recruited during a period of 2 years during which data were collected.
Exclusion criteria included the following: severe ven-tricular dysfunction (left venven-tricular ejection fractiono40%),
reintervention surgery, requirement for blood products from the start of CPB, preoperative history of liver or kidney dysfunction, immunological disease, preoperative intake of corticosteroids or anti-inflammatory drugs (except for acetyl-salicylic acid), and a history of recent myocardial infarction (last 2 weeks).
Patients who were allocated to the TIVA group were anesthetized with TIVA in target-controlled infusion of propofol as a hypnotic (TCI infusion system, Diprifusors; AstraZeneca, Germany). Propofol was infused to an initial target blood concentration of 4mg/mL during the induction and maintenance of anesthesia. The target dose was based on bispectral (BIS) index monitoring (i.e., the dose was selected to have BIS values between 45 and 55). Sufentanil was infused at a dose of 0.5 to 1 mg/kg (induction) and maintained at 0.5 to 1mgkg-1h-1during surgery. Muscle relaxation for tracheal intubation was
obtained with 0.1 mg/kg pancuronium at induction and an additional one-third of this dose was provided if necessary. Patients who were allocated to the TIVA+DEX group were anesthetized with TIVA in target-controlled infusion of propofol as a hypnotic (TCI infusion system, Diprifusor). The initial target blood concentration of propofol was 4mg/mL for induction and maintenance of anesthesia. Sufentanil was administered at 0.5 to 1mg/kg during induction and at rates of 0.5 to 1mgkg-1h-1during the maintenance period. DEX was infused at 0.3 mgkg-1h-1during the entire surgery (induction and maintenance of anesthesia). The dose of DEX was lower than the average dose that is commonly used in surgeries to prevent bradycardia and because it was used together with sufentanil and propofol. Muscle relaxation for tracheal intubation was obtained with 0.1 mg/kg pancuronium at induction and an additional one-third of the dose was provided if necessary. Surgeons working in the operation room and the medical team in the intensive care unit (ICU) were blind to treatment protocols.
Systemic arterial blood pressure was measured via radial artery catheterization. A Swan-Ganz catheter (Edwards Lifesciences LLC, USA) was inserted for determining central venous pressure, pulmonary capillary pressure, and the cardiac index. Hemodynamic parameters were periodically monitored for a period of 24 h after surgery to detect and adjust arterial blood pressure and the cardiac index to be within 20% of that found at baseline (pre-operation level). Cardioscopy, pulse oximetry, expired CO2
levels, nasopharynx temperature, and the BIS index were monitored. The surgery was conducted under mini-CPB and mild hypothermia (34-35°C). Blood samples were collected to measure arterial gases, hemodilution, and electrolytes.
For determination of biochemical and inflammatory markers, arterial blood was sampled at radial catheteriza-tion before induccatheteriza-tion of anesthesia (baseline), 90 min after starting CPB (during surgery), 5 h after starting mini-CPB (within 2–3 h after the end of surgery), and 24 h after
the end of surgery.
Cytokines (IL-1, IL-6, IL-10, TNF-a, and INF-g) were measured by chemical analysis (commercial kits: eBio-sciences, USA). Plasma levels of C-reactive protein were
measured by immunoassay (Dimensions; Siemens,
Healthcare Diagnostics Inc., USA). We used a chemilumi-nescent method (Immulites; Siemens, Healthcare Diag-nostics Inc.) for determination of cardiac troponin I levels. Creatine phosphokinase (CPK) and CPK-MB levels were measured by enzymatic methods (Dimensions; Siemens, Healthcare Diagnostics Inc.), cortisol levels were deter-mined using a chemiluminescent enzyme immunoassay (Immulites; Siemens, Healthcare Diagnostics Inc.), and glucose levels were measured by a biochromatic method (Dimensions; Siemens, Healthcare Diagnostics Inc.).
TBARS (20) and ALA-D activity (21) in erythrocytes were determined as described previously.
hemodynamic data were collected by trained personnel who were not authors of this study and blind to the anesthetic regimen used. They also recorded the duration of the surgery, the duration of mini-CPB, time for extubation, time in the ICU, and time for in-hospital stay. Postoperative com-plications and necessity of inotropic support with dobuta-mine, dopadobuta-mine, and noradrenaline (i.e., the use of two or more of these inotropic drugs for hemodynamic stability) were recorded. However, their use was necessary only in three patients in the TIVA group and in two in the TIVA+DEX group.
All continuous data are reported as means±SD.
Statis-tical analysis was performed by two-way ANOVA (two anesthetic procedures four sampling times) with time and treatment as the two factors. Values were considered to be statistically significant when P waso0.05.
Results
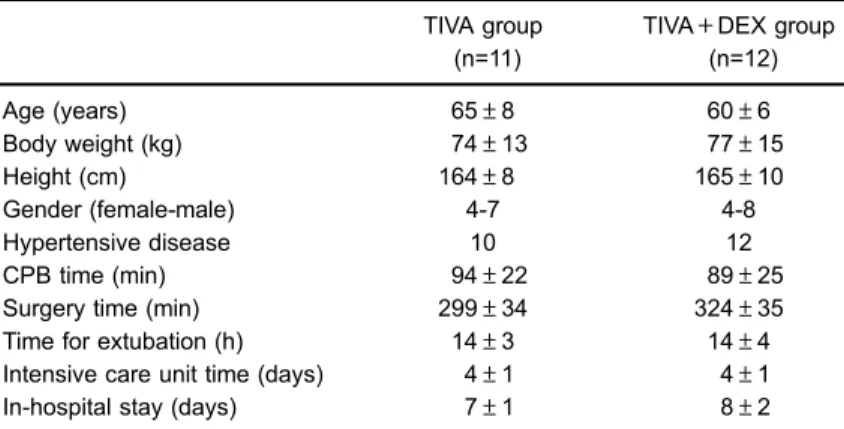
The characteristics of the two groups were similar regarding age, weight, height, comorbidities, mini-CPB time, total surgery time, time for extubation, time in the ICU, and in-hospital stay time (Table 1). Mean arterial pressure was decreased (Po0.01) and heart rate was increased (Po0.01)
in a similar manner in the two anesthetic groups after surgery compared with baseline (Supplementary Figure S1). Hemo-dilution was similar in both anesthetic groups. The hematocrit was significantly decreased after surgery and then increased in the 24-h recovery period after surgery (two-way ANOVA, Po0.0001; Supplementary Figure S1).
Plasma IL-1 (Figure 1A and B) and IL-6 (Figure 1C and D) levels were increased after surgery compared with baseline, but this increase was proportionally higher in the TIVA group
compared with the TIVA+DEX group (both Po0.0001).
Plasma IL-10 levels were decreased after CABG surgery compared with baseline (Po0.0001; Figure 1E and F).
Anesthesia with TIVA or TIVA+DEX did not modify the rate of decrease in IL-10 levels (Figure 1E and F).
Plasma INF-glevels (Figure 2A and B) and TNF-alevels (Figure 2C and D) were increased after surgery compared with baseline. However, the increase in INF-g and TNF-a
levels was proportionally higher in the TIVA group than in the TIVA+DEX group (Figure 2A–D; both Po0.0001).
Plasma C-reactive protein levels were significantly increased only after 24 h (Supplementary Figure S2; Po0.0001), CPK levels gradually increased after surgery
(Supplementary Figure S2C and D), and CPK-MB levels immediately increased after the end of surgery compared with baseline (Supplementary Figure S2E and F). How-ever, the changes in these markers were similar between the two anesthetic groups. Troponin, cortisol, and glucose levels were increased after surgery compared with base-line, but no differences were observed between the two anesthetic procedures (Supplementary Figure S3).
TBARS in erythrocytes were increased after surgery compared with baseline. This increase in TBARS was proportionally higher in the TIVA+DEX group than in the TIVA group (Figure 3A and B; Po0.01). ALA-D activity
was decreased after surgery compared with baseline, and this decrease was lowest 24 h after surgery in both experimental groups (Figure 3C and D; Po0.001).
Discussion
The mainfinding of the present study was that DEX (as a component of TIVA) modified the inflammatory response
Table 1.Anthropometric characteristics and surgery-related parameters of the two groups of patients.
TIVA group (n=11)
TIVA+DEX group (n=12)
Age (years) 65±8 60±6
Body weight (kg) 74±13 77±15
Height (cm) 164±8 165±10
Gender (female-male) 4-7 4-8
Hypertensive disease 10 12
CPB time (min) 94±22 89±25
Surgery time (min) 299±34 324±35 Time for extubation (h) 14±3 14±4
Intensive care unit time (days) 4±1 4±1 In-hospital stay (days) 7±1 8±2
in CABG surgery under mini-CPB. DEX use was asso-ciated with a reduced increase in plasma IL-1, IL-6, TNF-a, and INF-glevels compared with conventional TIVA. In both groups of patients, a similar postoperative decrease in IL-10 levels occurred. In contrast to our expectation, DEX use was associated with an increase in TBARS levels in erythrocytes after surgery compared with the TIVA group. The decrease in activity of ALA-D, which is considered as a putative marker of oxidative stress (21,22), was similar in both anesthetic groups. Taken together, these results indicated dissociation between changes in the levels of inflammatory markers and oxidative stress in erythrocytes of patients who were subjected to CABG surgery.
There are limited data on the effects of DEX and other
a-2 adrenergic receptor agonists on cytokines (13,23–30)
and TNF-aproduction by macrophages (27,28). Taniguchi et al. (25,26) demonstrated that DEX has inhibitory effects on cytokine release triggered by endotoxemia. Therefore, one of the mechanisms of anti-inflammatory effects of DEX may be via modulation of cytokine production by macrophages and monocytes. Similarly, Hofer et al. (29) showed that clonidine decreased proinflammatory cyto-kine production in experimental sepsis. They observed an
improvement in survival after induction of sepsis in mice by preventive administration of clonidine or DEX (29,30). In accordance with ourfindings, they reported a reduction in the plasma proinflammatory mediators IL-1b, IL-6, and TNF-a (29). They suggested the use of central-acting
a2-adrenergic receptor agonists as a preventive therapeutic option in major surgery. In the current study, patients did not have sepsis, but CABG surgery resulted in a high immunological stress response, which to some extent is similar to SIRS. Of particular therapeutic significance, DEX (TIVA+DEX) hampered the surgery-induced increase in IL-1, IL-6, INF-g, and TNF-alevels compared with conven-tional TIVA. Notably, one study showed that DEX decreased the inflammatory response in ICU patients with severe sepsis more than did propofol infusion (30), when TNF-a, IL-1, and IL-6 were used as endpoints of inflammation.
Recently, Peng et al. (31) demonstrated that DEX was a potent suppressor of lipopolysaccharide-induced infl amma-tion in activated microglia and may be a potential thera-peutic agent for the treatment of intensive care unit delirium. They investigated the effects of DEX on the production of proinflammatory mediators in lipopolysaccharide-stimulated microglia and found that DEX (10 and 100 ng/mL) inhibited Figure 1.Interleukin (IL)-1 (A,B), IL-6 (C,D), and IL-10 (E,F) levels were measured in patients who underwent coronary arterial bypass graft surgery under mini-cardiopulmonary bypass, using two dif-ferent types of anesthesia (conventional total intra-venous anesthesia [TIVA; n=11] and TIVA+DEX [n=12]). Two-way ANOVA showed a significant interaction between type of anesthesia and sam-pling time for IL-1 and IL-6 levels (Po0.0001). This finding indicated that the increase in IL-1 and IL-6 levels as a function of time after surgery was attenuated in patients who were anesthetized with TIVA+DEX compared with those who received only TIVA. Two-way ANOVA of IL-10 levels only showed a significant main effect of sampling time (Po0.0001) with a similar and progressive
the release of nitric oxide, prostaglandin E2, interleukin 1b, and TNF-a. The dosage that we used in the current study can be considered low to moderate. Nevertheless, this dose diminished the surgery-induced increase in plasma IL-1, IL-6, TNF-a, and INF-glevels.
DEX can inhibit cortisol synthesis, but this has not been reported in short-term use in humans (32–34). In fact,
Bekker et al. (35) hypothesized that intraoperative admin-istration of DEX reduces the stress response and improves the quality of recovery in patients undergoing major spinal
surgery by negatively modulating the increase in plasma cortisol levels observed after surgery (35). However, we did not observe any differences in increased levels of cortisol and glucose between the two anesthetic groups of patients (for details, see Supplementary material).
In this study, we demonstrated that DEX attenuated the increase in IL-1, IL-6, TNF-a, and INF-glevels in patients under CABG surgery with mini-CPB. One of the limitations of the present study was the small number of enrolled patients. However, the variability in inflammatory markers Figure 2.A, B,Plasmag-interferon (INF-g) and
C, D, tumor necrosis factor-a(TNF-a) levels in patients who underwent coronary arterial bypass graft surgery under mini-cardiopulmonary by-pass, using two different types of anesthesia (conventional total intravenous anesthesia [TIVA; n=11] and TIVA+DEX [n=12]). Two-way ANOVA showed a significant type of anesthesia versus sampling time interaction for INF-g and TNF-a
levels (Po0.0001). Thisfinding indicated that the
increase in INF-gand TNF-alevels after surgery was lower in patients who were anesthetized with TIVA+DEX than in patients who received only TIVA.
Figure 3. A, B, Thiobarbituric reactive sub-stances (TBARS) and C, D, d-aminolevulinate dehydratase (ALA-D) enzyme activity of erythro-cytes in patients who underwent coronary arterial bypass graft surgery under mini-cardiopulmonary bypass, using two different types of anesthesia (conventional total intravenous anesthesia [TIVA; n=11] and TIVA+DEX [n=12]). For TBARS, two-way ANOVA showed a significant sampling time versus type or anesthesia interaction (Po0.001).
was satisfactory. Furthermore, the dose of DEX used was low. Future studies on the anti-inflammatory effect of DEX at high doses need to be performed. Indeed, the safety and efficacy of high doses of DEX in patients undergoing major surgeries need to be determined to assess its appropriate-ness as an ideal anti-inflammatory anesthetic. In short, based on our results, we conclude that DEX is an important anesthetic adjuvant in cardiac surgery.
Supplementary Material
Click here to view [pdf].
Acknowledgments
This study was supported by Fundac¸ão de Amparo a
Pesquisa do Estado do Rio Grande do Sul (FAPERGS), Coordenac¸ão de Aperfeic¸oamento de Pessoal de Nível
Superior (CAPES), Conselho Nacional de Desenvolvi-mento Científico e Tecnológico (CNPq), Rede Instituto Brasileiro de Neurociência [(FINEP (IBN-Net) #01.06. 0842-00], FAPERGS-PRONEX-CNPQ, Instituto Nacional de Ciência e Tecnologia em Excitotoxicidade e
Neuropro-tec¸ão (INCT-EN), and
FAPERGS-PQ-GAUCHO-2014-2015 (2251/14-7).
References
1. Sander M, von Heymann C, von Dossow V, Spaethe C, Konertz WF, Jain U, et al. Increased interleukin-6 after cardiac surgery predicts infection.Anesth Analg2006; 102: 1623–1629, doi: 10.1213/01.ane.0000215998.21739.48.
2. Murkin JM. Panvascular inflammation and mechanisms of injury in perioperative CNS outcomes. Semin Cardiothorac Vasc
Anesth2010; 14: 190–195, doi: 10.1177/1089253210378177.
3. Wan S, LeClerc JL, Vincent JL. Inflammatory response to cardiopulmonary bypass: mechanisms involved and possi-ble therapeutic strategies.Chest1997; 112: 676–692, doi:
10.1378/chest.112.3.676.
4. Matata BM, Sosnowski AW, Galinanes M. Off-pump bypass graft operation significantly reduces oxidative stress and inflammation. Ann Thorac Surg 2000; 69: 785–791, doi:
10.1016/S0003-4975(99)01420-4.
5. Hall R. Identification of inflammatory mediators and their modulation by strategies for the management of the systemic inflammatory response during cardiac surgery.
J Cardiothorac Vasc Anesth 2015; 27: 983–1033, doi:
10.1053/j.jvca.2012.09.013.
6. Mathew JP, Parks R, Savino JS, Friedman AS, Koch C, Mangano DT, et al. Atrialfibrillation following coronary artery bypass graft surgery: predictors, outcomes, and resource utilization. MultiCenter Study of Perioperative Ischemia Research Group.JAMA1996; 276: 300–306, doi: 10.1001/
jama.1996.03540040044031.
7. Rose EA. Off-pump coronary-artery bypass surgery.N Engl
J Med2003; 348: 379–380.
8. Rodemeister S, Duquesne M, Adolph M, Nohr D, Biesalski HK, Unertl K. Massive and long-lasting decrease in vitamin C plasma levels as a consequence of extracorporeal circula-tion.Nutrition 2014; 30: 673–678, doi: 10.1016/j.nut.2013.
10.026.
9. Bulow NMH, Colpo E, Duarte MF, Correa EFM, Schlosser RS, Lauda A, et al. Inflammatory response in patients under coronary artery bypass grafting surgery and clinical implica-tions: a review of the relevance of dexmedetomidine use.
ISRN Anesthesiology2014, doi: 10.1155/2014/905238.
10. Aantaa R, Jalonen J. Perioperative use of alpha2-adreno-ceptor agonists and the cardiac patient.Eur J Anaesthesiol
2006; 23: 361–372, doi: 10.1017/S0265021506000378.
11. Corcoran TB, Engel A, Sakamoto H, O’Shea A, O’ Callaghan-Enright S, Shorten GD. The effects of propofol on neutrophil function, lipid peroxidation and inflammatory response during
elective coronary artery bypass grafting in patients with impaired ventricular function.Br J Anaesth2006; 97: 825–831, doi: 10.1093/bja/ael270.
12. Memis D, Hekimoglu S, Vatan I, Yandim T, Yuksel M, Sut N. Effects of midazolam and dexmedetomidine on infl amma-tory responses and gastric intramucosal pH to sepsis, in critically ill patients.Br J Anaesth2007; 98: 550–552, doi:
10.1093/bja/aem017.
13. Nader ND, Ignatowski TA, Kurek CJ, Knight PR, Spengler RN. Clonidine suppresses plasma and cerebrospinalfluid con-centrations of TNF-alpha during the perioperative period.
Anesth Analg2001; 93: 363–369, doi:
10.1213/00000539-200108000-00026.
14. Adams R, Brown GT, Davidson M, Fisher E, Mathisen J, Thomson G, et al. Efficacy of dexmedetomidine compared with midazolam for sedation in adult intensive care patients: a systematic review.Br J Anaesth2013; 111: 703–710, doi:
10.1093/bja/aet194.
15. Abdallah FW, Brull R. Facilitatory effects of perineural dexmedetomidine on neuraxial and peripheral nerve block: a systematic review and meta-analysis.Br J Anaesth2013; 110: 915–925, doi: 10.1093/bja/aet066.
16. Candiotti KA, Bergese SD, Bokesch PM, Feldman MA, Wisemandle W, Bekker AY. Monitored anesthesia care with dexmedetomidine: a prospective, randomized, double-blind, multicenter trial. Anesth Analg 2010; 110: 47–56, doi:
10.1213/ane.0b013e3181ae0856.
17. Can M, Gul S, Bektas S, Hanci V, Acikgoz S. Effects of dexmedetomidine or methylprednisolone on inflammatory responses in spinal cord injury. Acta Anaesthesiol Scand
2009; 53: 1068–1072, doi: 10.1111/j.1399-6576.2009.02019.x.
18. Gu J, Chen J, Xia P, Tao G, Zhao H, Ma D. Dexmedetomidine attenuates remote lung injury induced by renal ischemia-reperfusion in mice. Acta Anaesthesiol Scand 2011; 55: 1272–1278, doi: 10.1111/j.1399-6576.2011.02526.x.
19. Sleigh J. All hands on dex.Anaesthesia 2012; 67: 1193– 1197, doi: 10.1111/j.1365-2044.2012.07334.x.
20. Grotto D, Santa Maria L, Valentini J, Paniz C, Schmitt G, Garcia SC, et al. Importance of the lipid peroxidation biomarkers and methodological aspects for malondialde-hyde quantification.Quimica Nova2009; 32: 169–174, doi:
10.1590/S0100-40422009000100032.
of intoxication with metals and other pro-oxidant situations.
Toxicol Res2012; 1: 85–102, doi: 10.1039/C2TX20014G.
22. Rocha JBT, Bulow NMH, Correa EF, Scholze C, Nogueira CW, Barbosa NBV. Dexmedetomidine protects blood
d-minolevulinate dehydratase from inactivation caused by hyperoxygenation in total intravenous anesthesia.Hum Exp Tox2011; 30: 289–295, doi: 10.1177/0960327110372399.
23. Straub RH, Herrmann M, Berkmiller G, Frauenholz T, Lang B, Scholmerich J, et al. Neuronal regulation of interleukin 6 secretion in murine spleen: adrenergic and opioidergic control.J Neurochem1997; 68: 1633–1639, doi: 10.1046/
j.1471-4159.1997.68041633.x.
24. Wu X, Song X, Li N, Zhan L, Meng Q, Xia Z. Protective effects of dexmedetomidine on blunt chest trauma-induced pulmonary contusion in rats. J Trauma Acute Care Surg
2013; 74: 524–530, doi: 10.1097/TA.0b013e31827d5de3.
25. Taniguchi T, Kidani Y, Kanakura H, Takemoto Y, Yamamoto K. Effects of dexmedetomidine on mortality rate and inflammatory responses to endotoxin-induced shock in rats.
Crit Care Med2004; 32: 1322–1326, doi: 10.1097/01.CCM.
0000128579.84228.2A.
26. Taniguchi T, Kurita A, Kobayashi K, Yamamoto K, Inaba H. Dose- and time-related effects of dexmedetomidine on mortality and inflammatory responses to endotoxin-induced shock in rats.J Anesth2008; 22: 221–228, doi: 10.1007/ s00540-008-0611-9.
27. Lai YC, Tsai PS, Huang CJ. Effects of dexmedetomidine on regulating endotoxin-induced up-regulation of inflammatory molecules in murine macrophages.J Surg Res2009; 154: 212–219, doi: 10.1016/j.jss.2008.07.010.
28. Szelenyi J, Kiss JP, Vizi ES. Differential involvement of sympathetic nervous system and immune system in the modulation of TNF-alpha production by alpha2- and
beta-adrenoceptors in mice. J Neuroimmunol 2000; 103: 34–40, doi: 10.1016/S0165-5728(99)00234-9.
29. Hofer S, Steppan J, Wagner T, Funke B, Lichtenstern C, Martin E, et al. Central sympatholytics prolong survival in experi-mental sepsis.Crit Care2009; 13: R11, doi: 10.1186/cc7709. 30. Tasdogan M, Memis D, Sut N, Yuksel M. Results of a pilot study on the effects of propofol and dexmedetomidine on inflammatory responses and intraabdominal pressure in severe sepsis. J Clin Anesth 2009; 21: 394–400, doi: 10.1016/j.jclinane.2008.10.010.
31. Peng M, Wang YL, Wang CY, Chen C. Dexmedetomidine atten-uates lipopolysaccharide-induced proinflammatory response in primary microglia.J Surg Res2013; 179: e219–e225, doi:
10.1016/j.jss.2012.05.047.
32. Maze M, Virtanen R, Daunt D, Banks SJ, Stover EP, Feldman D. Effects of dexmedetomidine, a novel imidazole sedative-anesthetic agent, on adrenal steroidogenesis:in vivo
andin vitrostudies.Anesth Analg1991; 73: 204–208.
33. Venn RM, Bryant A, Hall GM, Grounds RM. Effects of dexmedetomidine on adrenocortical function, and the cardio-vascular, endocrine and inflammatory responses in post-operative patients needing sedation in the intensive care unit.
Br J Anaesth2001; 86: 650–656, doi: 10.1093/bja/86.5.650.
34. Bulow NM, Barbosa NV, Rocha JB. Opioid consumption in total intravenous anesthesia is reduced with dexmedetomi-dine: a comparative study with remifentanil in gynecologic videolaparoscopic surgery. J Clin Anesth 2007; 19: 280– 285, doi: 10.1016/j.jclinane.2007.01.004.
35. Bekker A, Haile M, Kline R, Didehvar S, Babu R, Martiniuk F, et al. The effect of intraoperative infusion of dexmedetomi-dine on the quality of recovery after major spinal surgery.
J Neurosurg Anesthesiol 2013; 25: 16–24, doi: 10.1097/