w w w . r b o . o r g . b r
Original
Article
Anatomical
study
on
the
relationship
between
the
dorsal
root
ganglion
and
the
intervertebral
disc
in
the
lumbar
spine
夽
Emiliano
Vialle
∗,
Luiz
Roberto
Vialle,
William
Contreras,
Chárbel
Jacob
Junior
HospitalUniversitárioCajuru,PontifíciaUniversidadeCatólicadoParaná,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received28May2014 Accepted1August2014 Availableonline3July2015
Keywords:
Spine/anatomyandhistology Spinalganglia
Minimallyinvasivesurgical procedures
a
b
s
t
r
a
c
t
Objective:Todescribethelocationofthedorsalrootganglioninrelationtotheintervertebral disc,includingthe“triangular”safetyzoneforminimallyinvasivesurgeryinthelumbar spine.
Methods:Eight adult cadavers were dissected bilaterally in the lumbar region, using a posterolateralapproach,soastoexposetheL3L4andL4L5spaces,therebyobtaining mea-surementsrelatingtothespacebetweentheintervertebraldisc,pediclescranialandcaudal tothedisc,pathofthenerveroot,dorsalganglionandsafetytriangle.
Results:The measurements obtained were constant, without significant differences betweenlevels oranylaterality. Thedorsalganglionoccupied thelateralborderofthe triangularsafetyzoneinallthespecimensanalyzed.
Conclusion:Preciselocalizationoftheganglionshowsthatthesafetymarginforminimally invasiveproceduresislessthanwhatispresentedinstudiesthatonlyinvolve measure-mentsofthenerveroot,thusperhapsexplainingthepresenceofneuropathicpainafter someoftheseprocedures.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Estudo
anatômico
da
relac¸ão
do
gânglio
da
raiz
dorsal
com
o
disco
intervertebral
na
coluna
lombar
Palavras-chave:
Colunavertebral/anatomia& histologia
Gângliosespinais Procedimentoscirúrgicos minimamenteinvasivos
r
e
s
u
m
o
Objetivo:Descreveralocalizac¸ãodogângliodaraizdorsalemrelac¸ãoaodiscointervertebral, incluindoazona“triangular”deseguranc¸aparacirurgiaminimamenteinvasivanacoluna lombar.
Métodos:Oitocadáveresadultosforamdissecadosbilateralmente,naregiãolombar,coma abordagemposterolateral,atéexposic¸ãodosespac¸osL3L4eL4L5eseobtiverammedidas referentesaoespac¸oentreodiscointervertebral,ospedículoscranialecaudalaodisco,o trajetodaraiznervosa,ogângliodorsaleotriângulodeseguranc¸a.
夽WorkperformedintheDepartmentofAnatomy,MedicalCourse,PontifíciaUniversidadeCatólicadoParaná,Curitiba,PR,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](E.Vialle).
http://dx.doi.org/10.1016/j.rboe.2015.06.013
Resultados: Asmedidasobtidasforamconstantes,semdiferenc¸assignificativasentreníveis oulateralidade.Ogângliodorsalocupouabordalateraldazonatriangulardeseguranc¸aem todososespécimesanalisados.
Conclusão:Alocalizac¸ãoprecisadogângliomostraqueamargemdeseguranc¸apara proced-imentosminimamenteinvasivosémenordoqueaapresentadanosestudosqueenvolvem apenasmedidasdaraiznervosa,oqueexplicatalvezapresenc¸adedorneuropáticaapós algunsdessesprocedimentos.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Advancesinsurgicaltreatmentsfordegenerativepathological conditions,andspecificallyinrelationtominimallyinvasive surgeryforthelumbarspine,havegivenrisetotheneedto reassessprevious concepts ofsurgical anatomy, giventhat new accesses that are less invasive have been developed. Minimallyinvasiveapproacheshavetheadvantageoftissue preservation, reduction ofunnecessary damage to healthy areas,accelerationofhealingandreductionofthedurationof treatment.1–3However,theseapproachesdonotalwaysenable
directviewingoftheneuralstructuresanditisatthispoint thatreviewinganatomicalknowledgebecomesimportant.
Thedorsalnerverootsarecomposedonlyofsensoryfibers comingfromthespinalnervesthatheadtowardthe spinal cord.Theventralnerverootsaremostlycomposedofmotor fibers,but they may transporta small quantity ofsensory fibers.Closetothejunctionbetweenthedorsalandventral roots,thedorsalrootpresentsadilatationknownasthe dor-salrootganglion(DRG),4whichconsistsofagroupingofcell
bodiesofsensoryfibers.TheDRGsarelocatedinthe interver-tebralforamina,exceptforthesacralDRGs,whicharelocated insidethevertebralcanal,andthecoccygealDRGs,whichare intradural.4–6
TheDRG differsfromthenerverootsinthatitis sensi-tivetomechanicalpressureevenintheabsenceofchemical irritation, since it contains a large number of nociceptors thataremechanicallymoresensitive.Moreover,itmayhave greaterchanceofcausingneuropathicpainifitisinjured.4,5,7
Neuropathicpainisastateofneuraldysfunctionprovoked byfunctional and structuralalterations to the central and peripheralsensorypathways,whichproducemodificationsto theprocessingofthenociceptiveinformation.Itcanbecaused byinjuriestotheroots,DRGs,spinalcordorencephalon.8,9
Transforaminalintersomaticarthrodesisortransforaminal lumbarinterbodyfusion(TLIF)wasdevelopedtoenableaccess tolumbarintervertebraldiscsbymeansofaunilateral extra-canalroute,thereby avoiding theproblemsand limitations oftheoriginaltechnique(posteriorlumbarinterbodyfusion, PLIF).OneofthecomplicationsrelatingtousingTLIFthathas beenreportedintheliteratureisthepresenceofneuropathic painsubsequenttothesurgery.Thishasbeenattributedto excessivemanipulationofthedorsalganglionoftheemerging root.10–12
Inviewofthesparsenessoftheliteratureontheanatomy ofthedorsalganglion,asappliedtotheTLIFtechnique,we
conductedastudyoncadavers,withtheaimofdetermining thesafestareaforundertakingatransforaminalapproachfor treatinglumbarintervertebraldiscs,withemphasisontheir anatomicalrelationshipwiththedorsalganglion.
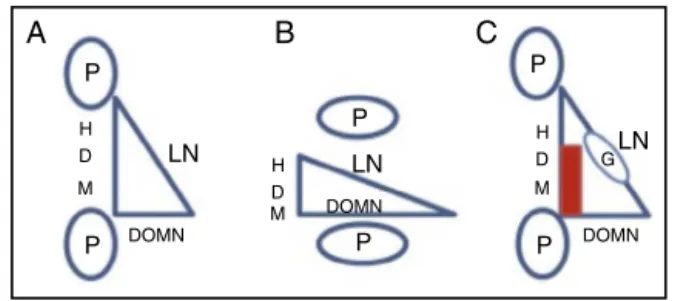
The“triangularsafetyzone”isconsideredtobeasafearea foraccessingtheintervertebraldiscsofthelumbarspine.This zonewasfirstdefinedbyMirkovicetal.,13withitslaterallimit
astheduramater,itslowerlimittheuppervertebralplateau anditshypotenusethelumbarroot.Inthiszone,the interver-tebraldisccanbeaccessedwithoutputtingthesurrounding neuralstructuresatrisk.ThepositionoftheDRGisnot men-tionedinthistriangleand,becauseofitsovalshape,itmay reducethelaterallimitsoftheareaofsafetyforminimally invasiveapproaches.12,13
Thepresentstudyhadtheaimofdescribingthelocation oftheDRGinrelationtotheintervertebraldisc,includingthe “triangular”safetyzoneforminimallyinvasivesurgeryonthe lumbarspine.
Methods
Thisstudywasconductedinourinstitution’sDepartmentof HumanAnatomy.Eightcadaverswithoutanyprevious scar-ringonthelumbarspinewerestudied.Theywere allmale, ranginginagefrom45to62years(mean:54).Thenumber ofcadaverswasdefinedbytheinstitutionbycalculatingthe variabilityofthesample.
The cadavers were positioned in ventral decubitus and a posterior accessroute ina single layerwas constructed. Extensive laminectomywasthen performedonthelumbar spine,toexpose theduralsac, thelumbarrootswiththeir respective DRGs, the pedicles and the intervertebral discs (Fig.1).ThesegmentL5-S1was notstudiedbecauseofthe needformoreextensivedissectionandpossibledamagetothe anatomicalspecimen.Usingastraightosteotome,osteotomy was performed on the joint facets and lateral recess, and theanatomicalstructuresoftheintervertebralforamenwere viewed.
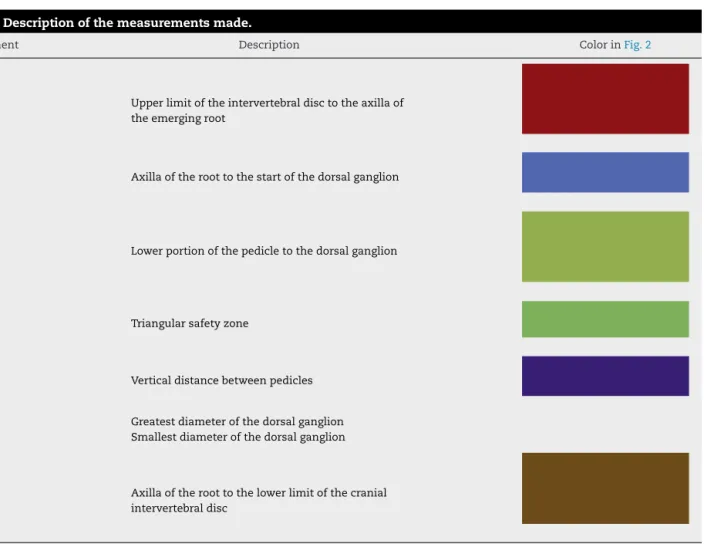
Using a digital pachymeter(Mistainless®), the following measurementsinmillimetersweremade(Table1,Fig.2):
(1) Upperlimitoftheintervertebraldisctotheaxillaofthe emergingroot;
Table1–Descriptionofthemeasurementsmade.
Measurement Description ColorinFig.2
1 Upperlimitoftheintervertebraldisctotheaxillaof theemergingroot
2 Axillaoftheroottothestartofthedorsalganglion
3 Lowerportionofthepedicletothedorsalganglion
4 Triangularsafetyzone
5 Verticaldistancebetweenpedicles
6 Greatestdiameterofthedorsalganglion
7 Smallestdiameterofthedorsalganglion
8 Axillaoftheroottothelowerlimitofthecranial intervertebraldisc
(4) Triangularsafetyzone(height,baseandhypotenuse): Heightofthetriangle:lateralborderoftheduramater; Base:uppervertebralplateauofthelowervertebra; Hypotenuse:spinalnerve;
(5) Verticaldistancebetweenpedicles; (6) Greatestdiameterofthedorsalganglion; (7) Smallestdiameterofthedorsalganglion;
Pedicle DRG*
DRG*
DRG* Dural sac
Pedicle
Nerve root Nerve
root ID** Pedicle
Fig.1–Anatomicalexposureofthenerveroot,
intervertebraldisc(ID),dorsalrootganglion(DRG),pedicle andduralsac.
(8) Axillaoftheroottothelowerlimitofthecranial interver-tebraldisc.
Results
The data and the results obtained are summarized in
Tables2and3.
Inallthespinesevaluated,theDRGtouchedorenteredthe limitsofthetriangularsafety zoneandthuswasshownto beariskfactorforproceduresthatcomeclosetothisregion. Anotherfactorthatemphasizesthecloserelationshipofthe DRGwiththetriangularsafetyzoneistheratioofitsheight (around15mm)tothegreatestlengthoftheDRG(7.5mm).If theportionofthetriangularzonerelatingtothecranial pedi-cleandthevertebralbody(around8mm)isexcluded,itcan beseenthattheremainderoftheexternalborderofthe tri-angularzonenecessarilyendsupbeingoccupiedbytheDRG (Fig.2).
Discussion
Table2–Meansofthevaluesobtainedinthestudy.
Measurement Description Mean(mm)
1 Upperlimitoftheintervertebraldisctotheaxillaoftheemergingroot 14.65
2 Axillaoftheroottothestartofthedorsalganglion 7.95
3 Lowerportionofthepedicletothedorsalganglion 5.45
4 Triangularsafetyzone Table3
5 Verticaldistancebetweenpedicles 15.25
6 Greatestdiameterofthedorsalganglion 13.25
7 Smallestdiameterofthedorsalganglion 7.05
8 Axillaoftheroottothelowerlimitofthecranialintervertebraldisc 8.0
8
2
5
3
1
6.7
Fig.2–Measurementsmadeduringthestudy.1,upper limitoftheintervertebraldisctotheaxillaoftheemerging root;2,axillaoftheroottothestartofthedorsalganglion; 3,lowerportionofthepedicletothedorsalganglion;4, greentriangulararea:triangularsafetyzone;5,vertical distancebetweenpedicles;6and7,diameteroftheDRG;8, axillaoftheroottothelowerlimitofthecranial
intervertebraldisc.
MoststudieshavedescribedtheDRGasanovalstructure thatisalmostentirelylocatedwithinthe foraminaat lum-barlevels,10,11buttheydonotdescribethesafetylimitsforit.
Thisknowledgeisofgreatimportanceforminimallyinvasive proceduresonthespine.
ThetriangularsafetyzonewasfirstdescribedbyMirkovic et al.,13 who definedit as a space inthe foraminalregion
thatwouldmakeitpossibletointroducecannulaefor pos-terolateral percutaneous procedures in the lumbar region,
Table3–Measurementofthetriangularsafetyzone.
Measurement L3left L3right L4left L4right
Base(mm) 14.25 13.75 14.55 14.17
Height(mm) 14 16.55 17.52 16.4
Hypotenuse(mm) 18.98 21.53 23.03 21.72
without putting the surrounding neural structures at risk. TherewasnomentionofthepositionoftheDRGinthatinitial report.13–15
The triangle constructed from the data of Choi et al.15
presentedanatomicalcharacteristicsthatdifferedfromthose describedbyMirkoviketal.13inrelationtoheightandwidth.
However,thegeneralmeanofthehypotenuseofthetriangular safetyzonewasconcordant.Theyobtainedameanof23mm versus25.49mminthestudybyMirkovik,butneitherofthese studiesmadeanymentionofthepositionoftheDRG.
Kambinetal.14describedthesafetylimitsofpercutaneous
proceduresforaccessingintervertebraldiscs,with introduc-tionofinstrumentsatadistanceof10cmfromthemidline andinparallelwiththevertebralplateau,withpenetrationof theannulusatateno’clockortwoo’clockposition.Theyalso reportedthelimitationsoftheseprocedures,suchasextruded andsequesteredhernias.
Inthepresentstudy,attentionwaspaidtothesafety lim-itsoftheDRG,whichwaslocated7mmfromtheexitpoint ofthenerveroot,usuallyinalocationwithintheforamina. Thedistancefromtheintervertebraldisctothelowerpartof thenerverootwassufficientforasafeapproach.Thelower pedicle,whichmarksthelowerlimitofthesafetyzone,was located5mmfromtheDRG,i.e.differingfromthefindingsof Mirkovicetal.13andChoietal.15(Fig.3).
Thelimitationofthisstudywasthesmallnumberof spec-imens foranalysis, whichmay have affectedthe valuesof thedatapresented.However,similarstudiesintheliterature thatpresentedlargernumbersoflevelsanalyzedincludedthe
P
B
A
C
P
LN
DOMN
DOMN
DOMN H D M H
D M H
D M
G LN
LN P
P P
P
entirelumbarspine,whichgeneratedwidevariationofroot angles,especially atL2-L3 and L5-S1.15 Furthermore,those
studiesdidnotplaceanyemphasisonthedorsalganglionand itslocation,perhapsforintroductionpointsforendoscopy.In thepresentstudy,wesoughttofindspacesforaccessingthe discinminimallyinvasiveprocedures.
Conclusion
TheDRGinfringes thelaterallimitsofthetriangularsafety zone,inthe intervertebralforamen, and maybeinjured in foraminalproceduressuchasminimallyinvasiveTLIF.We pro-posethatarectangularsafetyzoneshouldbeused,withthe aimofreducingthenerveinjuryandthepresenceof neuro-pathicpaininpercutaneousprocedures.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. ShenJ,WangHY,ChenJY,LiangBL.Morphologicanalysisof normalhumanlumbardorsalrootganglionby3DMR imaging.AJNRAmJNeuroradiol.2006;27(10):2098–103.
2. PotterBK,FreedmanBA,VerwiebeEG,HallJM,PollyDWJr, KukloTR.Transforaminallumbarinterbodyfusion:clinical andradiographicresultsandcomplicationsin100
consecutivepatients.JSpinalDisordTech.2005;18(4):337–46.
3. KimKT,LeeSH,LeeYH,BaeSC,SukKS.Clinicaloutcomesof 3fusionmethodsthroughtheposteriorapproachinthe lumbarspine.Spine(PhilaPA1976).2006;31(12):1351–7.
4.BougdukN,TwomeyLT.Clinicalanatomyofthelumbarspine. Edinburgh:ChurchillLinvigstone;1987.
5.PorterfieldJA,DeRosaC.Mechanicallowbackpain. Perspectivesinfunctionalanatomy.Philadelphia:Saunders; 1998.
6.HasegawaT,MikawaY,WatanabeR,AnHS.Morphometric analysisofthelumbosacralnerverootsanddorsalroot gangliabymagneticresonanceimaging.Spine(PhilaPA1976). 1996;21(9):1005–9.
7.CohenMS,WallEJ,BrownRA,RydevikB,GarfinSR.1990 AcroMedAwardinbasicscience.Caudaequinaanatomy.II: extrathecalnerverootsanddorsalrootganglia.Spine(Phila PA1976).1990;15(12):1248–51.
8.BaronR.Neuropathicpain:thelongpathfrommechanisms tomechanisms-basedtreatment.IntJPainMedPalliatCare. 2001;1(1):2–14.
9.NicholsonBD.Evaluationandtreatmentofcentralpain syndromes.Neurology.2004;625Suppl2:S30–6.
10.RihnJA,PatelR,MakdaJ,HongJ,AndersonDG,VaccaroAR, etal.Complicationsassociatedwithsingle-level
transforaminallumbarinterbodyfusion.SpineJ. 2009;9(8):623–9.
11.HeeHT,CastroFPJr,MajdME,HoltRT,MyersL. Anterior/posteriorlumbarfusionversustransforaminal lumbarinterbodyfusion:analysisofcomplicationsand predictivefactors.JSpinalDisordTech.2001;14(6):533–40.
12.SelznickLA,ShamjiMF,IsaacsRE.Minimallyinvasive interbodyfusionforrevisionlumbarsurgery:technical feasibilityandsafety.JSpinalDisordTech.2009;22(3):207–13.
13.MirkovicSR,SchwartzDG,GlazierKD.Anatomic considerationsinlumbarposterolateralpercutaneous procedures.Spine(PhilaPa1976).1995;20(18):1965–71.
14.KambinP,ZhouL.Historyandcurrentstatusofpercutaneous arthroscopicdiscsurgery.Spine(PhilaPa1976).1996;2124 Suppl:57S–61S.