Clinical
Paper
Oral
Surgery
Comparative
efficacy
of
nimesulide
and
ketoprofen
on
inflammatory
events
in
third
molar
surgery:
a
split-mouth,
prospective,
randomized,
double-blind
study
E.C. Pouchain,F.W.G.Costa,T.P.Bezerra,E.C.S.Soares:Comparativeefficacy ofnimesulideandketoprofenoninflammatoryeventsinthirdmolarsurgery:a split-mouth,prospective,randomized,double-blindstudy. Int.J.OralMaxillofac.Surg. 2015;44:876–884. #2015InternationalAssociationofOralandMaxillofacial
Surgeons. PublishedbyElsevierLtd.Allrightsreserved.
E.C.Pouchaina,F.W.G.Costab, T.P.Bezerrab,E.C.S.Soaresb aPostgraduateResidencyPrograminOral andMaxillofacialSurgery,WalterCantı´dio UniversityHospital,Fortaleza,Ceara´,Brazil; bPostgraduatePrograminDentistry,Federal UniversityofCeara´,Fortaleza,Ceara´,Brazil
Abstract. Thisstudyaimedtocomparetheeffectofnimesulideandketoprofenon
inflammatoryparametersrelatedtothesurgicalremovalofthirdmolars.A
split-mouth,prospective,randomized,double-blindstudywasconductedinpatients
undergoingremovaloffourthirdmolars.Eighteeneligiblepatientswereallocated
tooneoftwogroupstoreceivetreatmenttwotimesadaywitheitherketoprofen
100mgornimesulide100mgforaperiodof3days.Therescuemedicationintake
(number)andpainintensitywereevaluatedat6,12,24,and48h,andat7days
postoperatively. Swellingandmaximummouthopeningwereevaluatedat24h,
72h,and7dayspostoperatively.Thepeakpainscoreoccurredat6haftersurgery
inthenimesulidegroupandat12hintheketoprofengroup.Therewasno
statisticallysignificantdifferencebetweenthegroups,althoughpainreliefwas
observedafter48hinthenimesulidegroupandafter7daysintheketoprofengroup.
Foreachgroup,therewasastaticallysignificantdifferenceinpainscoresamongthe
studiedperiods(P<0.0001).Noneofthe patientsrequiredrescuemedication.
Therewasastatisticallysignificantdifferenceinmaximummouthopeningbetween
the preoperativeandpostoperativeperiods(P<0.0001).Ketoprofenand
nimesulidewereeffectiveatcontrollingpain,swelling,andtrismusafterthe
surgicalremovalofthirdmolars.
Keywords: analgesia;thirdmolar;nimesulide; ketoprofen;split-mouth.
Acceptedforpublication22October2014 Availableonline3April2015
http://dx.doi.org/10.1016/j.ijom.2014.10.026,availableonlineathttp://www.sciencedirect.com
The surgical removal of impacted third molars is considered the most common outpatient procedure among oral surger-ies.1–3 Normally, an inflammatory reac-tion with pain, swelling, and trismus is observedasaresultofthisprocedure.1–3 Theremovalofthirdmolarsiscommonly associated with a significant change in qualityoflife,4particularlyduringthefirst threepostoperativedays.5Therefore,itis necessarytotakemeasurestocontrolthe postoperative inflammatoryevents. Such measures include cryotherapy,6 laser ap-plication,7andNSAIDs(non-steroidal an-ti-inflammatorydrugs).8,9
Nimesulide (4-nitro-2-phenoxy meth-ane sulfonanilide) belongs to the group of sulfanilamide derivatives, differing from otherNSAIDs bypresentinga sul-fonanilideradicalratherthanacarboxylic radical.9Thisdrugisapartiallyselective cyclooxygenase2enzyme(COX-2) inhib-itor,usedforthetreatmentofacutepain, suchasthatassociatedwithosteoarthritis. Itiscurrentlyacceptedforuseincountries ofdifferentregionsoftheworld,including Europe, LatinAmerica,andAsia. Nime-sulidehasshownefficacyinthetreatment of acute pain associated with different diseases, such as back pain, toothache, postoperative pain and inflammation, and headache and migraine.9–13 Its effi-ciency has been evaluated in more than 200clinicalstudies,whichhaveincluded morethan90,000patientswith inflamma-toryandacutelypainfulconditions.9The use of nimesulide in the symptomatic treatment of inflammatory pain is sup-portedbytherapidonsetoftheanalgesic drug effect, which becomes apparent at 15min after its administration. Thus, nimesulide is a valuable option when therapidreliefofpainisrequired.14,15
Ketoprofen is aneffective inhibitor of cyclooxygenaseandprostaglandin synthe-sis,16demonstratingantipyretic,analgesic, andanti-inflammatoryproperties.17,18This drug has been used in the treatment of musculoskeletal disorders, and evidence fromclinicalstudiessuggeststhat ketopro-fenisaseffectiveasother anti-inflamma-toriesinthereductionofpostoperativepain and discomfort.8 Following third molar removal, thisdrug relievespain approxi-mately25.5minafteritsadministration.19 Several clinical trials have been con-ductedtocomparetheactionsof acetami-nophen,1,19,20 ibuprofen,19 ketorolac,21 meloxicam,22 ketoprofen,8,20,23,24 and nimesulide22,24inthecontrolof inflamma-tory eventsafter third molarsurgery. To date, only onestudyhasbeenperformed tocomparetheeffectsofnimesulide and ketoprofenontheinflammationcausedby
thissurgicalprocedure,andthedrugswere administered rectally.25 Therefore, we present theresultsof a split-mouth, pro-spective, randomized, double-blind trial aimed at assessing and comparing the effects of orallyadministerednimesulide andketoprofenonpain,swelling,and tris-mus in patients undergoing the surgical removal offourthirdmolars under local anaesthesia.
Materialsandmethods
Studydesignandsample
The present prospective, single-centre, randomized, double-blind pilot study usingasplit-mouthdesignwasconducted onpatientsrecruitedfromthedivisionof oralandmaxillofacialsurgeryofthe uni-versityhospitalwhorequiredthirdmolar extraction.Thisstudywasapprovedbythe university hospital ethics committeeand was performed in accordance with the Declaration of Helsinki. Patient recruit-mentwasconductedbetweenApril2011 andJune2012andfollowedtheguidelines oftheCONSORTstatement.26
This study included healthy subjects (ASA classification I; American Society of Anesthesiologists) of both genders, aged 18–35years,withanindicationfor removaloftheirfourthirdmolarsandno periodontal disease. The subjects were able and willing to cooperate with the protocolandtosignanappropriatewritten informed consent form. Furthermore, to standardizethesample,eachpatienthadto have similar patterns of tooth and root formation,position,andimpactiondegree betweentheupperandlowerthirdmolars oftherightandleftsidesofthemouth.27 Patientswereexcludediftheyfulfilledat leastoneofthefollowingcriteria:smoker, pregnantorbreast-feeding,using medica-tionsthatinteractwiththedrugsused in thisstudy,haveorthodonticbandsonthe second molars, a known allergy to NSAIDs,asystemicchronicdisease,signs ofanypre-existingacuteinflammatoryor infectious condition, or a history of NSAID useinthepast 21days.Patients whodidnotfollowtheindicated recom-mendations or whose surgery exceeded 2hwereremovedfromthisstudy.Patients whodidnotreturnforreassessmentwere alsoremoved.
Patientdatawererecorded preoperative-lyandaccordingtoastandardizedclinical examination, and included gender, age, systemic conditions, periodontal status, haemogramparameters,plateletcount, in-ternationalnormalized ratio(INR)value, and blood glucose. Orthopantomograms
wererequiredto evaluatetoothvariables such asposition,Pelland Gregory28 and Winter29classifications,tooth/root forma-tion,anddegreeofimpaction.
Patientswerescheduled forsurgeryat twoseparateclinicalsessions(onesideat atime)atleast3weeksapart.Eachperson had both upper and lower third molars removedatthesametimeontheinvolved side.Subjectswereallocatedtooneoftwo groupsaccordingtoacomputer-generated randomization code to receive treatment two times a day with either ketoprofen 100mgornimesulide100mg(onetablet every 12h for3 days). Thestudy drugs were dispensed asidentical tablets bya blindedcollaborator.Priortothesurgical procedure,themethodofallocation con-cealmentoftherightandleftsidesofthe mouth was followed, as described by Bezerra et al.27 Antibiotic prophylaxis wasnotadoptedforthesurgicalprocedure.
Surgicaloverview
Allpatientsweresubmittedtoa standard-ized surgical technique performed inan outpatientsettingunderlocalanaesthesia, followed bystrictbiosafetycontrol.One surgeon with 5 years of experience in dentoalveolar surgery performed all of thesurgicalprocedures.Thesamesurgical procedure was adoptedfor bothsidesof the mouth,aimingtoreducethe bias re-lated tothe intraoperativetrauma. Local anaesthesiawith2%mepivacaine associ-ated with 1:200,000 epinephrine (three cartridges)wasadministered.A mucoper-iosteal flapwasraisedandboneremoval and/or tooth sectioning was performed. The surgical wound was closed using a 4–0silksuture.
After surgery, 750mg of acetamino-phen was allowed as rescue medication for7daysifnecessary.Thepostoperative recommendationswerecarefullyreadand explainedtothepatient,inparticular the need for aliquid and colddietfor 24h, rigorousoralhygiene,andtoavoid mouth-wash. Patients were informed that they should contactthe surgeonby telephone in thecaseofpersistentbleeding orany other complicationssuchasfever.
Outcomemeasures
or discomfort). Before starting the treat-ment,eachpatientreceivedanexplanation abouthowtomeasurepainintensityonthis scale. Study participants were asked to record the pain intensity score at 6, 12, 24, 48, and 72h, and 7 days following surgery. Additionalanalyses includedthe evaluationoftimetore-medication,which was defined byOnget al.30as‘the time fromtheendofsurgeryuntiltheintakeof rescue medication became necessary for thepatient’.Thenumberofpatients requir-ingacetaminophenafterthesurgical pro-cedure and the number of analgesics consumed during the study period were recorded.
Thesecondaryoutcomewasthe occur-rence of postoperative inflammatory events.Thefollowingmeasurementswere performed to evaluate postoperative swellingonthefacialside receiving sur-gery(Fig.1):tragustothesoftpogonion (Tr–Pog’),tragustotheexternalcornerof theeye(Tr–Exo),tragustothenasal bor-der(Tr–Al),tragustothelabial commis-sure (Tr–Che), angle ofthemandible to theexternalcorneroftheeye(Go–Exo), angleofthemandibletothenasalborder (Go–Al),angleofthemandibletothesoft pogonion (Go–Pog’), and angle of the mandible tothelabial commissure(Go– Che).Thedifferencesbetweenthe preop-erative values (baseline)and those mea-sured at 24h, 72h, and 7 days after surgery werecompared.
To estimate trismus,maximum mouth openingwasmeasuredinmillimetres be-tweentheupperandlowercentralincisors usinga calibratedslidingcaliper (Thera-Bite Range-of-Motion Scales), preopera-tively(baseline)andat24h,72h, and7 daysaftersurgery.
Statisticalanalysis
Standard statistical evaluation included the Kolmogorov–Smirnov testto evalu-ate the normality of the distributions. Pain scores andfacial distancesdid not followtheGaussianpatternofnormality, differingfrommaximummouthopening, which did.TheMann–Whitneytestwas usedforcomparisonsofpainscoresand facial distances between the ketoprofen and nimesulide groups. The Friedman test (Dunn post hoc test) was used to assessthesamevariables(painscoreand facialdistances)amongeachofthefixed postoperative time intervals. One-way analysis of variance (ANOVA; Tukey post hoc tests)and the t-test were used toassess themeansofmaximum mouth opening. All data were expressed as the meanstandard deviation (SD).
Statistical significance was set at P<0.05.
Results
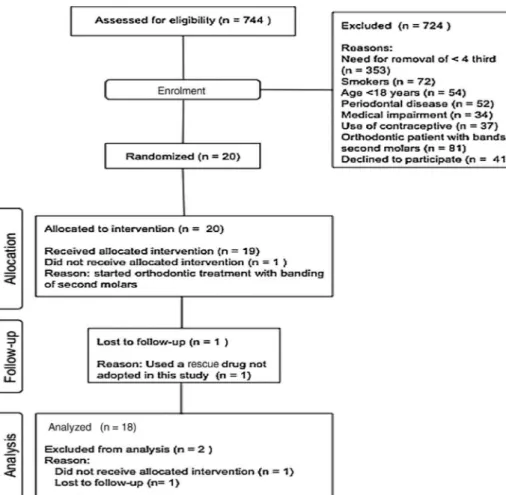
Thecompositionofthefinalsampleinthe presentstudywasinaccordancewiththe characteristics of clinical trials using ‘split-mouth’ as the study design. The experimentalunitsrandomlyallocatedto interventions in split-mouth models are expressed by divisions of the mouth (e.g.dentalarches/sides),allowingbetter controlofindividualbiologicalresponses withareducednumberofrecruited indi-viduals. A total of 744 patients were assessed for eligibility in this study (Fig.2);724didnotmeetthestudy crite-ria,onewasremovedbecauseorthodontic treatmentwasstartedwithbandingofthe secondmolars,andonedidnotreturnfor follow-up. Amongthe excludedpersons,
therewerecaseswithoverlapping exclu-sioncriteria.Thus,anorderofprioritywas adoptedfortheexclusioncriteria.
The study sample comprised 18 patients.There were16females(88.9%) andtwomales(11.1%)andtheyrangedin age from 18 to 35 years (mean age 194.4 years). Thelower third molars (n=36) were characterized as 1A (n=16), 1B (n=10), 2A (n=4), and 2B(n=6)accordingtothePelland Gre-goryclassification (P>0.05;Chi-square test),andashorizontal (n=2), mesioan-gular (n=16), and vertical (n=18) according to the Winter classification (P>0.05; Chi-square test). The upper third molars(n=36) were characterized as A (n=22), B (n=8), and C (n=6) accordingtothePellandGregory classi-fication(P>0.05;Chi-squaretest),andas mesioangular (n=2), vertical (n=10), and distoangular (n=24) according to
the Winterclassification (P>0.05; Chi-squaretest).Theaveragedurationof sur-gerywas29.9(7.2)min;extractionson theleftsidetook30.4(7.3)min,while those on the right side took 29.4 (7.3)min.
Painintensity
Comparisonsofpainintensitybetweenthe groups at each observation time point didnotrevealanystatisticallysignificant
difference (Table1). Figure 3 illustrates thechangeinthemeanpostoperativepain scores across the different observation time points of the study (6, 12, 24, 48, and72h,and7days).Thecomparisonof allobservationperiodsamongeachgroup andbetweenthegroupsshoweda statisti-cally significant difference using the Friedman test (P<0.0001). Inthe keto-profengroup,theDunnposthoctest iden-tifiedadifferencebetweenthetimepoints of6hand7days,andbetween 12hand
7days(Fig.4A).Inthenimesulidegroup, a statistically significant difference was found between the time points of 6h and48h,6hand72h,and6hand7days (Fig.4B).
Timetorescueanalgesia
After the standardized administration of thestudydrugsinbothgroups,onlyoneof the patients required a drug for rescue analgesia during the observation period
Fig.2. FlowchartofpatientrecruitmentintothisstudyaccordingtotheCONSORTstatement.
Table1. Painintensityscoresoverthestudyperiodfortheketoprofenandnimesulidegroups.
Periodaftersurgery Painscore(meanSD) P-value Test Ketoprofen Nimesulide
6h 2.6111.914a 2.6111.852a,b,c 0.9872 Mann–Whitney 12h 2.8893.085d 2.0002.612 0.4395 Mann–Whitney 24h 1.6672.249 1.2782.191 0.4856 Mann–Whitney 48h 1.6112.547 1.4442.791b 0.5836 Mann–Whitney 72h 0.94441.798 0.88891.937c 0.7707 Mann–Whitney 7days 0.11110.4714a,d 0.22220.6468a 0.5744 Mann–Whitney Total 1.6392.318 1.4072.209 0.4653 Mann–Whitney
P-value <0.0001 <0.0001 Friedman/posthocDunn
SD,standarddeviation.
a
Statisticallysignificantdifferencebetween6hand7days.
b
Statisticallysignificantdifferencebetween6hand48h.
cStatisticallysignificantdifferencebetween6hand72h. d
ofthestudy.Thepatientrequiringarescue drugwasremovedfromtheanalyzed sam-ple because she took a drug other than acetaminophen750mg.
Facialswellingandtrismus
At each observation point, there was no statistically significant difference in
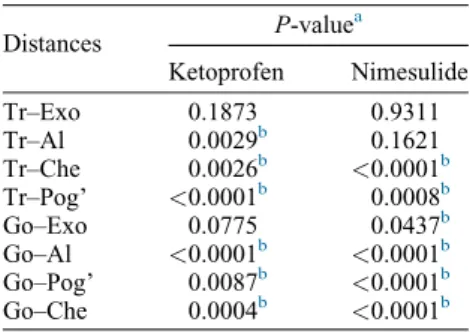
the mean linear distances between thetwostudiedgroups(P>0.05). How-ever, comparing all observation periods between themselves and by group (Table 2), a statistically significant differencewasobservedforthedistances Tr–Al (ketoprofen, P=0.0029), Tr– Che(ketoprofen,P=0.0026;nimesulide P<0.0001), Tr–Pog’ (ketoprofen,
P<0.0001; nimesulide, P=0.0008), Go–Exo (nimesulide, P=0.0437), Go–Al (nimesulide and ketoprofen, P<0.0001), Go–Pog’ (ketoprofen, P=0.0087; nimesulide, P<0.0001), and Go–Che (ketoprofen, P=0.0004; nimesulide,P<0.0001).Table3shows the differences between measurements in the preoperative and postoperative periods.
Withregardtomaximummouth open-ing,there was nostatistically significant difference(P>0.05)betweenthe preop-erative(baseline)andpostoperative peri-ods(24h,72h,and7days)ofobservation when ketoprofen was compared with nimesulide (Table 4). Individually, ketoprofen and nimesulide showed a statistically significant difference in the maximummouth openingwhen the pre-operativevaluewascomparedtothe post-operativeperiods(24h,72h,and7days) (P<0.0001; one-way ANOVA and Tukey post hoc test). For both groups, therewasastatisticallysignificant differ-ence at 24h and 72h after surgery
Fig.3. Meanpainintensityscores(VAS)overthestudyperiod.
Fig.4. Painscores(meanSD)in(A)theketoprofengroup,and(B)thenimesulidegroup;*P<0.05, statisticallysignificantdifference.
Maximummouthopening(meanSD)beforesurgery(baseline)andaftersurgeryin(C)theketoprofengroup,and(D)thenimesulidegroup(the standardwasthepreoperativevalue);*statisticallysignificantdifference(P<0.05)inrelationtothepreoperativemeasurement(ANOVA/Tukey
(P<0.05;t-test)incomparisonwiththe baselinevalueformaximummouth open-ing(Fig.4C,D).Inaddition,therewasa statisticallysignificantdifferencein max-imummouthopeningat72handat7days postoperative (P<0.05; t-test) when comparedwiththe24hpostoperative pe-riod(Fig.4C,D).
Discussion
Themainobjective ofthis researchwas to conduct a study on two COX-2 par-tially selective drugs to compare their analgesic efficacy and to analyze their anti-inflammatoryeffectsthroughathird molarsurgerymodel,withasplit-mouth methodology and without a placebo group. The third molar surgery model was chosen because it has been used widely in pharmacological tests since 197631 and is a procedure commonly performedin dentistryin which postop-erative pain is usually observed in the early stagesafter thesurgical procedur-e.32 This model has been considered important in clinical investigations to
distinguish the analgesic effects of dif-ferentdrugs,asperformedinthisstudy, andevenbetweendifferentdosagesofa single drug.33,34 As some patients have bilaterally impacted third molars, they can be the control for themselves.This study design, known as‘split-mouth’,32 enables adequate control of individual variabilityandrequiresasmallernumber of patients.35 Moreover, we agree with Anderson and Cranswick36 and Merry etal.37abouttheunnecessaryand uneth-ical use of a placebo in studies using drugs withwell-knowneffects.
InBrazil,bothketoprofenand nimesu-lidearedrugsthatareusedwidely follow-ing procedures such as orthopaedic, thoracic, abdominal, and oral surgery, which justifies the interest in studying these two drugs.38–40 In a multicentre prospective study involving nine Italian universities,assessing thelocalprotocols ofthestudyservices,nimesulidewasthe mostprescribedNSAID, usedin68%of thecases,whereasketoprofenwasusedin only9%ofthecases.24Nostudy compar-ing the effects of both of these drugs administeredorallyusingthe methodolo-gyadoptedinthepresentstudyhasbeen publishedtodate.
The efficacyof nimesulide and keto-profeninthecontrolofpostoperativepain afterdentalextractionhasbeenwell de-scribed in clinical trials. Bjornsson etal.,20comparingtheuseofketoprofen 75mg with acetaminophen 1000mg, showed a statistically significant differ-ence between the drugs, with the least amount ofpain inthe groupofpatients who received ketoprofen. De Menezes and Cury,22 comparing nimesulide 100mgandmeloxicam75mg,observed lower pain intensity for the nimesulide group.However,thepresentstudydidnot findanystatisticallysignificantdifference between thedrugs studiedinrelationto painscores.Thisisinagreementwiththe results ofthe studyby Seymouret al.,8 who evaluated the analgesicefficacy of different doses ofketoprofen (12.5 and 25mg) and acetaminophen (500 and 1000mg). Likewise,Leone et al.41 did not find any statistical difference when comparing ketoprofen with methylpred-nisoloneinthecontrolofpainfollowing third molar surgery, even though these drugs are from different groups and have differentactions, which highlights thegoodefficacyofketoprofen. Further-more,thegreatestpainintensityoccurred withinthefirst12hwiththeuseofboth drugsinthisstudy,whichisinagreement with the results of De Menezes and Cury.22Inparticular,itwasobservedthat
Table2. Assessmentofpostoperative swell-ing:P-valuesfordifferencesinmeasurements between thepreoperativeand all postopera-tiveperiods.
Distances P-value
a
Ketoprofen Nimesulide Tr–Exo 0.1873 0.9311 Tr–Al 0.0029b 0.1621 Tr–Che 0.0026b <0.0001b
Tr–Pog’ <0.0001b 0.0008b
Go–Exo 0.0775 0.0437b
Go–Al <0.0001b <0.0001b
Go–Pog’ 0.0087b <0.0001b
Go–Che 0.0004b <0.0001b
Tr–Exo,tragustotheexternalcornerofthe eye; Tr–Al, tragus to the nasal border; Tr–Che, tragus to the labial commissure; Tr–Pog’, tragus to the soft pogonion; Go–Exo,angleofthemandibletotheexternal corneroftheeye;Go–Al,angleofthe mandi-bletothenasalborder;Go–Pog’,angleofthe mandibletothesoftpogonion;Go–Che,angle ofthemandibletothelabialcommissure.
a
Friedman/posthocDunntest.
bStatisticallysignificantdifference.
Table3. Differencesinthefacialdistancemeasurementstakenbeforesurgeryincomparisonto postoperativevalues.
Distances Differenceincm(meanSD) P-valuea
Ketoprofen Nimesulide 24h
Tr–Exo 0.050.08 0.030.05 0.2576 Tr–Al 0.170.50 0.180.19 0.9356 Tr–Che 0.350.25 0.330.29 0.5112 Tr–Pog’ 0.380.34 0.330.32 0.3627 Go–Exo 0.210.33 0.120.26 0.4090 Go–Al 0.330.33 0.300.33 0.9235 Go–Pog’ 0.140.29 0.280.26 0.1637 Go–Che 0.380.28 0.330.94 0.5033 72h
Tr–Exo 0.040.15 0.010.10 0.2863 Tr–Al 0.890.32 0.120.12 0.2313 Tr–Che 0.250.28 0.250.26 0.7000 Tr–Pog’ 0.330.27 0.280.27 0.4718 Go–Exo 0.120.35 0.070.25 0.6295 Go–Al 0.240.30 0.220.28 0.8978 Go–Pog’ 0.060.24 0.120.23 0.7347 Go–Che 0.270.32 0.240.91 0.7484 7days
Tr–Exo 0.020.15 0.020.08 0.9151 Tr–Al 0.330.42 0.080.13 0.1026 Tr–Che 0.890.26 0.090.16 0.6861 Tr–Pog’ 0.070.23 0.090.20 0.6015 Go–Exo 0.030.09 0.010.20 0.7558 Go–Al 0.030.09 0.000.17 0.2135 Go–Pog’ 0.020.07 0.000.12 0.1448 Go–Che 0.040.17 0.050.82 0.9487 SD,standarddeviation;Tr–Exo,tragustotheexternalcorneroftheeye;Tr–Al,tragustothe nasalborder;Tr–Che,tragustothelabialcommissure;Tr–Pog’,tragustothesoftpogonion; Go–Exo,angleofthemandibletotheexternalcorneroftheeye;Go–Al,angleofthemandibleto thenasalborder;Go–Pog’,angleofthemandibletothesoftpogonion;Go–Che,angleofthe mandibletothelabialcommissure.
thepainscoreswerethesameforthetwo drugsat6h,butdifferentat12h. Bjorns-sonetal.20observedasimilarpain inten-sity reduction between 4 and 9h after surgeryintheketoprofengroup,differing fromSeymouretal.8whofoundthatthe reductionin painscores occurredat1h afterthesurgicalprocedure.
Inthe present study, both drugs were administeredimmediatelyafterthe surgi-calprocedureandtheuseofrescue med-ications for pain was found to be unnecessary. This is in contrast to the studies by Seymour et al.8 and Olmedo et al.21 Theresults ofthe present study suggest that nimesulide and ketoprofen controlpainattherapeuticdosesandthat theroutineuseofadditionalpostoperative analgesics is unnecessaryin third molar surgery.Levrinietal.24observedthat75% ofpatientsusedrescuemedicationduring theearlyonsetofpain(3hafterthe surgi-cal procedure) and that 24% ofpatients usedrescuemedicationimmediatelyafter thesurgicalprocedure.
Inthe studyby Levrini etal.,24 those patientswhousedthedrugaftertheonset of pain experienced their peak pain at around 4h and 10min after surgery; in contrast,thepeakmaximumpainoccurred at6hand30minaftersurgeryinpatients whoreceivedmedicationbeforetheonset of pain. Considering the time intervals assessed inthe presentstudytoevaluate postoperative pain (6, 12, 24, and 48h, and7days),thepeakinpainoccurred at 6h after the surgical procedure in the nimesulide groupand at 12h postopera-tivelyintheketoprofengroups.Thepain values decreased significantly after the sixthhourpostoperativeinthenimesulide group, whereas in the ketoprofen group the paindecreasedsignificantly after the 12th postoperative hour. In addition, nimesulide showed lowerpain scores at the24h,48h,and72hintervalsthanthe
ketoprofen group,demonstrating abetter analgesic efficacy in comparison with ketoprofen.Thesedatashowthatalthough completepainreliefwasnotobserved,the pain level was tolerable to patients and theydidnotrequirerescuemedication.
Regarding oedema, a significant in-creasewasobservedinthefirst24hafter thesurgicalprocedureforbothdrugs eval-uated,whereasinthestudiesofTroullos et al.42 andDeMenezesandCury,22 the maximum swelling occurred at48h and 72h,respectively, aftertheextractionof thethirdmolars.Therewasnostatistically significantdifferencewhenthegroupsin thisstudywerecomparedwitheachother, whichisincontrasttotheresultsfromthe study ofBjornssonetal.20;theyfounda statisticallysignificantreductionin swell-ing on the third and sixth postoperative days for the ketoprofen group. In that study,thereductioninswellingwith keto-profen use was 27.8% onthe third day, increasing to 70.8%on the sixthday of observation.DeMenezesandCury22 ob-served that the group using nimesulide (100mgtwiceaday)hadlesspronounced swelling compared to the meloxicam group (7.5mg twice a day) during the periodsstudied.Nostatisticallysignificant difference in swelling was observed be-tween the nimesulide and ketoprofen groupsinrelationtotheassessedinterval periodsinthepresentstudy.
Inbothgroupsstudied, P-values were lessthan0.05forthedifferencesin mea-surementsbetweenthepreoperative peri-od and the postoperative period for six facialmeasurements.Additionally,fiveof them(Tr–Pog’,Tr–Che,Go–Al,Go–Pog’, and Go–Che)showed P-values lessthan 0.0001. InthestudybyDeMenezesand Cury,22thedistanceGo–Chewasthemost affected. Theseauthorsobserved statisti-cally significant differences for nimesu-lideincomparisonwithmeloxicaminthe
Go–Exo distance at 24h postoperative, the Go–Exo and Go–Pog’ distances at 48h postoperative, and the Go–Exo, Go–Al,Go–Che,and Go–Pog’distances at72hpostoperative. Thesefindings are not supported by the present research, since at 72h nimesulide did not show any statistically significant difference compared to ketoprofen for all facial swellingmeasurements.
Theassessmentoftrismuswasdoneby measuring the difference in maximum mouthopeningbetweenthepostoperative and preoperative periods. A decrease in mouthopeningwas observed inthefirst 72haftersurgerybothinthisstudyandin thestudyperformedbyDeMenezesand Cury.22However,inthisstudytherewas nostatisticallysignificantdifferenceinthe comparisonbetween the nimesulide and ketoprofengroups.Asignificantincrease inmouthopeningoccurredat72handat7 daysaftersurgeryinthepatientsofboth groups.Thiswasalsofoundinthestudyof DeMenezes and Cury,22 whose patients usednimesulide,aswellasinthestudyof Bjornsson et al.,20 whose patients used ketoprofen.
Several pharmacological studies have aimed to investigate the tolerability of differentdrugs.Olmedoetal.21recruited patients to analyze the drug safety of ketorolacandketoprofen.Adverseeffects were transient in all patients who pre-sented one, and noneof thepatients re-quiredadjuvanttreatment.Inthestudyby Olmedo et al.,21 37.3% of the patients reportedsometypeofadverseeffect,with drowsiness being the most prevalent (10.7%ofcases),followedbygastric dis-turbances(8%)anddizziness(5.3%).The most prevalent adverse effect related to ketoprofen was pyrosis (10.3%). Three seriousadverse effects werereported by Olson et al.,19 with twoof these events related to ibuprofen and one related to acetaminophen. No adverse effect, such asgastrointestinal discomfort, dizziness, ornausea,wasrelatedtotheuseof keto-profen in this study. Bjornsson et al.20 statedthattheadverseeffectsthatdeserve specialattentionarethoseassociatedwith the gastrointestinal tract (stomach ache anddiarrhoea).Inthatstudy,alladverse effects were reported to be of mild to moderateintensity.20Ketoprofenand oth-er strongNSAIDs have been associated withariskofgastricirritation.43–45Unlike thosestudies,noneofthepatients evalu-ated in the present clinical trial experi-encedadverseeffectsrelatedtotheuseof drugsduringthestudyperiod.Thisfactis probablyduetotheshortperiod(3days) thatwasadoptedinthemethodology.Itis
Table 4. Comparison ofmaximummouthopening (meanSD) assessedbeforeand after surgeryintheketoprofenandnimesulidegroups.Thestandardparameterwasthepreoperative (baseline)measurementofmaximummouthopening(mm).
Timeaftersurgery
Maximummouthopening (meanSD)
P-value Test Ketoprofen Nimesulide
0(baseline) 42.833.2 43.113.6 0.8096 t-Test 24h 29.566.8a 33.117.9a 0.1580 t-Test 72h 36.477.0a,b 37.367.6a,b 0.7168 t-Test 7days 40.396.2b 40.616.4b 0.9162 t-Test
P-value <0.0001 <0.0001 One-wayANOVA
SD,standarddeviation;ANOVA,analysisofvariance.
a
Statisticallysignificantdifference(P<0.05)inrelationtothepreoperativemeasurement
(baseline);ANOVA/Tukeyposthoctest.
bStatisticallysignificantdifference(
P<0.05)inrelationtothe24hpostoperative
reasonable to assume that a relatively shortdurationoftheketoprofendrug regi-menrepresentsalimitedrisktothepatient who has had no previous experience of gastrointestinal problems orreactions to otherNSAIDs.20
De Menezes and Cury22 described no adverseeffectsinpatientswhoused nime-sulide. In a review of hepatic adverse effects, agreaternumberandseverityof hepatotoxicevents wasdemonstratedfor patientswhousednimesulideinrelationto otherNSAIDs.45Macio´etal.45foundthat thepatientswithahigherriskof hepato-toxicity with nimesulideuse wereolder, female,andhadamedianof62daysusing this drug. Different from that work, the patients in the research by De Menezes andCury22andinthepresentstudywere younger (average age around 20 years) andusednimesulideforaveryshort peri-odoftime.
Thepresentresearchwasacomparative study of ketoprofen and nimesulide ad-ministeredorallyfollowingsurgeryforthe removal of third molars. In summary, patients who received ketoprofen 100mg or nimesulide 100mg showed goodcontrolofpain,swelling,andtrismus aftertheextractionofthethirdmolars.
Funding
None.
Competinginterests
Nonedeclared.
Ethicalapproval
This study was approved by the Ethics CommitteeoftheWalterCantı´dio Univer-sityHospital,Ceara´,Brazil(protocol num-ber 084.08.11) and was conducted in accordancewiththeHelsinkistatements.
Patientconsent
Thepatientprovidedinformedconsentfor theuseofthedataandthephotographin thispublication.
References
1. Seymour RA,MeechanJG, BlairGS. An investigation intopost-operativepainafter thirdmolarsurgeryunderlocalanalgesia.Br JOralMaxillofacSurg1985;23:410–8.
2. ClauserC,BaroneR.Effectofincisionand flapreflectiononpostoperativepainafterthe removal of partially impacted mandibular third molars. Quintessence Int 1994;25:
845–9.
3. Berge TI, EgilO. Predictorevaluation of postoperative morbidity after surgical re-moval of mandibular third molar. Acta OdontolScand1994;52:162–9.
4. McGrathC,ComfortMB,Lo EC,LuoY. Changesinlifequalityfollowingthirdmolar surgery–theimmediatepostoperative peri-od.BrDentJ2003;194:265–8.
5. Colorado-Bonnin M, Valmaseda-Castello´n E, Berini-Ayte´sL,Gay-Escoda C.Quality oflifefollowinglowerthirdmolarremoval.
Int J Oral Maxillofac Surg 2006;35:
343–7.
6. SortinoF,MessinaG,PulvirentiG. Evalua-tionofpostoperativemucosaandskin tem-perature after surgery of impacted third molar.MinervaStomatol2003;57:393–9.
7. Markovic AB,Todorovic L. Postoperative analgesia afterlower third molarsurgery: contributionoftheuseoflong-actinglocal anesthetics,low-powerlaseranddiclofenac.
Oral Surg Oral Med Oral Pathol Oral RadiolEndod2006;12:e4–8.
8. SeymourRA,KellyPJ,HawkesfordJE.The efficacy of ketoprofen and paracetamol (acetaminophen)inpostoperativepainafter thirdmolar surgery.Br JClinPharmacol
1996;41:581–5.
9. RainsfordKD.Nimesulide:amultifactorial approachtoinflammationandpain: scientif-ic and clinical consensus. Curr Med Res Opin2006;2:1161–70.
10. BinningA.Nimesulideinthetreatmentof postoperativepain:adouble-blind, compar-ative study in patients undergoing arthro-scopickneesurgery.ClinJPain2007;23:
565–70.
11. FerrariA,PasciulloG,SavinoCiceroAF, OttaniA,BertoliniA,SternieriE.Headache treatmentbeforeandaftertheconsultationof aspecializedcenter:a pharmacoepidemiol-ogystudy.Cephalalgia2004;24:356–62.
12. PohjolainenT,JekunenA,AutioL,Vuorela H.Treatmentofacutelowbackpainwiththe COX-selective anti-inflammatory drug nimesulide: results ofa randomized, dou-ble-blindcomparativetrialversusibuprofen.
Spine(PhilaPa1976)2000;25:1579–85.
13. WoberW.Comparativeefficacyandsafety ofnimesulideanddiclofenacinpatientswith acuteshoulder,andameta-analysisof con-trolledstudieswithnimesulide. Rheumatol-ogy(Oxford)1999;38:33–8.
14. BianchiM,BrogginiM.Arandomised, dou-ble-blind,clinicaltrialcomparingthe effica-cyofnimesulide,celecoxibandrofecoxibin osteoarthritis of theknee.Drugs2003;63:
37–46.
15. BianchiM,BrogginiM.Anti-hyperalgesic effects of nimesulide: studies in rats and humans.IntJClinPract2002;128:11–9.
16. JamaliF,BrocksDR.Clinical pharmacoki-netics of ketoprofen and its enantiomers.
ClinPharmacokinet1990;19:197–217.
17. FossgreenJ.Ketoprofen–asurveyofcurrent publications. Scand J Rheumatol1976;14:
7–32.
18. Kantor TG. Ketoprofen: a review of its pharmacologicandclinicalproperties. Phar-macotherapy1976;6:93–103.
19. OlsonNZ,OteroAM,MarreroI,TiradoS, CooperS,DoyleG,etal.Onsetofanalgesia for liquigelibuprofen 400mg, acetamino-phen1000mg,ketoprofen25mg,and pla-cebointhetreatmentofpostoperativedental pain.JClinPharmacol2001;41:1238–47.
20. BjornssonGA,HaanaesHR,SkoglundLA. Ketoprofen75mgqidversusacetaminophen 1000mgqidfor3daysonswelling,painand otherpostoperativeeventsafterthirdmolar surgery.JClinPharmacol2003;43:305–14.
21. OlmedoMV,Ga´lvezR,VallecilloM. Dou-ble-blind parallel comparison of multiple dosesofketorolac,ketoprofenandplacebo administeredorallytopatientswith postop-erativedentalpain.Pain2001;90:135–41.
22. DeMenezesSA,CuryPR.Efficacyof nime-sulideversus meloxicamin thecontrol of pain,swellingandtrismusfollowing extrac-tionofimpactedlowerthirdmolar.IntJOral MaxillofacSurg2010;39:580–4.
23. SeymourRA,WatkinsonH,HawkesfordJE, MooreU.Theefficacyofbuffered ketopro-fen inpostoperativepainafterthirdmolar surgery. Eur J Clin Pharmacol 2006;55:
801–6.
24. LevriniL,CarraroM,RizzoS,SalgarelloS, BertelliE, PelliccioniGA, etal. Prescrip-tionsofNSAIDstopatientsundergoingthird molarsurgery:anobservational,prospective, multicentresurvey.ClinDrugInvest2008;
28:657–68.
25. Pierleoni P, TonelliP, ScaricabarozziI.A double-blindcomparisonofnimesulideand ketoprofen in dental surgery. Drugs
1993;46:168–70.
26. MoherD,HopewellS,SchulzKF,Montori V,GøtzschePC,DevereauxPJ,etal. CON-SORT 2010 explanation and elaboration: updated guidelines for reporting parallel grouprandomised trials.JClinEpidemiol
2010;63:e1–37.
27. BezerraTP,Studart-SoaresEC,ScaparoHC, Pita-NetoIC,BatistaSH,FontelesCS. Pro-phylaxisversusplacebotreatmentfor infec-tive and inflammatory complications of surgicalthirdmolarremoval:asplit-mouth, double-blind, controlled,clinical trialwith amoxicillin (500mg). J Oral Maxillofac Surg2011;69:e333–9.
28. PellGJ,GregoryBT.Impactedmandibular third molars: classification and modified techniquesforremoval.DentDig1933;39:
330–8.
29. WinterGB.Principlesofexodontiaapplied to the impacted mandibular third molar. SaintLouis:AmericanBooks;1926.
30. Ong KS,SeymourRA, ChenFG,HoVC. Preoperativeketorolachasapreemptiveeffect forpostoperativethirdmolarsurgicalpain.Int JOralMaxillofacSurg2004;33:771–6.
31. CooperSA,BeaverWT.Amodeltoevaluate mildanalgesicsinoralsurgeryoutpatients.
32. MeechanJG,SeymourRA.Theuseofthird molarsurgeryinclinicalpharmacology.BrJ OralMaxillofacSurg1993;31:360–5.
33. ForbesJA.Oralsurgery.In:MaxME, Por-tenoyRK,LaskaEM,editors.Advancesin pain researchand therapy.The designof analgesicclinicaltrials.NewYork:Raven Press;1991.p.347.
34. VanAkenH,ThysL,VeekmanL,BuerkleH. Assessinganalgesiainsingleandrepeated administrationsofpropacetamolfor postop-erativepain:comparisonwithmorphineafter dental surgery. Anesth Analg 2004;98:
159–65.
35. LesaffreE,GarciaZatteraMJ,RedmondC, HuberH,NeedlemanI,ISCBSubcommittee onDentistry.Reportedmethodological qual-ityofsplit-mouthstudies.JClinPeriodontol
2007;34:756–61.
36. AndersonB,CranswickN.Theplacebo(I shallplease)–isitsopleasinginchildren?
PediatrAnaesth2005;15:809–13.
37. MerryAF,GibbsRD,EdwardsJ,TingGS, Frampton C, Davies E, et al. Combined acetaminophenandibuprofenforpainrelief after oralsurgeryin adults:a randomized controlled trial. Br J Anaesth 2010;104:
80–8.
38. ArraisPS,CoelhoHL,BatistaMC,Carvalho ML,RighiRE,ArnauJM.Profileof self-medication in Brazil. Rev Saude Publica
1997;31:71–7.[inPortuguese].
39. PereiraFS,BucarethiF,StephanC,Cordeiro R.Self-medication inchildrenand adoles-cents.JPediatr(RioJ)2007;83:453–8.
40. CastilhoLS,Paixa˜oHH,PeriniE. Prescrip-tion patternsof drugsof systemicuse by dentists. Rev Saude Publica 1999;33:
287–94.
41. LeoneM,RichardO,AntoniniF,Rousseau S,ChabaaneW,GuyotL,etal.Comparison ofmethylprednisoloneandketoprofenafter multiplethirdmolarextraction:a random-izedcontrolledstudy.OralSurgOralMed Oral Pathol Oral Radiol Endod 2007;
103:e7–9.
42. Troullos ES, Hargreaves KM, Butler DP, Dionne RA. Comparison of nonsteroidal anti-inflammatorydrugs,ibuprofenand flur-biprofen,withmethylprednisoloneand pla-ceboforacutepain,swelling,andtrismus.J OralMaxillofacSurg1990;48:945–52.
43. Henry D, Lim LL, Rodrigues LA, Perez Gutthann S, Carson JL, Griffin M, et al. Variabilityinriskofgastrointestinal compli-cations with individual non-steroidal
anti-inflammatorydrugs:resultsofa collab-orativemeta-analysis.BrMedJ1996;312:
1563–6.
44.Lanza FL, Codispotti JR,NelsonEB. An endoscopic comparison of gastroduodenal injurywithover-the-counterdosesof keto-profenandacetaminophen.AmJ Gastroen-terol1998;93:1051–4.
45.Macio´ MA,CarvajalA,VeraE. Hepatotox-icityassociatedwithnimesulide:datafrom theSpanishpharmacovigilancesystem.Clin PharmacolTher2001;72:696–7.
Address:
Fa´bioWildsonGurgelCosta PostgraduatePrograminDentistry FederalUniversityofCeara´ RuaMonsenhorFurtado RodolfoTeo´filo Fortaleza Ceara´ 60430-350