w w w . r b o . o r g . b r
Original
Article
Analysis
on
the
results
from
percutaneous
extensor
osteotomy
of
the
distal
femur
in
patients
with
amyoplasia
夽
,
夽夽
Marcus
Vinicius
Moreira
∗,
André
Casari
Rimoldi,
Solange
Aoki
Associac¸ãodeAssistênciaàCrianc¸aDeficiente,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received10March2013 Accepted8October2013 Availableonline5May2014
Keywords: Arthrogryposis Osteotomy Knee
a
b
s
t
r
a
c
t
Objective:toreviewthemedicalfilesof19patientswithadiagnosisofamyoplasia,who underwentpercutaneousextensorosteotomyofthedistalfemurtocorrectdeformitiesin whomthekneeswerefixedinflexion.
Methods:weanalyzed37osteotomyprocedureson35kneesthatpresentedaninitial defor-mity inwhich the knees werefixed inflexion at33.8◦.All ofthese kneesunderwent
percutaneousextensorosteotomyofthedistalfemurandwerefollowedupfora mean periodof73.7months.
Results:weobservedrecurrenceofthedeformityin29osteotomycases,i.e.in78.4%ofthem. Themeanrecurrencevelocityofthedeformitywas0.69◦/month.
Conclusion: percutaneousextensorosteotomyofthedistalfemurprovidedsufficient correc-tionofdeformitiesinwhichthekneewasfixedinflexionintheseamyoplasiacases,but therewasasignificantdegreeofrecurrenceamongthepatientsanalyzed.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Análise
de
resultados
da
osteotomia
extensora
percutânea
de
fêmur
distal
em
pacientes
com
amioplasia
Palavras-chave: Artrogripose Osteotomia Joelho
r
e
s
u
m
o
Objetivo:revisarosprontuáriosde19pacientescomdiagnósticodeamioplasia,submetidos àosteotomiaextensorapercutâneadefêmurdistal,paracorrec¸ãodedeformidadefixaem flexãodosjoelhos.
Métodos:analisamos37osteotomiasem35joelhoscommédiadedeformidadefixainicial médiaemflexãodosjoelhosde33,8◦,todossubmetidosàosteotomiapercutâneaextensora
dofêmurdistaleacompanhadosemmédiade73,7meses.
Resultados: observamosrecidivadadeformidadeem29osteotomias,ouseja,78,4%delas.A velocidademédiaderecidivadadeformidadefoide0,69◦/mês.
夽
Pleasecitethisarticleas:MoreiraMV,RimoldiAC,AokiS.Análisederesultadosdaosteotomiaextensorapercutâneadefêmurdistal empacientescomamioplasia.RevBrasOrtop.2014;49:345–349.
夽夽
WorkperformedattheCongenitalMalformationClinic,Associac¸ãodeAssistênciaàCrianc¸aDeficiente,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.V.Moreira).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Conclusão: aosteotomiaextensorapercutâneadofêmurdistalforneceucorrec¸ãosuficiente dadeformidadefixaemflexãodosjoelhosnaamioplasia,porémapresentousignificativo grauderecidivanospacientesanalisados.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Thetermarthrogryposisdescribesagroupofdiseasesthatare characterizedbytheirpresentationofmultiplejoint contrac-tures,withinvolvementoftwoormorejointsindifferentareas ofthebody.1
Arthrogryposis affects1:3000 livebirthsand its etiology ismultifactorial. There isa consensusthat it is related to restrictionoffetalmovementsafterthetenthweekof preg-nancy.Thisprocessisknownasafetalakinesia/hypokinesia sequence.2,3
Amyoplasiaisthecommonesttypeofarthrogryposis syn-drome,andoccursin38–47%ofthecases.2Itischaracterized byjointcontracturesthataffectallfourlimbs,symmetrically (84%ofthecases),withreplacementofthemuscletissuewith fibrotictissueandwithhemangiomaontheface.1
Thecontracturesmayaffectboththeupperandthelower limbs.The knee joints contribute tothe general incidence andprevalenceofthedeformities,andsuchdeformitiesare presentin70%ofthechildrenwithamyoplasia.Ofthese,48% ofthekneespresentabnormalitiesofflexion,21%extension and4%dislocation.1
Thetreatmentforpatientswithamyoplasiaiscomplexand multidisciplinary.Theaimsare tostimulateimprovedjoint mobility,achieveandmaintainalignmentsothatlessenergy isexpendedduringmobilization,promotetheuseoforthoses, stimulatewalkingatdifferentlevelswhenpossible;andattain independenceinactivitiesofdailyliving.4
Fixed deformities in which the knee is flexed are an obstacle tothe use oforthoses and leadto greater energy expenditureinpatientswhocanwalk,especiallywhenthe deformity is greater than 20◦. Such deformities may also
becomefactorsthatareharmfultoseatedposturesand trans-fers,andmaymakehygienedifficult.
Forfixeddeformitiescomprisingknee flexion,the
treat-ment should vary according to the degree of flexed
contracture. Deformities of up to 20◦ generally allow the
use of orthoses and therefore maintenance of qualities is proportionaltothepatient’scapacitytomovearound.Mild deformitiesofbetween20◦and40◦impedeorthosisuseand
commonly require surgical treatment. The possibilities for intervention include posterior soft-tissue release, percuta-neousextensorosteotomyofthedistalfemur,serialplaster casts or a combination of surgical techniques and serial plastercasts.Contractures ofgreater severity, greater than 40◦, require not only soft-tissue release but also extensor
osteotomyofthedistalfemur, withshortening,because of therisk ofstretching ofthesofttissuesand neurovascular lesions.Deformitiesofgreaterseveritymayrequiresoft-tissue releaseinassociationwithgradualcorrectionusingan exter-nalfixator.1,5–7Percutaneousextensorosteotomyofthedistal femurbecomesanoptionparticularly forfixeddeformities
ofbetween20◦ and 40◦,and hastheadvantageofminimal
soft-tissueinjury,whichfavorstheconsolidationprocessand reducesthechancesofinfection.8
Theaimofthe present study wasto analyzethe surgi-calresultsfrompatientswithadiagnosisofamyoplasiawho underwent correction ofknee flexion deformitiessolelyby meansofthetechniqueofpercutaneousextensorosteotomy ofthedistalfemur.
Materials
and
methods
This was a retrospective study in which we analyzed the medicalfilesofpatientswhowere followedupatthe Con-genitalMalformationClinicaloftheAssociationfortheCare of Disabled Children (Associac¸ão de Assistência à Crianc¸a Deficiente,AACD),withadiagnosisofamyoplasiaandfixed kneeflexiondeformity.Thesepatientsunderwentoperations onthedistalfemurbymeansofthepercutaneousextensor osteotomytechniquebetween1998and2009.
Thedataonextensiondeficitsreportedbeforeandafterthe surgicalprocedureforcorrectionofthekneeflexiondeformity wereused,alongwithdatafromtheoutpatientfollow-up.The degreeofkneeflexionusedasaparameterforthestudywas measuredfromtheobserveddeficitincompleteknee exten-sion.
Inanalyzingthemedicalfiles,wedidnotseeany descrip-tions regarding residual deformity during the immediate postoperative period.Thus, all theknees operatedreached completeextensionduringthesurgicalprocedure.Therefore, weclassifiedfixedkneeflexiondeformitiesacquiredafterthe surgeryasrecurrence.
Patients with postoperative follow-up of less than 18 monthsand patients who underwentother surgical proce-dureswiththesamepurpose,withtheexceptionofposterior releaseofkneesofttissues,wereexcluded.Wealsoexcluded patients who underwent the proposed procedure in other institutionsorwhosepostoperativefollow-upwasirregular.
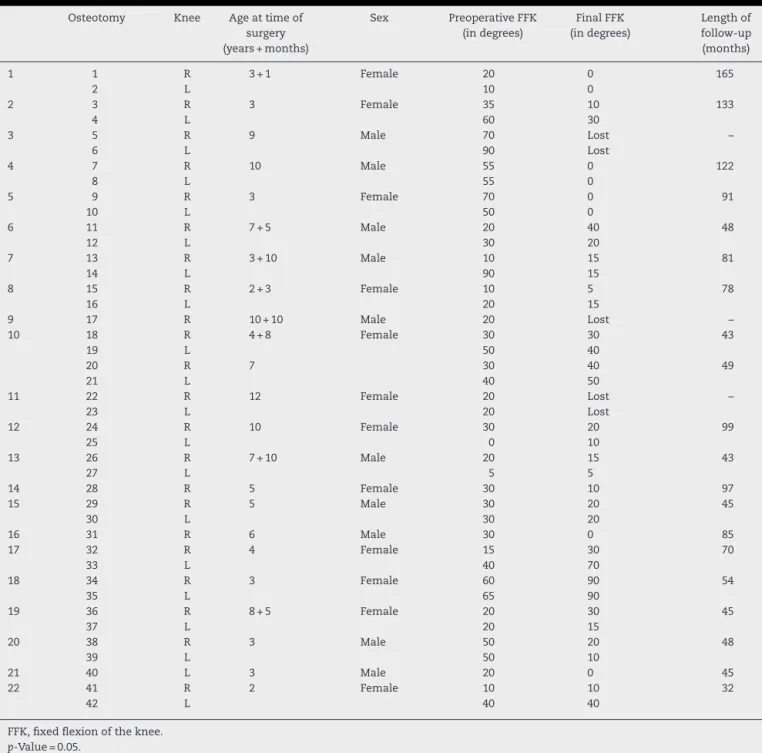
Table1–Clinicaldata.
Osteotomy Knee Ageattimeof surgery (years+months)
Sex PreoperativeFFK (indegrees)
FinalFFK (indegrees)
Lengthof follow-up (months)
1 1 R 3+1 Female 20 0 165
2 L 10 0
2 3 R 3 Female 35 10 133
4 L 60 30
3 5 R 9 Male 70 Lost –
6 L 90 Lost
4 7 R 10 Male 55 0 122
8 L 55 0
5 9 R 3 Female 70 0 91
10 L 50 0
6 11 R 7+5 Male 20 40 48
12 L 30 20
7 13 R 3+10 Male 10 15 81
14 L 90 15
8 15 R 2+3 Female 10 5 78
16 L 20 15
9 17 R 10+10 Male 20 Lost –
10 18 R 4+8 Female 30 30 43
19 L 50 40
20 R 7 30 40 49
21 L 40 50
11 22 R 12 Female 20 Lost –
23 L 20 Lost
12 24 R 10 Female 30 20 99
25 L 0 10
13 26 R 7+10 Male 20 15 43
27 L 5 5
14 28 R 5 Female 30 10 97
15 29 R 5 Male 30 20 45
30 L 30 20
16 31 R 6 Male 30 0 85
17 32 R 4 Female 15 30 70
33 L 40 70
18 34 R 3 Female 60 90 54
35 L 65 90
19 36 R 8+5 Female 20 30 45
37 L 20 15
20 38 R 3 Male 50 20 48
39 L 50 10
21 40 L 3 Male 20 0 45
22 41 R 2 Female 10 10 32
42 L 40 40
FFK,fixedflexionoftheknee.
p-Value=0.05.
Wefoundthat202patientswithadiagnosisof amyopla-siahadbeenfollowedupattheinstitution.Ofthese,65had undergoneasurgicalproceduretocorrectkneeflexion defor-mity.
Amongthese 65 patients, 19 were treated surgically by meansofcorrectionusinganexternalfixator,10underwent extensorosteotomyofthedistalfemur,withshortening,two underwentposteriorsoft-tissuereleasealoneand34 under-wentpercutaneousextensorosteotomyofthedistalfemur,in ordertocorrectthekneeflexiondeformity.
Amongthe34patientswhounderwenttheprocedurethat wasthefocusofthisstudy,10presentedinsufficientlengthof postoperativefollow-upandtwounderwenttheprocedureat otherservices.
Therefore, our sample included 22 patients with 42 osteotomieswhofulfilledthecriteriaforthisstudy.However, threepatientswho underwentosteotomydidnotmaintain their postoperative follow-up and were excluded from the analysisonthefinalresults.
Intheend,ouranalysisonthefinalresultswasbasedon 19operatedpatients(37osteotomies).
Results
Table2–Distributionofrecurrences.
Recurrence N % p-Value
No 8 21.6 <0.001
Yes 29 78.4
Table3–Correlationbetweendegreeofrecurrenceand age.
Age
Correlation −12.4%
p-Value 0.466
fourhadaunilateraldeformity.Oneofthepatientpresented recurrenceofthedeformitythreeyearsafterthefirst proce-dureandunderwentanewsurgicalprocedure.Threepatients whounderwentosteotomywerenotfollowedupatour insti-tution.Thus,therewasnorecordofpostoperativedataintheir cases.
Out ofthe 37 osteotomies performed and analyzed, we observedrecurrenceofthedeformityin29ofthem,i.e.78.4%
(Table2).Themeanvelocityofrecurrenceinthepresentstudy
was0.69◦/month,rangingfrom0.07◦to2.09◦/month.
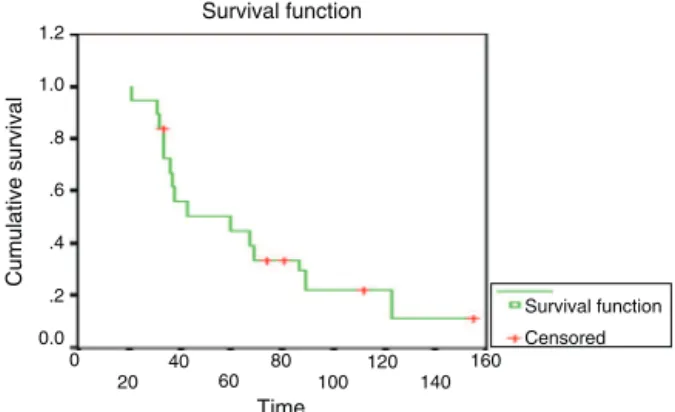
WeusedtheKaplan–Meierestimatortocalculate nonpara-metricreliabilityvaluesforasetofdatawithmultiplefailures. Inthisstudy,theKaplan–Meiersurvivalcurve(Fig.1)showed that50%ofthepatientswhounderwentthesurgical proce-durestudiedhereexperiencedrecurrencebeforereachingthe 48thmonthaftertheoperation.
Thepatients’meanageatthetimeofthesurgerywas5.8 years,witharangefrom2to12.Beforethesurgicalprocedure, themeanfixedflexionofthekneesamongthepatients ana-lyzedwas33.8◦,rangingfrom5◦ to90◦.Themeandegreeof
flexionafterpostoperativerecurrencewas22◦,rangingfrom
5◦to90◦.
Themeanpostoperativefollow-upperiodwas73.7months, witharangefrom32to165months.
From analysison the correlationbetween the degreeof recurrenceandage(Table3),thevalueobtainedwas−12.4%,
whichindicatesthatthevariableswereinverselyproportional andthecorrelationwasclassifiedas“poor”,withoutstatistical significance(p=0.466).
Thecorrelationbetweenthedegreeofrecurrenceandthe lengthofpostoperativeevolutionshowedavalueof−39.3%,
1.2
1.0
.8
.6
.4
.2 0.0 0
20 40
60 80
100 120
140 160
Time Survival function
Cumulative survival
Survival function Censored
Fig.1–Kaplan–Meiersurvivalcurve.
Table4–Correlationbetweendegreeofrecurrenceand lengthofevolution.
Evolution(months)
Correlation −39.3%
p-Value 0.016
whichindicatesthatthecorrelationwas“poor”,without sta-tisticalsignificance(Table4).
Discussion
Knee flexion deformity is one of the most challenging problems for orthopedic surgeons who treat patients with amyoplasia.Mildcontracturesofupto20◦donotstoppatients
fromwalking,buttheytendtoincreasetheenergy expendi-turethatisusuallynecessaryforwalkingthesamedistance. Contracturesofgreaterintensitynotonlypresentincreased energyexpenditurebutalsoroutinelymakeitdifficulttouse orthosesorimpedetheiruseforindependentwalking.Thus, surgicalproceduresaimtoreestablishalignment,soasto cor-rectandstimulatefunctionaldevelopment.9
In our series of cases, we found 202 patients with a diagnosis ofamyoplasia. Ofthese, 65 (32%) had knee flex-ion deformitiesthat requiredsurgical treatment. In acase series,Carlsonetal.10foundthat19.2%ofthepatientshad amyoplasiathatrequiredsurgicaltreatmentforcorrectionof kneeflexion.Svartmanetal.11foundthat10patients(17.8%) neededkneesurgery,outofatotalof56.
Percutaneous extensor osteotomyof the distalfemuris generallyapplicableforcorrectionofdeformitieslessthan40◦.
Thus,this isagoodoption, giventhatthetraining forthis technique iseasyand the surgicalmaterialsthatmightbe usedarewidelyavailable.Itsadvantagesincludealowerlevel ofsoft-tissueaggression(becauseofthesmallerincisionand lowerneedfordissection);smalleralterationstomuscleand periostealvascularization,withmaintenanceofasatisfactory bloodsupplytothesurgicalsite;lowerriskoftissue adher-ence;greaterstabilityatthefocusoftheosteotomy;greater potentialforconsolidation;andlowerriskofinfectionofthe operativewound.5,8,9,12
Thedisadvantagesofthistechniqueincludelowerability toviewtheoperationandimpossibilityofpromoting short-eningofthefemurwiththeaimofavoidingstretchingofthe neurovascularstructures.Theseconsiderablylimitthe appli-cabilityofthetechniqueanditspotentialforcorrectingthe deformity.
There isalso an importantmechanical factor; the cen-ter ofthe flexiondeformityisinthefemorotibialjoint and includesjointstructuresinitsphysiopathology,suchasthe posteriorjointcapsuleandtherespectiveligament,in asso-ciation withshortening ofthe knee flexors.Thetechnique analyzed here provides correctionthat occurs atan extra-articularsitebecauseoftheextensionofthedistalfemurin thesagittalplane.Thus,itisoutsideofthecenterof defor-mityanddoesnotaddressthestructuresthatgiverisetothe structuredflexion.
performed.Webelievethatrecurrenceofthedeformitymay bemultifactorial,causedbynonuse oforthosesduringthe postoperativeperiod,the greatpotentialforbone remodel-inginimmatureskeletons,lackofsoft-tissuereleaseinthe posteriorregionoftheknees,orevenvariationsinthe surgi-caltechnique.Svartmanetal.11mentionedthatdeformitiesin casesofamyoplasiawereofrecurrentnature,especiallywhen treatedinpatientsofyoungage.
Therecurrenceratewasalsohighlightedbymeansofthe Kaplan–Meiercurve,inwhich50%ofthepatientsexperienced recurrenceofthedeformitywithinthefirst48monthsafter theoperation.Thedatashowedthattherewasafailure to maintainthecorrectionthathadbeenmade,foralong-lasting period.
Thevelocityofrecurrenceencounteredinthisstudywas 0.69◦/month.Bevanetal.1reporteda1◦/monthandDelbello
andWatts5found0.9◦/month,whichwerebothforextensor
osteotomywithfemoralshortening.
Inourstudy,therewasanegativecorrelationbetweenage anddegreeofrecurrence.Thisshowsthatthevariableswere inverselyproportional,i.e.theyoungerthepatient’sage,the greaterwasthedegreeofrecurrenceofthedeformity. How-ever,the coefficientofcorrelationwasfoundtobe−12.4%,
whichreceiveda classificationof“poor” on thecorrelation scale,withoutstatisticalsignificance(p=0.466).Delbelloand Watts5 alsocorrelated youngagewiththedeformity recur-rencerateand foundanegativerelationship.Althoughour caseseriesdidnotshowanysignificantcorrelation,our clin-icalpracticesuggeststhatyoung ageisrelatedtoagreater deformityrecurrencerate.
Webelievethatthismedium-termfollow-upanalysison ourpatientswassufficienttoshowwhetherrecurrenceofthe deformityormaintenanceofthecorrectionwouldoccur.The meanfollow-upperiodwas73.7months.Therewasno sig-nificantcorrelationbetweenthedegreeofrecurrenceandthe lengthofthepostoperativefollow-up.
Therewasno intentionwiththis study tocomparethis surgicalmethodwithothermethodsusedforthesame pur-pose, which limits the applicability of the results to only thetechniqueanalyzedhere.Wetaketheviewthatstudies usingothersurgicaltechniquesandsubsequentcomparison betweenthem would be ofgreat importancefor providing moreobjectiveguidanceregardingthecharacteristicsof recur-renceofdeformitiesincasesofamyoplasia.Suchrecurrences couldbedueasmuchtovariationsinoperativetechniqueasto therecurrentnatureofthedeformitiesinthisdisease.Delbello andWatts5highlightedthedifficultymaintainingthe correc-tionobtainedduringthepostoperativeperiodandemphasized thatanewprocedureatanolderagemightbeneeded.
Despitetheresultsobtained,webelievethatthereisno jus-tificationforpostponingthecorrectiveprocedureuntilanage closertowhenskeletalmaturityisreached.Atthattime,the potentialforboneremodelingwouldbelower.Thebenefits, withregard notonly tofunctional and independent walk-ingbut alsotosocialinteractioninperformingactivitiesof dailyliving,exceedtherisksofundertakinganewsurgical approach.
Conclusion
Percutaneousextensorosteotomyofthedistalfemurprovided correctionofthesagittalalignmentofdeformedkneesthat werefixedinflexion,albeitthroughcreatingacompensatory deformityofextensionofthefemur.Therewasasignificant degreeofrecurrenceofthe deformityduringthe follow-up periodanalyzed.
Theplanningoftreatmentforthisgroupofpatientsneeds totakeintoconsiderationthebenefitsofthecorrections pro-posedandtheimprovementsinalignment,functionalresults andrisksofrecurrenceofdeformities.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BevanWP,HallJG,BamshadM,StaheliLT,JaffeKM,SongK.
Arthrogryposismultiplexcongenita(amyoplasia):an
orthopaedicperspective.JPediatrOrthop.2007;27(5):
594–600.
2.FilhoOB,SantosCE.Artrogriposemúltiplacongênita.In:
FernandesAC,RamosAC,CasalisME,HerbertSK,editors.
AACDmedicinaereabilitac¸ão–Princípioseprática.São
Paulo:ArtesMédicas;2007.p.69–76.
3.AlmanBA,GoldbergMJ.Síndromesdeimportância
ortopédica.In:MorrissyRT,WeinsteinSL,editors.Ortopedia
pediátricadeLovelleWinter.5aed.Barueri:Manole;2005.p.
317–27.
4.BamshadM,VanHeestAE,PleasureD.Arthrogryposis:a
reviewandupdate.JBoneJointSurgAm.2009;91Suppl.
4:40–6.
5.DelBelloDA,WattsHG.Distalfemoralextensionosteotomy
forkneeflexioncontractureinpatientswitharthrogryposis.J
PediatrOrthop.1996;16(1):122–6.
6.StaheliLT,HallJG,JaffeKM,PaholkeDO.Arthrogryposis:a
textatlas.Cambridge:CambridgeUniversityPress;1998.
7.ThomasB,SchoplerS,WoodW,OppenheimWL.Thekneein
arthrogryposis.ClinOrthopRelatRes.1985;(194):87–92.
8.IacovoneM.Osteoclasiacomperfurac¸õesósseas:método
paracorrec¸ãodedeformidadesdosmembrosinferiores:
estudobaseadoem44operac¸ões[tese].SãoPaulo:Faculdade
deMedicinadaUniversidadedeSãoPaulo;1981.
9.ZimmermanMH,SmithCF,OppenheimWL.Supracondylar
femoralextensionosteotomiesinthetreatmentoffixed
flexiondeformityoftheknee.ClinOrthopRelatRes.
1982;(171):87–93.
10.CarlsonWO,SpeckGJ,VicariV,WengerDR.Arthrogryposis
multiplexcongenita.Along-termfollow-upstudy.Clin
OrthopRelatRes.1985;(194):115–23.
11.SvartmanC,FucsPM,KertzmanPF,KampePA,RossetiF.
Artrogriposemúltiplacongênita–Revisãode56pacientes.
RevBrasOrtop.1995;30(1/2):45–52.
12.SödergårdJ,RyöppyS.Thekneeinarthrogryposismultiplex