w w w . r b o . o r g . b r
Original
Article
Bilateral
developmental
dysplasia
of
the
hip
treated
with
open
reduction
and
Salter
osteotomy:
analysis
on
the
radiographic
results
夽
,
夽夽
Anastácio
Kotzias
Neto
∗,
Adriana
Ferraz,
Franco
Bayer
Foresti,
Rafael
Barreiros
Hoffmann
HospitalInfantilJoanadeGusmão,Florianópolis,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received10March2013 Accepted10October2013 Availableonline5April2014
Keywords: Hipdislocation, congenital/pathology
Hipdislocation,congenital/etiology Hipdislocation,congenital/surgery Hipdislocation,congenital/therapy
a
b
s
t
r
a
c
t
Objectives:toevaluatetheradiographicresultsfrompatientswithbilateraldevelopmental dysplasiaofthehip(DDH)whounderwentsurgicaltreatmentbymeansofopen reduc-tionandSalterosteotomy,withorwithoutassociatedfemoralshorteningasdescribedby Ombrédanne.
Methods:thiswasaretrospectivedescriptivestudyinwhich21patientswithbilateralDDH (42hips)wereanalyzed.TheyweretreatedatHospitalInfantilJoanadeGusmão(HIJG),with operationsbetweenAugust1997andOctober2009.Toevaluatetheradiographicresults, theacetabularindexandtheWibergcenter-edgeangleweremeasured,andtheSeverin andKalamchi–MacEwenclassificationswereused.Descriptiveandparametricstatistical analyseswereusedtoevaluatethedata.
Results:wedidnotobserveanystatisticallysignificantdifferenceinanalyzingthe radio-graphicparameters, makingcomparisonsregarding the side affected,the order ofthe proceduresandwhetherfemoralshorteningwasperformed,althoughtherewasa signifi-cantdifferencebetweenthemfrombeforetoaftertheoperation.
Conclusion:openreductioninassociationwithiliacosteotomyasdescribedbySalter pre-sented significant improvements in the radiographic parameters analyzed, comparing thepre-andpostoperativevalues.Thisimprovementoccurredindependentlyofwhether Ombrédannefemoralshorteningwasperformed.Themostprevalentcomplicationinthe studygroupwasavascularnecrosisofthefemoralhead.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Displasia
do
desenvolvimento
do
quadril
bilateral
tratada
com
reduc¸ão
cruenta
e
osteotomia
de
Salter:
análise
dos
resultados
radiográficos
Palavras-chave: Luxac¸ãocongênitade quadril/patologia
r
e
s
u
m
o
Objetivos:avaliarosresultadosradiográficosdepacientesportadoresdedisplasiado desen-volvimentodoquadril(DDQ)bilateral, submetidosaotratamentocirúrgicopormeioda
夽
Pleasecitethisarticleas:KotziasNetoA,FerrazA,BayerForestiF,BarreirosHoffmannR.Displasiadodesenvolvimentodoquadril bilateraltratadacomreduc¸ãocruentaeosteotomiadeSalter:análisedosresultadosradiográficos.RevBrasOrtop.2014;49:350–358. 夽夽
WorkperformedattheOrthopedicsandTraumatologyService,HospitalInfantilJoanadeGusmão,Florianópolis,SC,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.KotziasNeto).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
rev bras ortop.2014;49(4):350–358
351
Luxac¸ãocongênitade quadril/etiologia Luxac¸ãocongênitade quadril/cirurgia Luxac¸ãocongênitade quadril/terapia
reduc¸ãocruentaeosteotomiadeSalterassociadaounãoaoencurtamentofemoraldescrito
porOmbrédanne.
Métodos: trata-sedeestudodescritivoretrospectivocomanálisede21pacientescomDDQ bilateral(42quadris),tratadosnoHospitalInfantilJoanadeGusmão(HIJG)eoperadosentre agostode1997eoutubrode2009.Paraavaliac¸ãodosresultadosradiográficos,forammedidos oíndiceacetabulareoângulocenter-edge(CÊ)deWibergeusadasasclassificac¸õesdeSeverin edeKalamchieMacEwen.Análisesestatísticasdescritivaseparamétricasforamusadas paraavaliac¸ãodosdados.
Resultados:nãoobservamosdiferenc¸aestatisticamentesignificantenaanálisedos parâmet-rosradiográficoscomparando-osquantoaoladoacometido,àordemdosprocedimentose àfeituradeencurtamentofemoralounão,emboraexistadiferenc¸asignificativaentreeles nosperíodospréepós-operatório.
Conclusão: reduc¸ãocruentaassociadaàosteotomiadoilíacodescritaporSalterapresentou melhoriasignificativadosparâmetrosradiográficosanalisadosnacomparac¸ãodosvalores prée pós-operatórios.Essamelhoriaocorreuindependentementeda feituraounãodo encurtamentofemoraldeOmbrédanne.Acomplicac¸ãomaisprevalentenogrupoestudado foianecroseavasculardacabec¸afemoral.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Developmental dysplasia of the hip (DDH) comprises a
spectrumof abnormalities during the development ofthis
joint that vary according to the patient’s age and go from self-limitingdefectswithoutlong-termconsequencesto dis-locationthatmayleadtopermanentdeficiency.1Incasesin
whichdislocationofthehipoccurs,theacetabulumpresents adeficiencyinitsanterosuperioraspectandisshowntobe thick,shallowandoblique.2Theetiologyismultifactorial,with
genetic,hormonalandenvironmentalcauses,butitisbelieved thattheprimarycauseisrestrictionofthemovementsofthe fetusorhyperelasticityofthejointcapsuleofthehip.3
TheincidenceofDDHwithdislocationisaroundonein
every thousandlivebirths.Itismoreprevalent inchildren withpelvicpresentation,femalesandchildrenwithapositive familyhistory(12%to33%).3–6
TheprognosisforDDHisdirectlylinkedtoearly diagno-sis,whichenablestreatmentthatismoreeffectiveandless aggressivetowardthepatient.7However,aconsiderable
num-ber ofcases are diagnosed after the child starts towalk.8
Thetreatment hasthe aim ofrecovering joint congruence
andstability,soastopromoteitsphysiologicaldevelopment. When instituted within the first days of life, a high
suc-cess rate and reduced complication rate are achieved. As
thechildgrows,the anatomicalalterationsincrease,which makesthe treatmentmoredifficult.9,10 Insmallerchildren,
the treatmentbegins withclosed reductionbymeans of a
Pavlikharness,whichiseffectiveinupto95%ofthecases.3
Afterthe age of sixmonths, the harnessloses its efficacy
andtherecommendedtreatmentbecomesclosedreduction
with plaster-cast immobilization. In children over the age
of18 months, the treatment varies from closed reduction
withplaster-castimmobilizationtoopenreductionin
asso-ciation with osteotomy. Thetreatment described bySalter
isthe preferred procedure and itmay or may notbeused
in association with the femoral shortening described by
Ombrédanne.3,11–13
Theimportanceofearlyidentificationandadequate
treat-ment for this disease is to prevent its sequelae, such as
deformity ofthe femoralhead, anteversion ofthe femoral
neck,valgusthighanddysplasticacetabulum,whichevolve tohiparthrosis.14,15
Theobjectiveofthisstudywastoevaluatetheradiographic resultsfrompatientswhounderwentsurgicaltreatmentfor
bilateral dislocation, with open reduction combined with
Salter’sosteotomy,inassociationwithOmbrédanne’sfemoral
shorteningwhennecessary.
Material
and
methods
Thiswasaretrospectivedescriptivestudy.Themedicalfiles ofallthepatientswithDDHattendedattheJoanadeGusmão Children’sHospital(HIJG)betweenAugust1997andOctober 2009werereviewed.Treatmentwasprovidedfor296patients: 70 (23.65%) using Pavlik’s harness, 93 (31.42%) with closed
reduction that was maintained using a plaster case from
thepelvistothefoot,21(7.09%)withopenreductionalone
and 112 (37.84%) with open reduction in association with
osteotomy.Amongtheosteotomycases,11patients(9.82%)
underwenttheDegaprocedure,four(3.57%)Pemberton,two
(1.79%)Chiari,two(1.79%)Steel,one(0.89%)Kalamchiandone (0.89%)Shelf.Amongtheremaining91patients(81.25%),the Salterprocedurewasused.Inthepresentstudy,onlythecases withbilateralinvolvementtreatedbymeansofopen
reduc-tion andSalter’sosteotomy,withorwithout Ombrédanne’s
femoralshortening,wereanalyzed.
Weanalyzed21patientswithbilateralDDH(42hips oper-ated).Ofthese,19(90.5%)were femaleandtwo(9.5%)were male.Themeanageatthetimeofdiagnosiswas2.3years; theearliestwasattheageofonemonthandthelatestwasat 4.6years.Themeanlengthoffollow-upwas5.8years,witha rangefromtwoyearsto13yearsandninemonths.
Thelengthofpostoperativeimmobilizationwassixweeks.
The patients were treated by two surgeons. In two cases
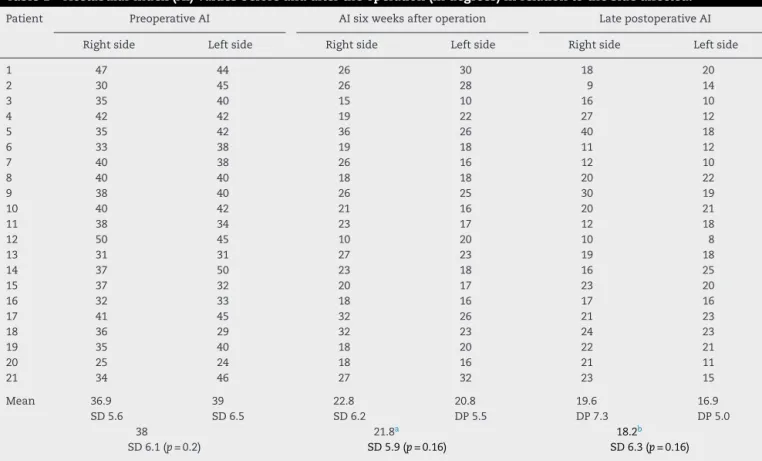
Table1–Acetabularindex(AI)valuesbeforeandaftertheoperation(indegrees)inrelationtothesideaffected.
Patient PreoperativeAI AIsixweeksafteroperation LatepostoperativeAI
Rightside Leftside Rightside Leftside Rightside Leftside
1 47 44 26 30 18 20
2 30 45 26 28 9 14
3 35 40 15 10 16 10
4 42 42 19 22 27 12
5 35 42 36 26 40 18
6 33 38 19 18 11 12
7 40 38 26 16 12 10
8 40 40 18 18 20 22
9 38 40 26 25 30 19
10 40 42 21 16 20 21
11 38 34 23 17 12 18
12 50 45 10 20 10 8
13 31 31 27 23 19 18
14 37 50 23 18 16 25
15 37 32 20 17 23 20
16 32 33 18 16 17 16
17 41 45 32 26 21 23
18 36 29 32 23 24 23
19 35 40 18 20 22 21
20 25 24 18 16 21 11
21 34 46 27 32 23 15
Mean 36.9
SD5.6
39
SD6.5
22.8
SD6.2
20.8
DP5.5
19.6
DP7.3
16.9
DP5.0
38
SD6.1(p=0.2)
21.8a
SD5.9(p=0.16)
18.2b
SD6.3(p=0.16)
AI,acetabularindex;SD,standarddeviation.
a SignificantdifferencebetweenpreoperativeAIandAIofsixweeksafteroperation(p<0.000001).
b SignificantdifferencebetweenpreoperativeAIandlatepostoperativeAI(p=0.001).
reduction. The other patients (90.5%) had not previously
undergoneanytypeoftreatment.
In one patient, the osteosynthesis material was not
removedbecauseoftechnicaldifficulties.Inalltheothers,the materialwasremoved.Themeanlengthoftimeafterthe oper-ationforthisproceduretobeperformedwas21.5monthsfor theleftsideand22.45monthsfortherightside.
Toevaluatetheradiographicresults,weusedthe acetab-ular index(AI),the center-edge angle(CÊ)ofWiberg,16 the
classificationofSeverin17andthetypeofavascularnecrosis
ofthefemoralhead,accordingtotheclassificationof Kalam-chiandMacEwen.18Thestatisticalanalysiswasperformedin
descriptiveandanalyticalformbymeansofthechi-square, pairedWilcoxon,Student’standpairedStudent’stmethods, withtheaimofestablishingwhetherstatisticalsignificance existedbetweentheparametersevaluated.Weusedthe Ses-tatnetsoftware19toanalyzethedataandthesignificancelevel
wasfoundtobe0.05.
ThisstudywasapprovedbytheResearchEthicsCommittee (CEP-HIJG)andwasregisteredunderprotocol027/2011.
Results
ThemeanpreoperativeAIwas38◦(±6.1◦):therightside pre-sentedamean of36.9◦ (±5.6◦)andtheleft side,39◦(±6.5◦). Therewasnostatisticaldifferenceinrelationtothisfinding, whichindicatedthatthesamplewashomogenous(Table1).
ThemeanAIsixweeksaftertheoperationwas21.8◦(±5.9◦)
amongthe 42 hips.The mean forthe rightside was 22.8◦
(±6.2◦)andfortheleftside,20.8◦ (±5.5◦).Therewasno sig-nificant difference(Table1). Thegeneralmeanforthe late postoperative AI was 18.2◦ (±6.3◦): for the right side, 19.6◦ (±7.3◦)andfortheleftside,16.9◦ (±5.0◦).Therewasno sta-tistically significant difference, but there was a significant differenceincomparingthepreoperativeAIwiththeAIsix weekaftertheoperationandwiththelatepostoperativeAI (Table1).
Thedegreeoffemoralheadnecrosiswasevaluated.There was nonecrosisin eightpatients,whiletwo were affected bilaterallyandelevenpresentedunilateralnecrosis.Outofthe 42hipsoperated,27didnotpresentnecrosis(64.29%),type1 necrosisoccurredinthreepatients(7.4%),type2infive(11.9%), type3infour(9.52%)andtype4inthree(7.14%).Inrelationto thesideaffected,wedidnotfindanystatisticallysignificant difference(Table2)(Figs.1A–Cand2A–C).
InrelationtotheCÊofWiberg,16themeanpostoperative
valuewas19.4◦(±11.6◦):fortherightside,18.1◦(±11.7◦),and fortheleftside,19.7◦(±12.3◦).Therewasnosignificant differ-encebetweenthesides(Table2).
Outofthetotalnumberofhips,accordingtothe classifi-cationofSeverin17(Table2),28(66.67%)presentedgoodand
rev bras ortop.2014;49(4):350–358
353
Table2–Evaluationofpostoperativeparameters,withcomparisonbetweenthesides.
Patient KalamchiandMacEwenclassification18
foravascularnecrosisofthefemoralhead
Center-edgeangle(CÊ)of
Wiberg16(indegrees)
Severinclassification17
Rightsidea Leftsidea Rightside Leftside Rightsideb Leftsideb
1 – – 18 22 1B 1A
2 – – 37 28 1A 1A
3 – 2 17 12 1B 3
4 1 – 20 18 1B 2A
5 3 – <0 11 4B 3
6 – – 31 40 1A 1A
7 2 – 34 40 1A 2A
8 2 – 13 8 3 3
9 2 – <0 16 4B 3
10 – – 15 24 2B 1A
11 – 4 32 40 1A 2A
12 4 2 35 17 2B 2B
13 – – 19 19 1A 1A
14 – – 15 16 2B 1B
15 – 3 10 0 3 4A
16 – – 10 30 3 1A
17 3 3 19 10 1A 3
18 – 1 18 8 1B 3
19 – 4 33 <0 2A 5
20 – – 16 30 1B 1A
21 1 – 8 24 3 1A
Mean 18.1
SD11.7
19.7
SD12.3
19.4
SD11.6(p=0.41)
SD,standarddeviation.
a Non-significantdifferencebetweenthesidesaffected(p=0.18).
b Non-significantdifferencebetweenthesidesaffected(p=0.08).
Thehipsdealtwithinthefirstsurgicalprocedurepresented resultssimilartothosedealtwithinthesecondprocedure, sincetherewasnostatisticaldifferenceinrelationtotheAI sixweeksafterthe operation,latepostoperativeAI,Wiberg CÊ(p=0.28),degreeofavascularnecrosisofthefemoralhead andSeverinclassification(p=0.09).Thepatients’ meanage atthetimeofthefirstsurgicalprocedurewas3.7years(1.9 to6.8years)and atthe timeofthe second surgical proce-dure,4.3years(2.5toeightyears),withameanintervalof7.2 months(3to15months)betweentheinterventions(Table3 andFig.3A–C).
Anothercriterionanalyzedwasinrelationtothepatients
who required femoral shortening. The femoral osteotomy
describedbyOmbrédanne12wasperformedon13patients(24
hips;57.14%).Therewasnostatisticallysignificantdifference inanyofthecriteriaanalyzed:AIsixweeksaftertheoperation (p=0.25),latepostoperativeAI(p=0.06),avascularnecrosisof thefemoralhead(p=0.08),Wiberg CÊ(p=0.18)and Severin classification(p=0.39).
Surgicalrevisionwasnecessaryforfourhips(9.52%)and thepatientsdidnotpresentpostoperativeinfection.
Discussion
Thetreatment forDDH hasthe basic premise ofattaining
stable concentric reduction of the hip into the functional
weight-bearingposition.Instabilityofthereductionoriginates frompoorpositioningoftheacetabulumintheanteriorand lateraldirections.OpenreductioninassociationwithSalter’s osteotomyoftheiliacboneinordertoredirecttheacetabulum istodayaclassicaltreatmentmethod.20
Intheliterature,wefoundfewstudiesshowingresultsfrom patientswhoweretreatedforbilateralDDHatalatestage,who underwentsurgicaltreatmentbymeansofopenreductionand Salter’sosteotomy,withorwithoutassociatedfemoral
short-eningasdescribedbyOmbrédanne.
Manyauthorshaverecommendedthatopenreductionin
associationwithosteotomyoftheinnominatebonefor correc-tionofacetabulardysplasiashouldbeperformedonchildren
ata minimumage of18 months21 and thatthe technique
describedbySalter22shouldbeappliedtopatientsata
max-imum age of six years.Several studies have clinically and radiographicallyevaluatedthepre-andpostoperative
condi-tions ofchildrenwithDDH whounderwentopenreduction
and Salter’s osteotomy,2,11,20,21,23–34 but noneofthem used
samplesconsistingonlyofpatientsaffectedbilaterally. Inthepresentstudy,21patientswithbilateralDDHwith
ameanintervalof7.2monthsbetweentheprocedureswere
evaluated.Thevariationinthetimebetweentheprocedures wasduetotherecoveryofmobilityinthehipthatwas oper-atedfirst.
Prado et al.21 studied 32 patients(42 hips,i.e., 10
r
e
v
b
r
a
s
o
r
t
o
p
.
2
0
1
4;
4
9(4)
:350–358
Table3–Evaluationofpostoperativeparametersinrelationtothesideaffectedearlierandlateron.
Patient Age(inmonths) AIsixweeks
afteroperation
(indegrees)
Late
postoperativeAI
(indegrees)
KalamchiandMacEwen
classification18for
avascularnecrosisofthe
femoralheada
Center-edge
angle(CÊ)of
Wiberg16(in
degrees)
Severin
classification17 b
1stS 2ndS 1stS 2ndS 1stS 2ndS 1stS 2ndS 1stS 2ndS 1stS 2ndS
1 42 46 26 30 18 20 – – 18 22 1B 1A
2 27 33 26 28 9 14 – – 37 28 1A 1A
3 59 65 15 10 16 10 – 2 17 12 1B 3
4 31 35 22 19 12 27 – 1 18 20 2 1B
5 82 86 36 26 40 18 3 – <0 11 4B 3
6 23 30 18 19 12 11 – – 40 31 1A 1A
7 31 39 26 16 12 10 2 – 34 40 1A 2A
8 28 38 18 18 20 22 2 – 13 8 3 3
9 43 46 26 25 30 19 2 – <0 16 4B 3
10 45 52 21 16 20 21 – – 15 24 2B 1A
11 40 44 23 17 12 18 – 4 32 40 1A 2A
12 81 96 20 10 8 10 2 4 17 35 2B 2B
13 35 40 27 23 19 18 – – 19 19 1A 1A
14 48 54 23 18 16 25 – – 15 16 2B 1B
15 57 64 17 20 20 23 3 – 0 10 4A 3
16 35 42 16 18 16 17 – – 30 10 1A 3
17 23 33 32 26 21 23 3 3 19 10 1A 3
18 60 71 32 23 24 23 – 1 18 8 1B 3
19 66 79 18 20 22 21 – 4 33 <0 2A 5
20 35 41 18 16 21 11 – – 16 30 1B 1A
21 35 43 27 32 23 15 1 – 8 24 3 1A
Mean 44.1
SD17.4
51.3
SD18.6
23.2
SD5.7
20.4
SD5.9
18.6
SD7.3
17.9
SD5.3
21.2
DP10.7
20.7
DP10.8
47.7
SD18.2
21.8
SD5.9(p=0.1)
18.2
SD6.3(p=0.39)
20.9
SD10.7(p=0.28)
S,surgery;AI,acetabularindex;SD,standarddeviation.
a Non-significantdifferenceinrelationtotheearlinessoftheintervention(p=0.7).
rev bras ortop.2014;49(4):350–358
355
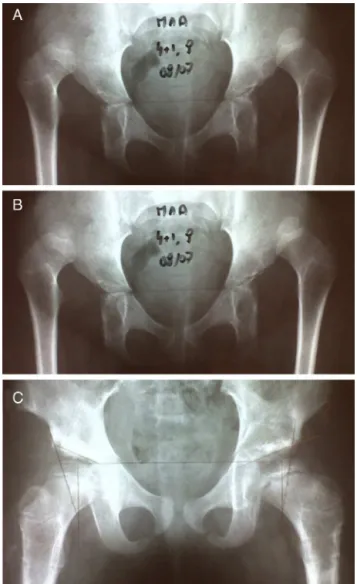
Fig.1–Femalepatientagedfouryearsandonemonth: preoperativeX-rayinAugust2007(A).X-rayonAugust16, 2009,twoyearsandfivemonthsafteroperationonright hipandoneyearandsixmonthsafteroperationonlefthip (B).X-rayonOctober2,2010,threeyearsandthreemonths afteroperationonrighthipandtwoyearsandeight monthsafteroperationonlefthip,presentingtypeI necrosisofthefemoralhead(C).
osteotomy.Amongthe10patientswithbilateralinvolvement, 10jointswereoperatedbetweentheagesoftwoandfouryears andtheothertenjointsbetweenfourandsevenyearsofage,
withamean interval offour monthsbetween thesurgical
procedures.
Bertoletal.20evaluated103hipsofeightboysand85girls
(10bilateralcases).Allofthemunderwentopenreductionand Salter’sosteotomy,withorwithoutassociatedrotationaland varusosteotomyofthefemur.Inoursample,wedidnot per-formvaruscorrection.
CarvalhoFilhoetal.2evaluatedthreeboysand15girls(four
bilateralcases)whohadalreadystartedtowalk,withDDHthat hadnotbeentreatedpreviously.Thesurgerywasperformedin asingleprocedureandthepatients’meanagewas19months. Rochaetal.23analyzed18femalehipsthatunderwentopen
reduction,Salter’sosteotomyandOmbrédanne’sprocedureat
Fig.2–Femalepatientagedthreeyearsandthreemonths: preoperativeX-rayinJune2004(A).X-rayinJanuary2005, threemonthsafteroperationonlefthipandsixmonths afteroperationonrighthip(B).X-rayinOctober2011,inthe latepostoperativeperiod,sevenyearsafteroperationon righthipandsixyearsandninemonthsafteroperationon lefthip,presentingtype4necrosisofthefemoralhead(C).
agesbetweentwoandeightmonths,inwhichfourcaseswere bilateral.Inthesebilateralcases,themeantimebetweenthe surgicalprocedureswassixmonths.
El-Sayedetal.24treated87patientswithDDHbymeansof
openreductionandSalter’sosteotomy.Therewere22 bilat-eralcases,whichwereoperatedwithanintervalofsixweeks. Bhuyan25waitedthreetosixmonthstoperformtheprocedure
onthecontralateralhip.
Regardingthepostoperativefollow-uponthepatientsof thepresentstudy,themeandurationwas5.8years.Carvalho Filhoetal.2followeduptheirpatientsforameanoffouryears,
Fig.3–Femalepatientagedtwoyears:preoperativeX-ray inMarch1998(A).X-rayinJuly2007:postoperative
radiographiccontrolproducednineyearsandeightmonths afteroperationonrighthipandnineyearsandtwomonths afteroperationonlefthip(B).X-rayinAugust2011,atthe ageof15yearsand11months:13yearsandeightmonths afteroperationonrightsideand13yearsandtwomonths afteroperationonleftside(C).
Manyauthorshavedescribedfollow-upsontreatedpatients rangingfromoneyearto24yearsandsixmonths.11,20,21,23–32
Regardingradiographicevaluations,themeanpreoperative AIamongthecasesstudiedherewas38◦,withameanvalue fortherightsideof36.9◦andfortheleftsideof39◦.Regarding theAIsixweeksaftertheoperation,themeanvaluewasfound tobe21.8◦,therightside22.8◦andtheleftside20.8◦.Themean forthelatepostoperativeAIwas18.2◦.Therewasastatistically significantdifferencebetweenthepre-andpostoperativeAIs (p<0.05).
CarvalhoFilhoetal.2foundapreoperativeangleof39◦and ameanpostoperativeangleof22◦.
Rochaetal.23foundpreoperativemeanvaluesof43.3◦on therightsideand42.1◦ontheleftsideandpostoperative val-uesof31.57◦and30.36◦,respectively.Althoughthevalueswere higher,theyalsoobservedasignificantdifferencefrombefore toaftertheoperation(p<0.001).
Yagmurluetal.26performedSalterorSteelosteotomyon
six patients.Themean preoperativeAIwas 37.8◦, and this improvedto21.2◦aftertheoperation.
El-Sayedetal.24foundastatisticallysignificantdifference
betweenthepre-andpostoperativeAIvalues,which dimin-ishedfrom41.56◦to20.41◦inchildrenyoungerthanfouryears. Bhuyan26reducedtheAIfrom42◦ (±5)to21◦(±2).Abdullah etal.27obtainedasignificantimprovementinAIinallthe42
hips treated,thus decreasingit from 44◦ (±2.5)to23◦ (±3). Among63children,Changetal.11foundameanpreoperative
AIof35.4◦;theAIsixmonthsaftertheoperationwas17◦andit was12.6◦tenyearsaftertheoperation.Inourstudy,therewas adecreasingtrendinAIvalueswithpassageoftime, chang-ingto18.2◦,butwithoutanystatisticallysignificantdifference inrelationtothevaluesfromsixweeksaftertheoperation (p=0.06).
ThepostoperativeWibergCEangleobtainedinour
anal-ysiswas19.4◦, i.e.,smallerthantheanglesof28◦ foundby CarvalhoFilhoetal.,2 31◦ (±9)and32.3◦ (±11.9)byEl-Sayed etal.24and32.3◦(±11.9)inpatientswithSalter’sosteotomy and36.9◦(±10.5)incaseswithassociatedfemoralshortening treatedbyTezerenetal.28
TheradiographicclassificationdescribedbySeverinmakes itpossibletoassesstheresultsfromSalter’sosteotomyover themediumandlongterms.Inourstudy,wefoundthat65%of thehipshadasatisfactoryradiographicresult.Betterresults were foundby CarvalhoFilhoet al.,2 with81% ofthe hips
in classificationsIand II; Prado etal.,21 with92.8%;Rocha
etal.,23with88.9%;El-Sayedetal.,24with88%(typesIandII);
Bhuyan,25with83.3%;andYagmurluetal.,26with74%showing
satisfactoryresults.
Femoralshorteningwasperformedon24hips,withoutany difference inthe radiographic evaluationinrelationto the caseswithout shortening. Bertolet al.20 foundthat 75%of
the resultswere goodinthe caseswithout shorteningand
64.4% inthe caseswith femoral shortening. Prado et al.21
performed femoralshorteningon alloftheir patientswith
bilateral involvement. They suggested that femoral
short-ening should be used as an auxiliary surgical treatment
methodforDDH,sincethefinalresultdependsonthe pro-ceduresusedinaddressingthejointproblem.Theyreported that,becauseofthediminishedorevenabsentpotentialfor recoveryofacetabulardevelopment,simplereplacement pro-ceduresinchildrenoverthe ageofthreeyears giveriseto unsatisfactorymediumandlong-termresults.Asheyetal.34
indicatedfemoralshorteninginassociationwithsimpleopen reduction,forchildrenovertheageofthreeyears.Tezeren et al.28 evaluated their resultsand found SeverinI in 75%
and SeverinIIin18.7% ofthecasestreated without
short-ening and SeverinI in 76.9% and Severin IIin 23% of the
patientswhounderwentfemoralshorteningandconcluded
thattherewasnosignificantdifferencebetweenthe proce-dures.
InthestudybySalterandDubos,22amongthepatientswho
rev bras ortop.2014;49(4):350–358
357
In relation to the duration of immobilization after the
operation,Rochaetal.24kepttheirpatientsinplastercasts
fromthepelvistothe footfor2.5months,El-Sayedet al.25
fortwomonthsand Sadeghpour et al.35 forthreemonths,
i.e.,longerperiodsthanthesixweeksrecommendedinthe presentstudy.
Thetimeintervaluntilremovalofthesynthesismaterial rangedfromthreemonthstofiveyearsandtenmonths,with
a mean of21.63 months. Carvalho Filho et al.2 performed
removalofthesynthesismaterialbetweeneightandtwelve weeksaftertheoperation,whileRochaetal.24 didthis one
yearaftertheoperation.
Somecomplications from Salter’sosteotomy have been
described,such assuperficial and deep infection, subluxa-tion,renewed dislocation,chondrolysis, neuropraxia ofthe sciaticnerve andavascularnecrosis.22 In thepresent
sam-ple,therewere 15casesofavascularnecrosis, withoutany significantdifferencebetweenthesides.Wedidnotfindany casesofsuperficialordeepinfection.Therewerethreecases
ofreneweddislocation,whichwereresolvedthroughanew
surgicalprocedure.
Wenotedthat in thecases ofavascularnecrosis,
espe-cially those of types 3 and 4, seven (16.66%) occurred in
patientsofmoreadvancedageandwithhigherdislocation.
These required greater capsule release because of
adher-encesandtheconsequentresection,giventhatthecapsule iselongated,whichisprobablythereasonforthisincidence (p>0.08).
Bertoletal.20foundagreaterrateofgrowthplateinjuryin
thegroupinwhichassociatedfemoralshorteningwas
per-formed(p<0.05), aswell asmorecasesofsubluxationand dislocation.Pradoetal.21reportedfourcasesofsubluxation
(9.5%). Rocha et al.23 had one case of subluxation, one of
osteonecrosisandoneotherofosteonecrosisassociatedwith subluxation.
Changetal.11 operatedon63childrenbetweentheages
of one and three years, using the technique described by
Salter, and found 30 cases ofavascular necrosis: 16 cases withearlysigns ofthis,withinthefirst twoyears afterthe operation,and14 withsignsseen lateronafterthe opera-tion.
Yagmurlu et al.26 described four cases with avascular
necrosisamong27hipsthatwere operated(14%).They did
not cite the classification used, or the likely cause of the event.
Roposchetal.36foundthat73%oftheircasespresented
avascularnecrosis(86/118)overameanfollow-upperiodof eightyears(oneto19years),accordingtothecriteriaofOgden andBucholz,amongthepatientstreatedwithopenandclosed reduction,andtheyconcludedthattherewasnorelationship withperformingfemoralshortening.
Weconsideredthatreneweddislocationandbone
necro-sispredisposedpatientstopoorfunctionalandradiographic results.Amongthepatientsstudied,thegradeencountered rangedfromtypesItoIVofKalamchiandMacEwen,andwas mostfrequentlytypeII,with11.9%(5/42),followedbytypeIII, with9.52%(4/42).Theseresultswereconcordantwiththoseof Holmanetal.,37whofound10casesofnecrosis,allclassified
asSeverinIVorworse,amongtheirresultsfromtreatments usingdifferenttechniqueson179hips.
Conclusions
Open reductionin association with osteotomy ofthe iliac
boneas describedbySalter presenteda statistically
signif-icantimprovementintheangularparametersmeasuredon
thepatients’radiographs,frombeforetoaftertheoperation.
This improvement did not have any relationship with
whetherfemoralshorteningasdescribedbyOmbrédannewas
performed.
Therewasnosignificantdifferenceregardingtheresults betweenthesidesoperated.
Avascular necrosis of the femoral head was the most
prevalent complication in the group studied and this had
arelationshipwithhigherdislocationandpatientsofmore advancedage.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.WilkinsonAG,WilkinsonS.Neonatalhipdysplasia:anew perspective.NeoReviwes.2010;11(7):e349–62.
2.CarvalhoFilhoG,ChueireAG,IgnácioH,CarneiroMO, FranceseNetoJ,CanesinAC.Tratamentocirúrgicodaluxac¸ão congênitadoquadrilpósmarcha:reduc¸ãoabertae
osteotomiadeSalter.ActaOrtopBras.2003;11(1):42–7. 3.BowenJR,Kotzias-NetoA.Developmentaldysplasiaofthe
hip.Brooklandville:DataTracePublishingCompany;2006. 4.Wynne-DaviesR.Acetabulardysplasiaandfamilialjoint
laxity:twoetiologicalfactorsincongenitaldislocationofthe hip.Areviewof589patientsandtheirfamilies.JBoneJoint SurgBr.1970;52(4):704–16.
5.DunnPM.Theanatomyandpathologyofcongenital dislocationofthehip.ClinOrthopRelatRes.1976;(119):23–7. 6.WilkinsonJA.Apost-natalsurveyforcongenital
displacementofthehip.JBoneJointSurgBr.1972;54(1):40–9. 7.OrtolaniM.Unsegnopoconotoesuaimportanzaperla
diagnosiprecocediprelussazionecongenitadell’anca.La Pediatria.1937;45:129–35.
8.SalterRB.Theclassic.Innominateosteotomyinthe treatmentofcongenitaldislocationandsubluxationofthe hipbyRobertB.Salter.J.BoneJointSurg(Brit).43B:3:518,1961. ClinOrthopRelatRes.1978;(137):2–14.
9.PuttiV.Earlytreatmentofcongenitaldislocationofthehip.J BoneJointSurgAm.1933;15(1):16–21.
10.OrtolaniM.Congenitalhipdysplasiainthelightofearlyand veryearlydiagnosis.ClinOrthopRelatRes.1976;(119):6–10. 11.ChangCH,KaoHK,YangWE,ShihCH.Surgicalresultsand complicationsofdevelopmentaldysplasiaofthehip–one stageopenreductionandSalter’sosteotomyforpatients between1and3yearsold.ChangGungMedJ.
2011;34(1):84–92.
12.OmbrédanneL.Préciscliniqueetopératoiredechirugie infantile.Paris:Masson;1923.
13.SalterRB.Roleofinnominateosteotomyinthetreatmentof congenitaldislocationandsubluxationofthehipintheolder child.JBoneJointSurgAm.1966;48(7):1413–39.
15.GadeHG.Acontributiontothesurgicaltreatmentof osteoarthritisofthehip-joint.Oslo:Grøndahl&Søns;1947. 16.WibergGC.Studiesondysplasticacetabulaandcongenital
subluxationofthehipjoint,withspecialreferencetothe complicationofOsteo-Arthritis(TranslatedfromtheSwedish byHelenFrey).ActaChirScand.1939;83Suppl.58.
17.SeverinEA.Contributiontotheknowledgeofcongenital dislocationofthehipjoint.Lateresultsofclosedreduction andarthrographicstudiesofrecentcases(Translatedfrom theSwedishbyHelenFrey);1941.
18.KalamchiA,MacEwenGD.Avascularnecrosisfollowing treatmentofcongenitaldislocationofthehip.JBoneJoint SurgAm.1980;62(6):876–88.
19.Estatísticapormeiodainternet.Availablein:
www.sestatnet.ufsc.br[Online][cited2012January15]. 20.BertolP,IshidaA,MacnicolMF.Tratamentodadisplasiado
desenvolvimentodoquadrilpelatécnicadeSalterisoladaou associadaàosteotomiadofêmur.RevBrasOrtop.
2004;39(5):232–44.
21.PradoJC,SantiliC,BaptistaPPR.Tratamentodaluxac¸ãoe subluxac¸ãocongênitasdoquadrilpelatécnicadeSalter associadaaoencurtamentodofêmur.RevBrasOrtop. 1984;19(6):203–8.
22.SalterRB,DubosJP.Thefirstfifteenyear’spersonal experiencewithinnominateosteotomyinthetreatmentof congenitaldislocationandsubluxationofthehip.Clin OrthopRelatRes.1974;(98):72–103.
23.RochaVL,ThoméAL,CastroDL,OliveiraLZ,MoraesFB. Avaliac¸ãoclínicaeradiológicaapósprocedimentodeSaltere Ombrédannenadisplasiadedesenvolvimentodoquadril. RevBrasOrtop.2011;46(6):650–5.
24.El-SayedM,AhmedT,FathyS,ZytonH.TheeffectofDega acetabuloplastyandSalterinnominateosteotomyon acetabularremodelingmonitoredbytheacetabularindexin walkingDDHpatientsbetween2and6yearsofage:short-to middle-termfollow-up.JChildOrthop.2012;6:471–7. 25.BhuyanBK.Outcomeofone-stagetreatmentof
developmentaldysplasiaofhipinolderchildren.IndianJ Orthop.2012;46(5):548–55.
26.YagmurluMF,BayhanIA,TuhaniogluU,KilincAS,KarakasES. Clinicalandradiologicaloutcomesarecorrelatedwiththeage ofthechildinsingle-stagesurgicaltreatmentof
developmentaldysplasiaofthehip.ActaOrthopBelg. 2013;79(2):159–65.
27.AbdullahES,RazzakMY,HusseinHT,El-AdwarKL,Youssef AA.Evaluationoftheresultsofoperativetreatmentofhip dysplasiainchildrenafterthewalkingage.AlexandriaJMed. 2012;48:115–22.
28.TezerenG,TukenmezM,BulutO,PercinS,CekinT.The surgicaltreatmentofdevelopmentaldislocationofthehipin olderchildren:acomparativestudy.ActaOrthopBelg. 2005;71(6):678–85.
29.ErtürkC,AltayMA,Yarimpapuc¸R,KorukI,Is¸ikanUE. One-stagetreatmentofdevelopmentaldysplasiaofthehipin untreatedchildrenfromtwotofiveyearsold.Acomparative study.ActaOrthopBelg.2011;77(4):464–71.
30.DobashiET,KiyoharaRT,MatsudaMM,MilaniC,Kuwajima SS,IshidaA.Tratamentocirúrgicodoquadrildisplásico inveterado.ActaOrtopBras.2006;14(4):183–9.
31.HaidarRK,JonesRS,VergroesenDA,EvansGA.Simultaneous openreductionandSalterinnominateosteotomyfor developmentaldysplasiaofthehip.JBoneJointSurgBr. 1996;78(3):471–6.
32.CordeiroEF,MatsunagaFT,CostaMP,FelizolaM,DobashiET, IshidaA,etal.Análiseradiográficadosfatoresprognósticos doquadrildisplásicoinveterado.ActaOrtopBras.
2010;18(4):218–23.
33.ForlinE,MunhozdaCunhaLA,FigueiredoDC.Treatmentof developmentaldysplasiaofthehipafterwalkingagewith openreduction,femoralshortening,andacetabular osteotomy.OrthopClinNorthAm.2006;37(2):149–60. 34.AshleyRK,LarsenLJ,JamesPM.Reductionofdislocationof
thehipinolderchildren:apreliminaryreport.JBoneJoint SurgAm.1972;54(3):545–50.
35.SadeghpourA,RouhaniA,MohseniMA,AghdamOA,Goldust M.Evaluationofsurgicaltreatmentofdevelopmental dysplasiaofthehipforavascularnecrosisoffemoralheadin children.PakJBiolSci.2012;15(8):391–4.
36.RoposchA,RidoutD,ProtopapaE,NicolaouN,GelferY. Osteonecrosiscomplicatingdevelopmentaldysplasiaofthe hipcompromisessubsequentacetabularremodeling.Clin OrthopRelatRes.2013;471(7):2318–26.