w w w . r b o . o r g . b r
Original
Article
Description
of
an
evaluation
system
for
knee
kinematics
in
ligament
lesions,
by
means
of
optical
tracking
and
3D
tomography
夽
,
夽夽
Tiago
Lazzaretti
Fernandes
a,∗,
Douglas
Badillo
Ribeiro
a,
Diogo
Cristo
da
Rocha
a,
Cyro
Albuquerque
b,
César
Augusto
Martins
Pereira
a,
André
Pedrinelli
a,
Arnaldo
José
Hernandez
aaInstituteofOrthopedicsandTraumatology,HospitaldasClínicas,MedicalSchool,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
bDepartmentofMechanicalEngineering,UniversityCenterofFundac¸ãoEducacionalInaciana(FEI),SãoBernardodoCampo,SãoPaulo,
SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29August2013 Accepted3October2013 Availableonline28August2014
Keywords: Kneejoint
Anteriorcruciateligament X-raycomputedtomography
a
b
s
t
r
a
c
t
Objective:Todescribeanddemonstratetheviabilityofamethodforevaluatingknee kine-matics,bymeansofacontinuouspassivemotion(CPM)machine,beforeandafteranterior cruciateligament(ACL)injury.
Methods:Thisstudywasconductedonakneefromacadaver,inamechanicalpivot-shift simulator,withevaluationsusingopticaltracking,andalsousingcomputedtomography. Results:Thisstudydemonstratedtheviabilityofaprotocolformeasuringtherotationand translationoftheknee,usingreproducibleandobjectivetools(error<0.2mm).The mech-anizedprovocationsystemofthepivot-shifttestwasindependentoftheexaminerand alwaysallowedthesameangularvelocityandtractionof20Nthroughoutthemovement. Conclusion: Theclinicalrelevanceofthismethodliesinmakinginferencesabouttheinvivo behaviorofakneewithanACLinjuryandprovidinggreatermethodologicalqualityinfuture studiesformeasuringsurgicaltechniqueswithgraftsinrelativelyclosepositions.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Descric¸ão
de
sistema
de
avaliac¸ão
da
cinemática
do
joelho
em
lesões
ligamentares
a
partir
de
rastreamento
óptico
e
tomografia
3D
Palavras-chave: Articulac¸ãodojoelho Ligamentocruzadoanterior
r
e
s
u
m
o
Objetivo:Descreveredemonstraraviabilidadedeummétododeavaliac¸ãodacinemáticado joelho,pormeiodeumaparelhodeCPM(continuouspassivemotion),anteseapósalesãodo ligamentocruzadoanterior(LCA).
夽
Pleasecitethisarticleas:FernandesTL,RibeiroDB,daRochaDC,AlbuquerqueC,PereiraCAM,PedrinelliAetal.Descric¸ãode sis-temadeavaliac¸ãodacinemáticadojoelhoemlesõesligamentaresapartirderastreamentoópticoetomografia3D.RevBrasOrtop. 2014;49(5):513–19.
夽夽
WorkdevelopedattheInstituteofOrthopedicsandTraumatology,HospitaldasClínicas,MedicalSchool,UniversidadedeSãoPaulo, SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](T.L.Fernandes). http://dx.doi.org/10.1016/j.rboe.2014.08.005
Introduction
Anteriorcruciateligament(ACL)reconstructionisoneofthe orthopedics’surgicalproceduresmostperformedtoday.Ithas beenestimatedthatapproximately200,000suchprocedures areperformedintheUSAeveryyear.1
Despite the large number of studies that have been conductedin relation to ACL reconstruction,2,3 the rate of excellentorgoodresultsrangesfrom69%to95%.4 Unsatisfac-toryresultsmayresultfrompersistentinstabilityoftheknee andconsequentdifficultyinreturningtothepreviouslevelof physicalactivity.5–9
ACLinsufficiencyisrepresentedbyanteriortranslationof thetibiaandbyrotationalinstabilityoftheknee.10Thepivot shifttestisusedtoevaluatetherotationalstabilityoftheknee afterACLinjury.11Someauthorshavedemonstratedthatthe presenceofapositivepivotshifttestispredictivefor develop-mentofosteoarthrosisandpoorfunctionalresults.12–15
Althoughthepivotshifttestisveryspecific(closeto100% under anesthesia),16–19 its resultis subjective because it is examiner-dependent.Therefore,itistooimpreciseforusein scientificstudies.10,15,18–21
Musahletal.20 demonstratedthatthemechanizedpivot shifttest,whichconsistsofusingacontinuouspassivemotion (CPM) machine to perform combined knee movements of internalrotation,valgusrotationandflexion,hasgreater accu-racythanthemanualtest.
Inconjunction with computer-assistedsurgerysystems, thepivotshiftsystemcanbemeasuredsatisfactorilyandbe usedtoanalyzekneestabilityafterdifferentACL reconstruc-tiontechniques.10,22
Thus,thepresentstudyhadtheobjectiveofdescribinga methodforkinematicevaluationofthekneebeforeandafter ACLinjury,bymeansoftechnologiesthatmakeitpossibleto objectivelyassesskneeligamentstability.23
For this, we present below the mechanized pivot shift apparatusandanopticaltrackingsysteminassociationwith computedtomography.
Materials
and
methods
Thisexperimentwasconductedonaknee fromacadaver, inconformitywithapprovalfromourinstitution’sResearch
EthicsCommittee.Thecadaver’sentirelowerlimbwasused, withpreservationofthehipandanklejoints.
Asinclusioncriteria,thekneeselecteddidnotpresentany previousACLinjuryorotherligamentinjuries,therewasno moderateorsevereosteoarthrosisandtherewasnoevidence offracturingordisplacedalignmentofthemechanicalaxisof thelimb.
Beforetheexperimentwasstarted,deinsertionandmuscle sectioningwereperformedinordertoenablefullkneerange ofmotion,asfollows:tenotomyoftheadductormassatits origininthepubis;sectioningofthequadricepsandhamstring musclesattheirorigin;andtenotomyofthecalcanealtendon.
Instrumentedpivotshiftandrotationalstabilityofthe knee
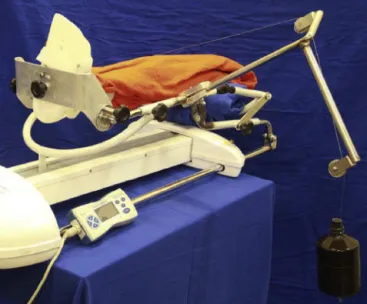
The mechanical pivot shift simulator was developed in the BiomechanicsLaboratory(LIM-41),startingfrom aCPM machine(Carci,Ortomed4060;ANVISA:10314290029)similar tothemodelusedandvalidatedbyBedietal.24
Thepelviswasstabilizedonthesurgicaltableandthehip andkneewereallowedtohavefullrangesofmotion.No sup-portusingbandsandthefemurortibialevelwasprovided.
TheCPMdevicewasdesignedtoallow15◦ofinternalankle
rotation,forboththeleftandfortherightlowerlimbs.Axial compressionoftheanklewasperformedatanangularvelocity of1.62◦/s,frommaximumextensionto50◦ofkneeflexion20
(Fig.1).
Themomentofinternalandvalgusrotationofthekneewas determinedbymeansofasystemofcablesandpulleys cou-pledtotheCPMdevice.Thepointoftractiononthetibiawas definedbymeansofatitaniumpinfixedperpendicularlyto thetuberosityoftibia,oflength10cm.Thetractionofthe tita-niumpinwasperpendiculartotheaxisofthetibiaandhadthe sameforcevectorof20N25throughouttheflexion–extension movement(0–50◦)20(Fig.2).
Measurementoftheanteriortranslationofthetibia
Fig.1–Mechanizedpivotshiftsystem.
Theverticalforce applied,inaccordance withthestudy by Bedietal.,26was68Nwiththekneeflexedat30◦.
Opticaltrackingsystem
Thetrackingsystem(MicronTracker 2,model H40) madeit possibletoobtainthespatialpositioningofthefemurandtibia throughidentifyingopticalmarkersanddeterminingtheknee translationandrotationmovements.
ThreeopticalmarkersweredistributedalongtwoL-shaped acrylicpiecesandwerefixedtothefemurandtibiausingtwo titaniumpins,inordertocreatearigidsystem(Fig.3).
Acomputerroutinewas developed(usingthe manufac-turer’slibrary,intheBasiclanguage)inordertorecognizeand savethethree-dimensionaldata(XYZ)thatwascapturedby thecamerasoftheopticaltrackingsysteminrealtime(15Hz, withmeasurementprecisionof0.2mm,accordingtothe man-ufacturer)(Fig.4).
Thecentralpointoftheknee,whichwasusedasa refer-encepointforcalculatingthekneerotationandtranslation,
Fig.2–Tractionsystemusingcablesandpulleys.
Fig.3–L-shapedopticalmarkersonthefemurandtibia.
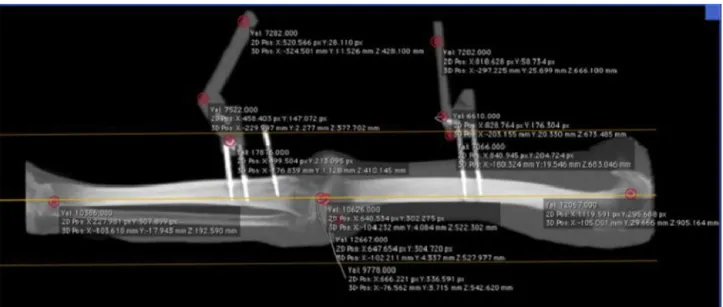
wasdefinedfromcomputedtomographyontheentirelimb afterthetestshadbeenfinished(Fig.5).
For there to be correspondence between the optical trackingsystemandthecomputed tomography,radiodense filamentswereincludedinthecentralpositionsoftheoptical markers(Fig.6).
The knee movement was calculated from rotation and translationmatricesbetweenthecoordinatesystemsofthe camera and tomography and the coordinate systems pos-itionedonthebariummarkersandonthecenteroftheknee. Atthispoint,coordinatesystemswerecreatedforthetibia andfemur.Oneoftheaxescoincidedwiththerespectiveaxis ofeachbone:onehorizontalandtheothervertical.Thesetwo coordinatesystemsweredetermined,foreachtimeinstant, bythecoordinatesystemsofthemarkers.
Therotationaroundtheaxesandthetranslationofthe cen-tralpointofthekneewereobtainedbymeansoftherotation andtranslationmatrixbetweenthefemoralandtibial coordi-natesystems.ThisprocedurewasdevelopedusingtheGNU Octavecomputersoftware.
Protocol
The testswere carried out in twostages: before and after dissection,underdirectviewingoftheACLatitsoriginand insertion.
Ateachstage,threemeasurementsoftheanterior trans-lationofthetibiaweremadeusingamanualdynamometer (68N) and three measurements of knee flexion–extension were made using the mechanizedpivotshift, asdescribed earlier.
Results
The knee used was the right knee of a 45-year-old male cadaver.
Fig.4–Three-dimensionalidentificationoftheopticalmarkers.
Fig.5–Mechanicalaxisofthelowerlimb:three-dimensionalpointsatthecenterofthefemoralheadandankle. Radiodenseandopticalmarkersonthefemurandtibia.
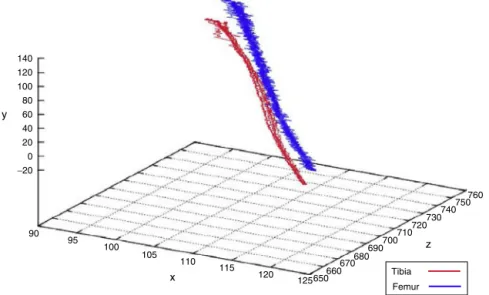
Theincreaseinthedistancebetweenthepositionsofthe centerofthefemurandthecenterofthetibia,between maxi-mumextensionandmaximumflexionofthekneerepresents thepivotshiftphenomenon(Fig.8,redline).
Fig.9showstheanteriortranslationofthetibiawiththe kneeflexedat30◦inrelationtothefemur,beforeandafter68N
or15lb25oftractionthroughthetitaniumpin,perpendicularly tothetibia.
140 120 100 80 60 40 20 0
−20
90 95
100 105
110 115
120
760 750 740 730 720 710 700 690 680 670 660 650 125
y
x Tibia
Femur
z
Fig.7–Graphicalrepresentationofkneemovementinthespaceofthecentralpointsofthefemurandtibia.
Fig. 10 shows a polar graph representing the combined translationandrotationmovementsofthetibia,inrelation tothefemurduringkneeflexionandextension.
Discussion
The main contribution of this study is that it shows the viabilityofaprotocolformeasuringkneetranslationand rota-tion usingobjective and reproducibletools(error<0.2mm). Moreover, the technology that was developedfor correlat-ing betweenthe opticaland tomographic systemsand the computationalmethodologyfordescribingthemovementare Brazilianintellectualproperty.
Laneetal.10reportedthataclinicalgradingsystem describ-ingkneestabilityintermsofkneeglide,kneeclunkingand
grossstabilityisvaluableforexperiencedorthopedists. How-ever,thissystemissubjectiveandnotreproduciblebetween surgeonsand,forthisreason,shouldnotbeusedinscientific studies.27
Themechanizedchallenge systemofthepivotshifttest isindependentoftheexaminerandalwaysallowsthesame angularvelocityandtraction of20Nthroughoutthe move-ment. Because the test is mechanized, this also reduces the risk ofbiasand increases theinternal validityofsuch studies.28 Consequently,thequality andrepresentativeness ofthesestudiesarealsoincreased.
Anotherimportanttechnicalnoterelatingtothepresent methodology relates to the use of tomography for defin-ingthecenterofkneerotation.Thisselectioncanbemade after the end of the experiment and it is possible, for example, to define the translation of the tibia in relation
10
8
6
4
2
0
−2
0 20 40 60 80 100
Angle, ^o
120 140 160 180
Femur-tibia Tibia Femur
Time, s
−0.5
−1
0 1 2 3 4 5 6 7 8 9
Time, s
Intact Injured
Fig.9–Anteriortranslationofthetibiaaftertractionof68Nbymeansofametalpininthetibialtuberosity(after4s).Blue line–intactACL;redline–injuredACL.(Forinterpretationofthereferencestocolorinthisfigurelegend,thereaderis referredtothewebversionofthisarticle.)
to the femur, in the lateral, medial or intercondylar com-partments. Three-dimensional computed tomography also enablesreconstructionoftheknee inanyplaneandallows kneealignmentandcorrectmeasurementofthepositionsof thefemoralandtibialtunnels.29,30
Thepivotshiftphenomenon presentedinFig. 8is con-cordant with what was shown by Bull et al.,31 in which subluxationofthe kneeoccurred atflexionofbetween25◦
and36◦.Otherstudieshavedemonstratedreductionofknee
subluxationatflexionofbetween40◦and44◦.10
Onemethodological limitation ofbiomechanicalstudies relatestocarryingout experimentsattimezero,i.e. imme-diatelyafterthesurgicalprocedureforACLreconstruction.In ourstudyspecifically,becausenoligamentreconstructionwas performed,therewerenochangestothemechanical proper-tiesofgraftsduringanyperiodofbiologicalintegrationthat couldhaveinfluencedtheanalysisontheresultspresented.
Furtherstudiesaredesirable,inordertobiomechanically analyzetheknee withtunnelsindifferentanatomical pos-itions.Crossetal.32arguedthattherewasnoconsensusin
Intact ACL Injured ACL
Extension Flexion
Translation [mm]
Axial rotation [
°]
5
4
3
2
1
0
0 2 4 6 8 10 12
Fig.10–Polarrepresentationofthecombinedtranslation androtationoftheknee.
theliteratureregardingwherewithintheoriginalfootprintthe ACLtunnelshouldbeconstructed.
Conclusion
Theclinical importanceofthepresent study relates tothe inferences thatcanbemade regardingthe invivobehavior ofknees withACL injuriesand the greater methodological qualitythatcanbeprovidedinfuturestudiesregarding mea-surements on surgical techniques with grafts in relatively closepositions.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.NationalInstitutesofHealth(NIH),NationalInstituteof ArthritisandMusculoskeletalandSkinDiseases(NIAMS), VanderbiltUniversity,UnitedStates.Prognosisandpredictors ofACLreconstruction–amulticentercohortstudy.Disponível em:http://clinicaltrials.gov/ct2/show/NCT00463099.
2.GirgisFG,MarshallJL,MonajemA.Thecruciateligamentsof thekneejoint.Anatomical,functional,andexperimental analysis.ClinOrthopRelatRes.1975;(106):216–31.
3.OdenstenM,GillquistJ.Functionalanatomyoftheanterior cruciateligamentandarationaleforreconstruction.JBone JointSurgAm.1985;67(2):257–62.
4.ArakiD,KurodaR,KuboS,FujitaN,TeiK,NishimotoK,etal. Aprospectiverandomisedstudyofanatomicalsingle-bundle versusdouble-bundleanteriorcruciateligament
5. GeorgoulisAD,RistanisS,ChouliarasV,MoraitiC,StergiouN. TibialrotationisnotrestoredafterACLreconstructionwitha hamstringgraft.ClinOrthopRelatRes.2007;(454):89–94. 6. KvistJ.Rehabilitationfollowinganteriorcruciateligament
injury:currentrecommendationsforsportsparticipation. SportsMed.2004;34(4):269–80.
7. LieDT,BullAM,AmisAA.Persistenceoftheminipivotshift afteranatomicallyplacedanteriorcruciateligament reconstruction.ClinOrthopRelatRes.2007;(457):203–9. 8. TashmanS,KolowichP,CollonD,AndersonK,AnderstW.
DynamicfunctionoftheACL-reconstructedkneeduring running.ClinOrthopRelatRes.2007;(454):66–73. 9. BediA,MusahlV,LaneC,CitakM,WarrenRF,PearleAD.
Lateralcompartmenttranslationpredictsthegradeofpivot shift:acadavericandclinicalanalysis.KneeSurgSports TraumatolArthrosc.2010;18(9):1269–76.
10.LaneCG,WarrenRF,StanfordFC,KendoffD,PearleAD.Invivo analysisofthepivotshiftphenomenonduringcomputer navigatedACLreconstruction.KneeSurgSportsTraumatol Arthrosc.2008;16(5):487–92.
11.GalwayHR,BeaupreA,MacIntoshDL.Pivotshift:aclinical signofsymptomaticanteriorcruciatedeficiency.JBoneJoint SurgBr.1972;54:763–4.
12.JonssonH,Riklund-AhlströmK,LindJ.Positivepivotshift afterACLreconstructionpredictslaterosteoarthrosis:63 patientsfollowed5–9yearsaftersurgery.ActaOrthopScand. 2004;75(5):594–9.
13.KaplanN,WickiewiczTL,WarrenRF.Primarysurgical treatmentofanteriorcruciateligamentruptures.Along-term follow-upstudy.AmJSportsMed.1990;18(4):354–8.
14.KocherMS,SteadmanJR,BriggsKK,SterettKK,HawkinsRJ. Relationshipsbetweenobjectiveassessmentofligament stabilityandsubjectiveassessmentofsymptomsand functionafteranteriorcruciateligamentreconstruction.AmJ SportsMed.2004;32(3):629–34.
15.LeitzeZ,LoseeRE,JoklP,JohnsonTR,FeaginJA.Implications ofthepivotshiftintheACL-deficientknee.ClinOrthopRelat Res.2005;(436):229–36.
16.KatzJW,FingerothRJ.Thediagnosticaccuracyofrupturesof theanteriorcruciateligamentcomparingtheLachmantest, theanteriordrawersign,andthepivotshifttestinacuteand chronickneeinjuries.AmJSportsMed.1986;14(1):88–91. 17.BenjaminseA,GokelerA,vanderSchansCP.Clinical
diagnosisofananteriorcruciateligamentrupture:a meta-analysis.JOrthopSportsPhysTher.2006;36(5):267–88. 18.BachBRJr,WarrenRF,WickiewiczTL.Thepivotshift
phenomenon:resultsanddescriptionofamodifiedclinical testforanteriorcruciateligamentinsufficiency.AmJSports Med.1988;16(6):571–6.
19.GalwayHR,MacIntoshDL.Thelateralpivotshift:asymptom andsignofanteriorcruciateligamentinsufficiency.Clin OrthopRelatRes.1980;(147):45–50.
20.MusahlV,VoosJ,O’LoughlinPF,StueberV,KendoffD,Pearle AD.Mechanizedpivotshifttestachievesgreateraccuracy thanmanualpivotshifttest.KneeSurgSportsTraumatol Arthrosc.2010;18(9):1208–13.
21.KocherMS,SteadmanJR,BriggsKK,SterettWI,HawkinsRJ. Relationshipsbetweenobjectiveassessmentofligament stabilityandsubjectiveassessmentofsymptomsand functionafteranteriorcruciateligamentreconstruction.AmJ SportsMed.2004;32(3):629–34.
22.PlaweskiS,CazalJ,RosellP,MerlozP.Anteriorcruciate ligamentreconstructionusingnavigation:acomparative studyon60patients.AmJSportsMed.2006;34(4):542–52. 23.SieboldR,DehlerC,EllertT.Prospectiverandomized
comparisonofdouble-bundleversussingle-bundleanterior cruciateligamentreconstruction.Arthroscopy.
2008;24(2):137–45.
24.BediA,MaakT,MusahlV,O’LoughlinP,ChoiD,CitakM,etal. Effectoftunnelpositionandgraftsizeinsingle-bundle anteriorcruciateligamentreconstruction:anevaluationof time-zerokneestability.Arthroscopy.2011;27(11):1543–51. 25.DriscollMD,IsabellJrGP,CondittMA,IsmailySK,JupiterDC,
NoblePC,etal.Comparisonof2femoraltunnellocationsin anatomicsingle-bundleanteriorcruciateligament
reconstruction:abiomechanicalstudy.Arthroscopy. 2012;28(10):1481–9.
26.BediA,MusahlV,O’LoughlinP,MaakT,CitakM,DixonP,etal. Acomparisonoftheeffectofcentralanatomical
single-bundleanteriorcruciateligamentreconstructionand double-bundleanteriorcruciateligamentreconstructionon pivot-shiftkinematics.AmJSportsMed.2010;38(9):1788–94. 27.BullAMJ,AmisAA.Thepivot-shiftphenomenon:aclinical
andbiomechanicalperspective.Knee.1998;5(3):141–58. 28.PearleAD,SolomonDJ,WanichT,Moreau-GaudryA,Granchi
CC,WickiewiczTL,etal.Reliabilityofnavigatedkneestability examination:acadavericevaluation.AmJSportsMed. 2007;35(8):1315–20.
29.KopfS,ForsytheB,WongAK,TashmanS,IrrgangJJ,FuFH. TranstibialACLreconstructiontechniquefailstopositiondrill tunnelsanatomicallyinvivo3DCTstudy.KneeSurgSports TraumatolArthrosc.2012;20(11):2200–7.
30.IwahashiT,ShinoK,NakataK,OtsuboH,SuzukiT,AmanoH, etal.Directanteriorcruciateligamentinsertiontothefemur assessedbyhistologyand3-dimensionalvolume-rendered computedtomography.Arthroscopy.2010;26Suppl.9:S13–20. 31.BullAM,EarnshawPH,SmithA,KatchburianMV,HassanAN, AmisAA.Intraoperativemeasurementofkneekinematicsin reconstructionoftheanteriorcruciateligament.JBoneJoint SurgBr.2002;84(7):1075–81.