SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Initial
experience
of
use
of
an
articulated
external
fixator
in
treating
Legg-Calvé-Perthes
disease
by
means
of
arthrodiastasis
during
the
active
phase
of
the
disease
夽
Carlos
Augusto
Malheiros
Luzo,
Roberto
Guarniero
∗,
Nei
Botter
Montenegro,
Rui
Maciel
de
Godoy
Junior
DepartmentofOrthopedicsandTraumatology,SchoolofMedicine,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received22April2015 Accepted25August2015 Availableonline4May2016
Keywords:
Legg-Calvé-Perthesdisease Orthopedicprocedures Externalfixators Hipjoint
a
b
s
t
r
a
c
t
Objective:TopresentthepreliminaryresultsfromtreatingpatientswithLegg-Calvé-Perthes Disease(LCPD)bymeansofhiparthrodiastasisusingamonolateralexternalfixatorapplied tothehipandtosuccinctlydescribethesurgicaltechniqueused,inaprospectivestudy. Methods:Prospectivestudyon18patientswithLCPDwhounderwentsurgicaltreatmentby meansofthehiparthrodiastasistechniqueusingamonolateralexternalfixator.Therewere 13maleandfivefemalepatientsofmeanage8.5years,rangingfromfiveto13years.Allthe patientspresentedunilateralhipimpairment:nineontherightsideandnineontheleft. Theresultswereevaluatedatmaturityusingclinicalandradiologicalcriteria.
Results:Allthepatientsevolvedwithimprovementofjointmobility,andpainreliefwas achievedin88.9%ofthem.Reossificationofthefemoralepiphysisoccurredwithinthefirst threemonthsofthetreatment.Thehipsoperatedatthenecrosisstageofthediseasedid notpassedthroughthefragmentationstage,thusshorteningtheevolutionofthedisease. Theresultswere77.8%satisfactoryand22.2%unsatisfactory.
Conclusion: Hiparthrodiastasiswithamonolateralexternalfixatorduringtheactivephase of LCPDimprovedthe degree ofjointmobility. Useofthe arthrodiastasis techniqueat thenecrosisstageoratthefragmentationstage(activephaseofthedisease)presented satisfactoryresultsfromtreatmentofLCPD.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheDisciplineofPediatric,DepartmentofOrthopedyandTraumatology,FaculdadedeMedicina,Universidadede SãoPaulo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.Guarniero).
http://dx.doi.org/10.1016/j.rboe.2016.04.005
Experiência
inicial
com
o
uso
de
fixador
externo
articulado
no
tratamento
da
doenc¸a
de
Legg-Calvé-Perthes
por
meio
de
artrodiástase
na
fase
ativa
da
moléstia
Palavras-chave:
Doenc¸adeLegg-Calve-Perthes Procedimentosortopédicos Fixadoresexternos Articulac¸ãodoquadril
r
e
s
u
m
o
Objetivo: Apresentaros resultados preliminaresdotratamento da DLCPcomousode artrodiástasecomfixadorexternomonolateralaplicadoaoquadriledescreversucintamente atécnicaoperatóriausadaemumestudoprospectivo.
Métodos: Estudoprospectivode18pacientescomDLCPsubmetidosaotratamento oper-atóriocomatécnicadeartrodiástasedoquadrilpormeiodefixadorexternounilateral.São 13pacientesdogêneromasculinoecincodofemininocomidademédiade8,5anoscom variac¸ãodecincoa13anos.Todosospacientescomacometimentounilateraldoquadril, nove àdireitaenove àesquerda.Aavaliac¸ãodos resultadosfoi feitanamaturidade e consideroucritériosclínicoseradiográficos.
Resultados: Todosospacientesevoluíramcommelhoriadamobilidadearticularcomalívio da dor obtidoem 88,9% dos pacientes. A reossificac¸ão da epífisefemoral ocorreunos primeirostrêsmesesdotratamento.Osquadrisoperadosnafasedenecrosenãopassaram pelafasedefragmentac¸ãoeabreviaramotempodeevoluc¸ãodadoenc¸a.Osresultadosforam 77,8%satisfatóriose22,2%insatisfatórios.
Conclusões: Aartrodiástasedoquadrilcomfixadorexternomonolateralnafaseativada DLCPmelhoraograudemobilidadearticular.Oempregodatécnicadeartrodiástasenas fasesdenecroseefragmentac¸ão(faseativadadoenc¸a)apresentaresultadossatisfatórios notratamentodaDLCP.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
A childhoodhip disorder was described simultaneously in 1910byLegg(UnitedStates),Calvé(France),andPerthes (Ger-many)asanobscurealteration,pseudocoxalgia,andjuvenile deforming arthritis, which characterize the picture known todayasLegg-Calve-Perthesdisease(LCPD).1
Thediseaseisself-limiting,originatedbyischemiaofthe femoral head in varying grades, leading to bone necrosis. Theetiology isstillunknown, althoughseveralhypotheses thatattempttoexplainthedeficiencyinbloodsupplyofthe femoralheadhavebeenraised.2
TherearevariousdegreesofavascularnecrosisinLCPD, whichdependmainlyontheextentoftheinjury.Thepresence ofnewepisodesofischemia,likelytooccurduringthecourse ofthe disease,may resultinafemoralhead withdifferent stagesofself-repair.3
Initially,necrosisaffectstheepiphysealtissueandgiverise tonewlyformedbonetissue.Thehyalinecartilagebecomes relativelythickened,asitcontinuestoreceivenormal nutri-tionfromthesynovialfluidandmaintainsthesphericalshape ofthefemoralhead.4
In the second stage of the disease,there is fragmenta-tion ofthe femoralhead, followed byresorption and bone replacement, which lasts from one to three years. In this stage, there is a spread of necrotic tissue by vascularized connectivetissue;resorptionandnecrosiswhenreplacement by immaturebone tissue takes place. The epiphysis loses
height due tothe collapseof the trabecular boneand the absorptionoffragmentedbone.Inmoderateandseverecases, metaphysealchangesinthefemoralnecktakeplace.
Thethirdstageofthedisease,therepairingstage,is charac-terizedbythereplacementofnecroticandimmatureboneby maturebonetissue.Thehistopathologicalpatternobserved in this stageranges from areas without boneinfarctionto femoralheadswithseveralareasofnecroticandmaturebone. ThechildwithLCPDfeelspaininthehipand/orkneeand decreasedjointrangeofmotion,primarilyintheinternal rota-tionandhipabductionmovements.
Radiographic examination in LCPD is characterized by threesigns:firstistheshrinkingoftheossificationnucleusof thefemoralhead,withwideningofthejointspace;secondisa subchondralfracture(Caffey’ssign),which,accordingtoSalter and Thompson,3 marksthebeginningoftheclinical symp-tomsandisconsidered,dependingonitslength,aprognostic factorfordisease;thirdsignistheincreaseoftheradiopacity ofthefemoralhead,characterizingavascularnecrosis.From thatmomenton,therepairprocessproducesheterogeneous images,dependingontheareasofrevascularizationandnew necrosisoutbreaks.
Treatmentresultsare influenced bymany factors;main onesareageatonset,maintenanceofthejointmobility,and degreeofhipinvolvement.
Thelong-termfollow-upofpatientstreatedinthis hospi-tal–withabductiondevices,femoralandiliacosteotomies, or cheilectomy – has indicated a tendency toward remod-eling, with alterations in the sphericity of the femoral head.5–7
ThetreatmentofLCPDhasasitsbasicprinciplethe pro-tection of the proximal femoral epiphysis. The idea of a treatmentmethodthatallowscenteringofthefemoralhead and providesprotectionagainst mechanicalbody load and against the action of pelvitrochanteric muscles is attrac-tive.
Inthisarticle,theauthorspresentthepreliminaryresults ofLCPDtreatmentwiththeuseofunilateralexternalfixator througharthrodiastasis, aimingtocreatenegativepressure onthe femoralhead and preserving thejoint space, in an attempttodecreasetheharmfuleffectsofsubchondral frac-turesanddestructionofthetrabecularboneofthefemoral head.
Material
and
methods
Thisprospectivestudyreportstheinitialexperiencewith18 patientswithLCPDsubmittedtosurgerywiththehip arthro-diastasistechniquethroughtheuseofaunilateralexternal fixator.
ThisstudywasapprovedbytheScientificCommitteeand ResearchEthicsCommitteeofourinstitution(DocumentNo. 201/95).
Thirteenmalesandfivefemales,withameanof8.5years ofage(range:5–13years),wereincluded.
Allpatientshadunilateralhipinvolvement:nineattheleft andnineattherightside.
Patientswereclassifiedaccordingtotheradiographic crite-riadevelopedbyCatterall8andbyHerringetal.9
Results were assessed considering clinical and radio-graphiccriteria.Asclinicalcriteria,theresponseofpatients inrelationtopaincontrolinthehipjointoftheaffectedside wereassessed,aswellasjointrangeofmotionandgeneral degreeofmovementofthehip:externalandinternalrotation, abductionandadduction,flexionandextension.
RadiographicevaluationincludedtheinitialCatterall8and Herringetal.9classification,aswellastheclassificationforthe finalresultsproposedbyStulbergetal.10atskeletalmaturityof thehipregion.Thecenter-edge(CE)angleoftheacetabulum wasalsomeasured.Thesphericityofthefemoralheadwas assessedaccording totheMose11 method,andthe indexes andepiphyseal quotientwere measured.Theextentofhip subluxationwasalsoassessed.
ThesystemproposedbythePediatricOrthopaedicSociety ofNorthAmerica(POSNA),12showninTable1,wasusedfor theevaluationofpostoperativeresultsofpatients.
Inclusioncriteria
Patientsofbothgenders,withthediagnostic ofLCPD,with unilateralhip diseasepresentingrestrictionofthe affected
Table1–PediatricOrthopaedicSocietyofNorth-America (POSNA)assessmentsystem.12
Result Center-edgeangle Mosecircles
Good >20◦ 0
Fair 15–19◦ 2
Poor <15◦ >2
joint movements, and pain duringactivities ofdailyliving wereincluded. TypesIIIorIVintheCatterall8classification
andwithtwoormore“radiographicrisksigns”;typesBorCin theclassificationbyHerringetal.9;patientsintheearlystages ofradiographiccondition,i.e.,condensationorfragmentation, which characterizes the “active” stage ofthe disease were included.
Exclusioncriteria
Patients with bilateral involvementof the hips and whose radiographicexaminationpresentedinitialsubluxationabove 50%ofthefemoralheadcircumferencemeasuredbythe Dick-ensandMenelaus13method,aswellaspatientsinthestage offemoralheadremodelingaccordingtoradiographic analy-sis.
Statisticalanalysis
Descriptive statistics of quantitativeordinal parameters of age,timeofusageoftheexternalfixator,follow-uptime,and rangeofmotion(externalandinternalrotation,abductionand adduction,flexionandextension)werecalculated:mean(M), standard deviation(SD), standarderror ofthe mean (SEM), maximum(Max)andminimumvalues(Min),andthenumber of cases (N). In the comparison of two groups of depend-ent paired ordinal parameters, the paired t-test was used, in caseofparametric distributions, and the Wilcoxon test, incaseofnon-parametric distributions.Mann–Whitney’sU testwasusedforindependentnon-parametricsamples. Abso-lute and relative frequencydistribution (%) was calculated to describe normaldistributions (qualitative).Comparisons betweennominaldistributionsweremadeusingFisher’sexact test.
Thesignificancelevelof5%(˛=0.05)wasadopted. Signifi-cantresults(differences)werehighlightedbyasterisks.
Surgicaltechnique
Indications for surgical treatment with hip arthrodiastasis throughexternalfixationinLCPDwereasfollows:
1) Pain,eveninthelowestdegree;
2) Decreaseinthedegreeofmobilityoftheaffectedjoint; 3) CatterallgroupsIIIorIV;
4) Atleasttworadiographicsignsof“headatrisk”; 5) Lessthan50%subluxationofthefemoralhead.
Fig.1–Illustrationofthepositionoftheexternalfixator. TwotothreeSchanzscrewsposteriorlyandinferiorly. (Impolfix®,Impol,SãoPaulo,Brazil).
Source:DepartmentofOrthopedicsandTraumatology,
FMUSP.
Aunilateral,articulatedexternalfixator(Impolfix®,Impol,São Paulo,Brazil)wasused.Theexternalfixatorisappliedwitha coupleofSchanzscrewspositionedintheacetabularregion andanothercoupleofSchanzscrewsinthediaphysealzone ofthefemur.
Jointdiastasisisappliedduringsurgeryaimingtocorrect Shenton’slineunderfluoroscopiccontrol.
Figs.1–4illustratethemainstepsforpositioningthe uni-lateralexternalfixator.
Fig.2–Illustrationofthepositionoftheexternalfixator fromtherotationcenterofthefemoralhead(arrow). (Impolfix®,Impol,SãoPaulo,Brazil).
Source:DepartmentofOrthopedicsandTraumatology,
FMUSP.
Fig.3–Illustrationofthepositionoftheexternalfixator (Impolfix®,Impol,SãoPaulo,Brazil)andhow
arthrodiastasisisperformed.
Source:DepartmentofOrthopedicsandTraumatology,
FMUSP.
Postoperative
Ifhipdiastasisisnotachievedthroughsurgery,itcanbeslowly progressedduringpostoperativeperiodof10–15days.Weekly dressings are usedinthe areasofcutaneousemergenceof theSchanzscrews.ControlX-raysareperformedatfour-week intervals.Theexternalfixatorremainsinsertedfor approxi-matelythreemonths.
Results
Clinicalanalysis
Theassessmentofage,sex(maleandfemale),andtheaffected side(rightorleft)ofthepatientsisshowninTable2.Table3
presents thepre- andpostoperativeclinical analysisofthe degreeofhipamplitude.
Radiographicanalysis
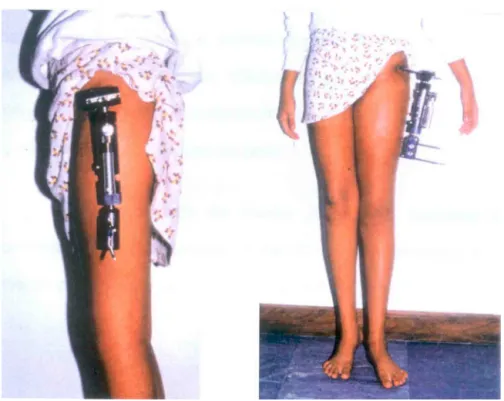
Fig.4–Photographoftheidealpositioningofmonolateralexternalfixator(Impolfix®,Impol,SãoPaulo,Brazil). Source:DepartmentofOrthopedicsandTraumatology,FMUSP.
Tables5–7 present the studies comparingthe outcomes aftersurgeryforPOSNAcriteriaandthefollowingfactors:sex, age,andfinalresult.
Figs.5–8showtheevolutionofapatientoperatedat7years and4monthsandtheprogresstwoyearsaftersurgery.
Table2–Presentationofpatientsaccordingtoage (years),sex,andaffectedside.
Order Age(years) Sex Side
1 8 M R
2 12 M L
3 9 M L
4 9 F L
5 9 M L
6 13 M R
7 6 F R
8 9 M R
9 8 M L
10 10 M L
11 7 M R
12 8 M L
13 9 M L
14 10 M R
15 7 F R
16 9 F R
17 5 F R
18 5 M L
M,males(13);F,females(5);R,right(9);L,left(9). Age–meanof8.5years;<7years=16.7%;>7years=83.3%.
Discussion
LCPDisaself-limitingconditioncausedbyischemiaand vary-ingdegreesoffemoralheadnecrosis.Thecauseofischemia iscurrentlyunknown;many hypothesesaresuggested,but thereisstillnocompleteproof.Currently,themostaccepted theoriesaredelayinskeletaldevelopment,microtrauma,and vascularalterations.14
According toBensahel,15 the highestfrequencyofLCPD isobservedintherangeof4–8years;itisanrarediagnosis outsidetheagerangeof2–10years.Inthepresentstudy,the meanageatdiseaseonsetwas8.5years,rangingfrom5to 13.Thisgroupofpatientscanbeconsideredapoorprognostic riskgroup,asageatdiseaseonsetisoneofthefactorsthat mostinfluenceoutcomes.16–18
ThepresentstudyincludedpatientsclassifiedasCatterall typesIIIandIV,whicharethetwogroupswithworst prog-nosis. Furthermore, patients had atleast two radiographic signsof“headatrisk.”Consideringthelimitationof(mean) movementamplitudeoftheaffectedhip,theneedfor surgi-caltreatmentindicationforthegroupofpatientsstudiedwas proven.
InthesurgicaltreatmentofLCPD,varizationosteotomies of the femur or the iliac bone (acetabulum) are the sur-gical treatment modalities most used to achieve femoral head containment. The literature review retrieved studies thatshowednosignificantdifferencebetweenbothtypesof osteotomy.19,20
Table3–Degreeofrangeofmotionofthehip,pre-andpostoperative,withstatisticalanalysis.
Amplitude(◦) Preoperative Postoperative Comparison
Abduction 20.6±11.49(2.71) 40.3±9.1(2.1) WilcoxonTc=34
To=0
Adduction 16.9±5.18(1.22) 20.8±4.62(1.09) WilcoxonTc=2
To=0
Flexion 92.2±0.17(0.04) 115.5±11.99(2.83) tPAIRED
t=4.73p=0.0002 Extension 16.4±2.87(0.68) 19.2±2.57(0.61) tPAIRED
t=4.61p=0.0002 Externalrotation 16.9±11.65(2.75) 37.5±11.41(2.69) WilcoxonTc=40
To=1
Internalrotation 9.3±9.54(2.25) 25.6±12.23(2.88) WilcoxonTc=29
To=1
Tc,criticalT;To,Tobtained.
Fig.5–Malepatient,7yearsand4months,CatterallIII.Preoperativeimage.
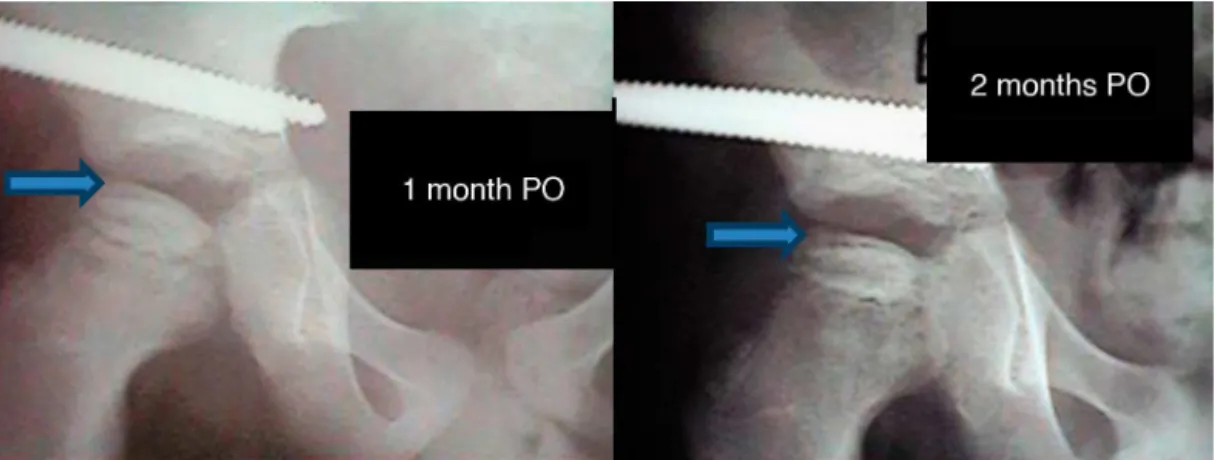
Fig.6–PatientfromFig.1,atoneandtwomonthspostoperatively.Newlygrowingtissue(arrow).
Table4–LCPDstagingandfrequencydistributionofthe resultsaccordingtotheCatterallandHerring
classifications.
Classification Catterall Herring
III–7(38.9%) A–1(5.6%) IV–11(61.1%) B–12(66.7%)
C–5(27.8%)
Total 18(100%) 18(100%)
by Volkov and Oganesian.21 The use ofanexternal fixator to promotethe maintenanceofthe joint space,utilized in variousjoints suchasknee,elbow,hip,andankle, hasalso been described for various orthopedic conditions, such as traumaandsequelae,septicarthritis,tuberculosis, epiphys-iolysis,chondrolysis,andLCDP.21–25AccordingtovanValburg etal.,26themaintenanceofthejointspaceprovidedbythe externalfixator,evenafterashortperiodoftreatment, indi-cates some joint repair, an important factor for obtaining clinicalimprovementofthepatient.
Table5–Frequencydistributionofthepostoperative resultsinthePOSNAclassificationofaccordingtosex. ComparisonbyFisher’sexacttest(˛=0.05).
POSNA
Sex Satisfactory Unsatisfactory Total
Male 11(61.1%) 2(11.1%) 13(72.2%) Female 3(17.7%) 2(11.2%) 5(27.8%)
Total 14(77.8%) 4(22.2%) 18(100%)
Fisherp=0.30.
Table6–Frequencydistributionofthepostoperative resultsinthePOSNAclassificationofaccordingtoage range.ComparisonbyFisher’sexacttest(˛=0.05).
POSNA
Agerange(years) Satisfactory Unsatisfactory Total
<7 2(11.1%) 1(5.5%) 3(16.7%) ≥7 12(66.7%) 3(16.7%) 15(83.3%)
Total 18(100%) 4(22.2%) 18(100%)
Fisherp=0.30.
Table7–Frequencydistributionofthepostoperative resultsinthePOSNAclassification.
POSNArating Absolute Relative(%)
Satisfactory 14 77.8
Unsatisfactory 4 22.2
Total 18 100.0
treatment.Theischemic femoralheadissubjectedto pres-sure overloadevenwhenthe patient isatrest,due tothe actionofthe muscles.Theideaofachievingneutralization ofthemusclestrengthandoftheweightforceactingonthe
Fig.7–PatientfromFig.1,atthreemonthspostoperatively. Reossificationofthefemoralhead.
femoralhead,whichincreasesthejointspace,creatinga situa-tioninwhichthearticularcartilagecanregenerateafterinjury, is veryattractive. Adding movement tothe methodallows foranimprovementinsynovialfluidcirculationand conse-quentimprovementofarticularcartilagenutrition,givingthe methodveryusefulmechanicalandbiologicalcharacteristics forthetreatmentofLCPD.Moreover,thistechniquepreserves thearticularsurfaceandprotectstheepiphysisfromforces actingonthehip;italsoreducestheriskofflatteningofthe headandcollapseofthenewlyformedvessels.Accordingto Stulberg,10decreasedjointspaceisthefactorthatshowsthe greatestassociationwithclinicallong-termresultsinLCPD.
DuringthenaturalcourseofLCPD,thehipundergoesthe phasesofsynovitis,necrosis,andremodeling4; arthrodiasta-siswasusedonhipsinthenecrosisorfragmentationstages (“active” stages of the disease). Afast revascularization of thefemoralepiphysiswasobservedinanintervalofoneto threemonths(Figs.5–8).Whenhipsweretreatedinthe necro-sis stage,regenerationoccurred without the fragmentation
phase.Thisphenomenonisconsistentwiththatdescribedby Volponetal.27
AllmodalitiesoftreatmentforLCPDarebasedin mechan-ical concepts. Arthrodiastasis offers a biological concept beyondthemechanicalconceptofanatomicaljoint centraliza-tionandmechanicalloadprotectionimposedonthejoint.28–30 AccordingtotheconceptsofIlizarov,31arthrodiastasisinduces angiogenesisaroundtheentirejoint.Itisimportanttonote that,undertheinfluenceofmechanicaltraction-loadoffered byarthrodiastasis,activehistogenesisoccursnotonlyinthe bone,butalsointheregionalsofttissues;yet,accordingto Ilizarov,theprocessoftissueformationandgrowthinanadult organismhasmanyfeaturesincommonwithtissue forma-tionduringtheembryonicandimmediatepostnatalperiods.
Figs.6and7presentanexampleofthistypeoftissue forma-tion.
The preliminary satisfactory results of treatment with arthrodiastasisobtainedin77.8%ofpatientscanbe consid-eredasoverall“good,”thusaccreditingthetechniqueasan effectiveLCPDtreatmentmethod.
TheauthorsagreewithKucukkayaetal.32 that arthrodi-astasisisagoodoperativetreatmenttechniqueforpatients agedabove6yearsandconsideredashavingpoorprognosis inthecriteriasetforthbyCatterall.Moreover,theprocessof reossification/remodelingofthefemoralheadappearstobe shortenedbyarthrodiastasisoftheaffectedhip.
Conclusion
Hip arthrodiastasis with unilateral external fixator in the activestagesofLCPDimprovesthedegreeofjointmobility.
Theuseofthearthrodiastasistechniqueinthenecrosisand fragmentationstages(activestagesofthedisease)presents satisfactoryresultsinthetreatmentofLCPD.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. WengerDR,WardTW,HerringJA.Currentconceptsreviewin Legg-Calvé-Perthesdisease.JBoneJointSurgAm.
1991;73(5):778–88.
2. KimHKW.Legg-Calvé-Perthesdisease.JAmAcadOrthop Surg.2010;18(11):676–86.
3. SalterRB,ThompsonGH.Legg-Calvé-Perthesdisease.The prognosticsignificanceofthesubchondralfractureanda two-groupclassificationofthefemoralheadinvolvement.J BoneJointSurgAm.1984;66(4):479–89.
4. JonsäterS.Coxaplana.Ahisto-pathologicandarthrographic study.ActaOrthopScandSuppl.1953;12:5–98.
5. CordeiroEN.FemoralosteotomyinLegg-Calvé-Perthes disease.ClinOrthopRelatRes.1980;(150):69–72.
6. GuarnieroR,IshikawaMT,LuzoCAM,MonetenegroNB, GodoyJúniorRM.Resultadosdaosteotomiafemoralvarizante notratamentodadoenc¸adeLegg-Calvé-Perthes.RevHosp ClinFacMedSaoPaulo.1997;52(3):132–5.
7.GuarnieroR,LuzoCAM,GrigolettoWJr,LageLAA,Iacovone M.Cheilectomyasasalvagesurgeryinthediseasedhip:early results.MAPFREMed.1995;6:208–10.
8.CatterallA.ThenaturalhistoryofPerthes’disease.JBone JointSurgBr.1971;53(1):37–53.
9.HerringJA,NeustatdtJB,WilliansJJ,BrowneRH.Thelateral pillarclassificationofLegg-Calvé-Perthesdisease.JPediatr Orthop.1992;12(2):143–50.
10.StulbergSD,CoopermanDR,WallensteinR.Thenatural historyofLegg-Calvé-Perthesdisease.JBoneJointSurgAm. 1991;63(7):1095–108.
11.MoseK.MethodsofmeasuringinLegg-Calvé-Perthesdisease. ClinOrthopRelatRes.1980;(150):103–9.
12.MeehanPL,AngelD,NelsonJM.TheScottishRiteabduction orthosisforthetreatmentofLegg-Perthesdisease.A radiographicanalysis.JBoneJointSurgAm.1992;79(1): 2–12.
13.DickensDRV,MenelausMB.Theassessmentoftheprognosis inPerthes’disease.JBoneJointSurgBr.1978;60(2):189–94.
14.DimeglioA.Legg-Calvé-Perthesdisease:etiology.MAPFRE Med.1995;6:10–1.
15.BensahelH.EpidemiologyofLCPdisease.MAPFREMed. 1995;6:8–9.
16.HerringJA.ThetreatmentofLegg-Calvé-Perthesdisease:a reviewoftheliterature.JBoneJointSurgAm.
1994;76(3):448–57.
17.PoussaM,YrjonenT,HoikkaV,OstermamK.Prognosisafter conservativeandoperativetreatmentinPerthes’disease.Clin OrthopRelatRes.1993;(297):82–6.
18.HoikkaV,PoussaM,YrjonenT,OstermamK.
IntertrochantericvarusosteotomyforPerthes’disease. Radiographicchangesafter2–16yearfollow-upof126hips. ActaOrthopScand.1991;62(6):549–53.
19.MobergA,HanssonG,KaniklidesC.Resultsafterfemoraland innominateosteotomyinLegg-Calvé-Perthesdisease.Clin OrthopRelatRes.1997;(334):257–64.
20.SponsellerPD,DesaiSS,MillisMB.Comparisonoffemoral andinnominateosteotomiesforthetreatmentof Legg-Calvé-Perthesdisease.JBoneJointSurgAm. 1988;70(8):1131–9.
21.VolkovMV,OganesianOV.Restorationoffunctionintheknee andelbowwithahinge-distractorapparatus.JBoneJoint SurgAm.1975;57(5):591–600.
22.KruminsM,KalnisJ,LacisG.Reconstructionoftheproximal endofthefemurafterhematogenousosteomyelitis.JPediatr Orthop.1993;13(1):63–7.
23.CanadellJ,GonzalesF,BarriosRH,CamilloS.Arthrodiastasis forstiffhipsinyoungpatients.IntOrthop.1993;17(4):254–8.
24.JudetR,JudetT.Arthrolyseetarthroplastiesousdistracteur articulaire.RevChirOrthopReparatriceApparMot. 1978;64(5):353–65.
25.CobbTK,MorreyBF.Useofdistractionarthroplastyin unstablefracturedislocationsoftheelbow.ClinOrthopRelat Res.1995;(312):201–10.
26.vanValburgAA,vanRoermundPM,LammensJ,van MelkebeekJ,VerboutAJ,LafeberEP,etal.CanIlizarovjoint distractiondelaytheneedforarthrodesisoftheankle?JBone JointSurgBr.1995;77(5):720–5.
27.VolponJB,LimaRS,ShimanoAC.Tratamentodaformaativa dadoenc¸adeLegg-Calvé-Perthespelaartodiástase.RevBras Ortop.1998;33(1):8–14.
28.KocaogluM,KilicogluOI,GoksanSB,CakmakM.Ilizarov fixatorfortreatmentofLegg-Calvé-Perthesdisease.JPediatr OrthopB.1999;8(4):276–81.
30.PaleyD.Tratamentodenecrosedacabec¸adofemurcom artrodiástasedoquadril.In:VCongressodeOrtopediae TraumatologiadoEstadodeSãoPaulo.1993.
31.IlizarovGA.Thetension-stresseffectonthegenesisand growthoftissues.In:IlizarovGA,editor.Transosseous osteosynthesis.Berlin:Springer-Verlag;1992.p.137–255.