rev bras reumatol.2015;55(2):185–188
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
Parvovirus
B19
infection
as
a
cause
of
acute
myositis
in
an
adult
Mustafa
Cakirca
a,
Cumali
Karatoprak
a,
Serdal
Ugurlu
b,∗,
Mehmet
Zorlu
a,
Muharrem
Kıskac¸
a,
Güven
C¸
etin
caDepartmentofInternalMedicine,MedicalFaculty,BezmialemVakifUniversity,Istanbul,Turkey
bDivisionofRheumatology,DepartmentofInternalMedicine,CerrahpasaMedicalFaculty,UniversityofIstanbul,Istanbul,Turkey
cDivisionofHematology,DepartmentofInternalMedicine,MedicalFaculty,BezmialemVakifUniversity,Istanbul,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19January2013 Accepted23June2013
Availableonline26November2014
Keywords: ParvovirusB19 Acuteadultmyositis Fever
a
b
s
t
r
a
c
t
ParvovirusB19infectionisoftenasymptomatic,butclinicalexpressionsmayinclude tran-sientaplasticcrisis,erythemainfectiosum,non-immunehydropsfetalis,andchronicred cellaplasia.Thisvirushasalsobeenassociatedwithrheumatoidarthritisandother autoim-muneconnectivetissuediseases;however,wecouldnotidentifyanyacuteadultmyositis casedevelopedafteraParvovirusB19infectionintheliterature.Forthisreason,wewould liketopresentararecaseofacutemyositisdevelopedafterParvovirusB19infection.In patientspresentingwithsymptomsoffever,rashonthelegsandmyositis,viralinfections suchasParvovirusB19shouldbekeptinmind.
©2014ElsevierEditoraLtda.Allrightsreserved.
Infecc¸ão
por
parvovírus
B19
como
causa
de
miosite
aguda
em
um
adulto
Palavras-chave: ParvovírusB19
Miositeagudadoadulto Febre
r
e
s
u
m
o
A infecc¸ão pelo ParvovírusB19costuma serassintomática,mas asexpressões clínicas podemincluircriseaplásticatransitória,eritemainfeccioso,hidropisiafetalnãoimunee aplasiacrônicadasérievermelha.Essevírustambémseassociaàartritereumatoideea outrasdoenc¸asautoimunesdotecidoconjuntivo;entretanto,nãoconseguimosidentificar naliteraturanenhumcasodemiositeagudaemadultodesenvolvidadepoisdeinfecc¸ãopelo ParvovírusB19.Poressarazão,gostaríamosdeapresentarumcasorarodemiositeaguda desenvolvidadepoisdeinfecc¸ãopeloParvovírusB19.Nospacientesqueapresentam sin-tomasdefebre,rashnaspernasemiosite,devemserconsideradasasinfecc¸õesvirais,como acausadapeloParvovírusB19.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
∗ Correspondingauthor.
E-mail:[email protected](S.Ugurlu). http://dx.doi.org/10.1016/j.rbre.2014.10.001
186
rev bras reumatol.2015;55(2):185–188Introduction
ParvovirusB19(B19),anon-enveloped22–26nmicosahedral single-stranded DNA virus discovered in 1975, is the only memberofthefamilyParvoviridaeknowntobepathogenic tohumans.1Thisinfectiousdiseaseisgenerallyseenduring childhood, but rarely in adults. Infection appears to con-ferlifelongimmunityinimmunocompetenthosts.Although theseroprevalenceishigh,viremiaorpresenceofviralDNA in peripheral blood is rare in healthy individuals.2 B19 is transmittedthrough the respiratory route, but can also be transmittedvertically from mother to fetus,through bone marrowandorgantransplantations,andviatransfusedblood products.2MostcasesofB19infectionsareasymptomaticand resolvespontaneouslyinadults.ButsometimesB19causesa transientaplasticcrisis,erythema-infectiosum(fifthdisease), non-immunehydropsfetalisandchronicredcellaplasia.This virushasalsobeenassociatedwithrheumatoidarthritisand otherautoimmuneconnectivetissuediseases;3however,we couldnotidentifyanyacuteadultmyositiscasesdeveloped afterB19infection.Intheliterature,forthatreason,wewould liketopresentararecaseofacutemyositisdevelopedafter B19infection.
Case
report
A 38-year-old male patient was admitted to the internal medicinepolyclinicwithcomplaintsofhighfeverandmalaise. These,plusdiffusepain,hadstarted3daysbeforeandbecame increasinglysevere.Hehadnohistoryofdiseasesormedicine use.Inthephysicalexamination,hisauxiliarybody tempera-turewas39◦C,andothersystemicexaminationswerenormal.
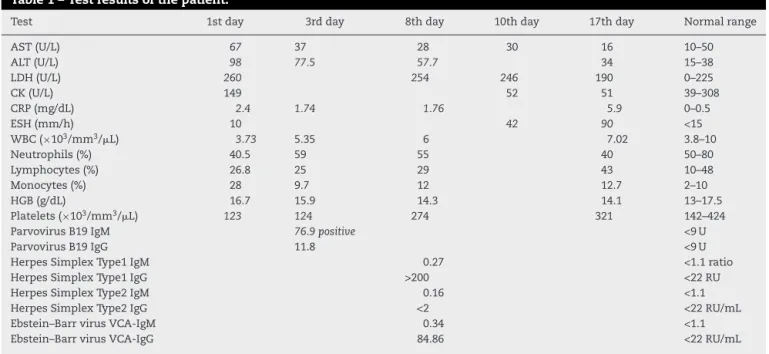
The laboratory tests revealed increased levels of alanine aminotransferase (ALT), aspartate aminotransferase (AST), andC-reactiveprotein(CRP).Leukopenia,thrombocytopenia, and monocytosis were foundinhishemogram(Table1).A slight increase in monocytes was found in his peripheral bloodsmear.Bloodculturetakenduringhishighfeverperiod showednogrowth.Heterophileantibody(monospot)was neg-ative.
Maculopapularrashesdevelopedunderbothkneesbuthis fever decreased within the next 2 days. B19 antibodyIgM testedpositive,andthusB19wasconsideredtobethecause oftherashes.Onthethirddayofthedisease,arthralgia devel-opedinbothankles,andalsoinbothhands.Onthesixthday, therashesremitted,replacedbypaininbothcalvessosevere thatitpreventedhimfromwalking.
Intheinvestigationsperformedforthefollow-up,AST,ALT and creatinekinase (CK) were found to havedecreased to withinnormalranges,butCRPanderythrocytesedimentation rates (ESH)had increased(Table 1). Thepatient was hospi-talized,andnaproxensodium1100mg/daywasinitiated.The bilateralcrurisMRItakenduetocontinuingseverepainonhis bilateralcalfmusclesrevealedthickeningandedemainboth gastrocnemiusandthesemimembranosusmusclegroup,an increasedsignalinT2,and anedematousappearance.The minimalcontrastinvolvementinthepost-contrastserieswas consideredtobemyositis(Fig.1).Follow-uponthe10thday ofthetreatmentrevealedreducedpain,andESHandCRPhad returnedtowithintheirnormalranges.
Discussion
B19iscommonworldwide,andtheseroprevalenceincreases withage,sothat15%ofpreschoolchildren,50%ofyounger
Table1–Testresultsofthepatient.
Test 1stday 3rdday 8thday 10thday 17thday Normalrange
AST(U/L) 67 37 28 30 16 10–50
ALT(U/L) 98 77.5 57.7 34 15–38
LDH(U/L) 260 254 246 190 0–225
CK(U/L) 149 52 51 39–308
CRP(mg/dL) 2.4 1.74 1.76 5.9 0–0.5
ESH(mm/h) 10 42 90 <15
WBC(×103/mm3/L) 3.73 5.35 6 7.02 3.8–10
Neutrophils(%) 40.5 59 55 40 50–80
Lymphocytes(%) 26.8 25 29 43 10–48
Monocytes(%) 28 9.7 12 12.7 2–10
HGB(g/dL) 16.7 15.9 14.3 14.1 13–17.5
Platelets(×103/mm3/L) 123 124 274 321 142–424
ParvovirusB19IgM 76.9positive <9U
ParvovirusB19IgG 11.8 <9U
HerpesSimplexType1IgM 0.27 <1.1ratio
HerpesSimplexType1IgG >200 <22RU
HerpesSimplexType2IgM 0.16 <1.1
HerpesSimplexType2IgG <2 <22RU/mL
Ebstein–BarrvirusVCA-IgM 0.34 <1.1
Ebstein–BarrvirusVCA-IgG 84.86 <22RU/mL
rev bras reumatol.2015;55(2):185–188
187
Fig.1–Bothlowerlimbs’MRIimagesofthepatient.
adultsandabout85%oftheelderlyshowserologicevidence ofpastinfection.2 Thisinfectiousdisease isgenerallyseen duringchildhood,but rarelyinadults.Laboratorydiagnosis of B19 can be performed using serology, PCR, histopatho-logicexaminationandimmunohistochemistry.2Theprecise diagnosis ofrecent or past infection with B19 dependson the use of enzyme immunoassays to detect anti-B19 IgM and IgG in plasma. To confirm acute B19 infection, IgM antibodiesmustbedetectedinplasmaorserum.These anti-bodies are synthesized approximately 7–10 days after the high-titer viremia.4 B19 IgG appears shortly after IgM and persistslifelongwithslowlydecreasingtitersunlessboosted bysubsequent encounters withthe virus. Theclinical sig-nificance of different serum-titers ofB19 DNA is not fully established. In healthy individuals with acute B19 infec-tion, viral titers as high as 1012gEq/mL are detectable in blood.3,4
Benignacutemyositisisaself-recovering[benign] condi-tioncharacterizedbyacutebilateralcalf painanddifficulty inwalkingthatusuallydevelopsinschool-agechildrenafter theyhaverecoveredfromviralinfections.Itwasfirst recog-nizedin1957byLundbergin74pediatricsubjects.5,6Myositis casescoincidewithdermatomyositisandsystemiclupus ery-thematosusafterParvovirusB19infectioninadults.7Although themostcommonviralcausesofacutemyositisareInfluenza A,B(including theH1N1 virus)and Coxsackievirusviruses inchildren,nocasereportwasfoundaboutB19associated with benign acute childhood myositis.8 However, there is onecase report about myofacitis associatedwith B19 in a healthyadult.9 But, toour knowledge,literaturereportsno casesaboutmyositisassociatedwithB19inanadult.Aswe knowB19infectionoccursespeciallyintransplantpatients, patients withsystemic diseases and immunocompromised patients.4 Inourcase,althoughtherewasnohistory of ill-nessanddrugintake,historyofintensepaceofwork,intense stress and a 12-h trip might have a negative impact on immuneresistanceandmaycausemyositisassociatedwith B19.
Inourpatient,clinicalandlaboratoryfindings,magnetic resonance imaging and response to therapy support the diagnosis of acute myositis. The expected increased sedi-mentationand CRPwere found;however, theCKlevel had not increasedinour patient. Theabsence ofincreasedCK levels mayleadtoconfusion.From thepatient’s laboratory follow-up,wecouldseethatCKlevelwasthreetimeshigher inthefirstperiod.ButCKlevelwasnormalineveryperiod of the disease.Although most patients withinflammatory myopathies present with increased creatine kinase levels, reportedseriesincludesomepatientswithnormalcreatine kinaselevels.9–11Inthesecases,eventhoughmyopathywas diagnosed by methods such as biopsy and MRI, CK levels were normal. Andconcrete evidencewas notsubmittedto explainthissituation.Inanarticlepresentingsevenpatients withmyositis,alackofcreatinekinaseelevationinpatients withmyositiswasfoundtobeapoorprognosticsign.10Our case had a benign course and clinical findings improved quickly.
Despitethesimilaritywithchildhoodbenignacute myosi-tis cases,ourcasewasthoughttobeinterestingbecause it wasinanadultwithnoincreasedCKlevel.Inpatientswho present withfever,rashon thelegs, andmyositis(such as inourcase),viral infectionssuchasB19shouldbekeptin mind.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
TheauthorsthankS.Delecroixfortranslationconsultancy.
r
e
f
e
r
e
n
c
e
s
1.CrowsonAN,MagroCM,DawoodMR.Acausalrolefor parvovirusB19infectioninadultdermatomyositisandother autoimmunesyndromes.JCutanPathol.2000;27:
505–15.
2.TolfvenstamT,BrolidenK.ParvovirusB19infection.Semin FetalNeonatalMed.2009;14:218–21.
3.KerrJR.PathogenesisofhumanparvovirusB19inrheumatic disease.AnnRheumDis.2000;59:
672–83.
4.SlavovSN,KashimaS,PintoACS,CovasDT.Human parvovirusB19:generalconsiderationsandimpacton patientswithsickle-celldiseaseandthalassemiaandon bloodtransfusions.FEMSImmunolMedMicrobiol. 2011;62:247–62.
5.LundbergA.Myalgiacrurisepidemica.ActaPaediatrScand. 1957;46:18–31.
6.MackayMT,KornbergAJ,ShieldLK,DennettX.Benignacute childhoodmyositis:laboratoryandclinicalfeatures. Neurology.1999;53:2127–31.
7.KalishRA,KnopfAN,GaryGW,CanosoJJ.Lupus-like
188
rev bras reumatol.2015;55(2):185–1888. KoliouM,HadjiloizouS,OuraniS,DemosthenousA,
HadjidemetriouA.Acaseofbenignacutechildhoodmyositis associatedwithinfluenzaA(H1N1)virusinfection.Clin MicrobiolInfect.2010;16:193–5.
9. IchinoseK,MigitaK,SekitaT,HamadaH,EzakiH,Mukoubara S,etal.ParvovirusB19infectionandmyofasciitis.Clin Rheumatol.2004;23:184–5.
10.FudmanEJ,SchnitzerTJ.Dermatomyositiswithoutcreatine kinaseelevation.Apoorprognosticsign.AmJMed. 1986;80:329–32.