w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Kinesiotherapy
effect
on
quality
of
life,
sexual
function
and
climacteric
symptoms
in
women
with
fibromyalgia
夽
Lilian
Lira
Lisboa
a,b,c,∗,
Elisa
Sonehara
c,
Katia
Cristina
Araújo
Nogueira
de
Oliveira
a,d,
Sandra
Cristina
de
Andrade
b,c,
George
Dantas
Azevedo
a,eaPostgraduatePrograminHealthSciences,UniversidadeFederaldoRioGrandedoNorte,Natal,RN,Brazil
bDepartmentofPhysicalTherapy,UniversidadeFederaldoRioGrandedoNorte,Natal,RN,Brazil
cCourseofPhysicalTherapy,UniversidadePotiguar(LaureateInternationalUniversities),Natal,RN,Brazil
dDepartmentofTocogynecology,UniversidadeFederaldoRioGrandedoNorte,Natal,RN,Brazil
eDepartmentofMorphology,UniversidadeFederaldoRioGrandedoNorte,Natal,RN,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15May2014 Accepted26August2014 Availableonline13May2015
Keywords:
Fibromyalgia Qualityoflife Sexuality Sexualapproach Climacteric
a
b
s
t
r
a
c
t
Objective:Toevaluatetheeffectofthekinesiotherapyinthequalityoflife,sexualfunction andmenopause-relatedsymptomsandcompareinclimactericwomenwithandwithout fibromyalgia(FM).
Methodology:Thegroupwascomposedof90climactericwomendividedin2groups:FM(47) andcontrol(43).Thepatientswereanalyzedontheirqualityoflife(UtianQualityofLife [UQoL]),sexualfunction(SexualQuotient-FemaleVersion[SQ-F]questionnaire)and inten-sityoftheclimactericsymptoms(Blatt–Kuppermanmenopausalindex[BKMI]).Bothgroups performedpelvicfloorkinesiotherapy,composedof20sessions,twiceaweek.Statistical analysiswasperformedusingStudent’st-test,mixed-designanalysisofvariance(ANOVA) andCohen’sKappa.
Results:Inthequalityoflife,animprovementwasnoticedinbothgroupsforalldomains analyzed.Inthecomparisonbetweengroupsitwasnoticedadifferenceintheemotional (p=0.01),health(p=0.03)andsexual(p=0.001)domainswithconsiderablegainsverifiedin thecontrolgroup.Improvementwasalsonoticedinthesexualfunction.Intheanalysis betweengroups,FMgroupshowedalowerscorecomparedtothecontrolgroup(p<0.001). Withrespecttotheclimactericsymptoms,therewasnodifferenceintheanalysisbetween groupsaftertheintervention(p<0.001).
Conclusions: Thepelvicfloorkinesiotherapypromotesapositiveeffectinthedomainsof qualityoflife, sexualfunctionandclimacteric symptomsinwomen withand without
夽
WorkconductedatthePostgraduatePrograminHealthSciences,UniversidadeFederaldoRioGrandedoNorte,andatUniversidade Potiguar(LaureateInternationalUniversities),Natal,RN,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.L.Lisboa).
http://dx.doi.org/10.1016/j.rbre.2014.08.018
fibromyalgiaintheclimactericperiod;however,fibromyalgiaseemstobealimitingfactor toachievebetterresultsinsomeoftheaspectsevaluated.
©2015ElsevierEditoraLtda.Allrightsreserved.
Efeito
da
cinesioterapia
na
qualidade
de
vida,
func¸ão
sexual
e
sintomas
climatéricos
em
mulheres
com
fibromialgia
Palavras-chave:
Fibromialgia Qualidadedevida Sexualidade Abordagemsexual Climatério
r
e
s
u
m
o
Objetivo: Avaliarecompararoefeitodacinesioterapianaqualidadedevida,func¸ãosexual esintomasclimatéricosemmulheresclimatéricascomesemfibromialgia.
Métodos: Participaram90mulheresclimatéricas,divididasemdoisgrupos:fibromialgia(47) econtrole(43).Aspacientesforamavaliadasnasvariáveis:qualidadedevida(UtianQuality ofLife[UQOL]),func¸ãosexual(questionáriodoquocientesexual/versãofeminina[QS-F])e intensidadedossintomasclimatérios(ÍndiceMenopausaldeBlatt–Kupperman[IMBK]).Os gruposfizeramcinesioterapiaparaoassoalhopélvico,compostode20sessões,duasvezes porsemana.AnáliseestatísticafoifeitapormeiodostestestdeStudentpareado,análise devariânciadedelineamentomistoeKappadeCohen.
Resultados: Naqualidadedevida,foiobservadamelhoriaemambososgruposparatodos osdomíniosavaliados.Naanáliseintergrupofoievidenciadadiferenc¸anosdomínios emo-cional(p=0,01),saúde(0,03)esexual(p=0,001)comganhosmaisexpressivosparaogrupo controle.Nafunc¸ãosexual,foiverificadamelhorianosgrupos,apósaintervenc¸ão;naanálise intergrupoasfibromiálgicasapresentaramescoresinferioresaogrupocontrole(p<0,001). Emrelac¸ão aossintomasclimatéricos não houvediferenc¸ana análiseintergrupo pós-intervenc¸ão(p=0,73).Entretanto,ambososgruposapresentaramreduc¸ãosignificativada sintomatologiaapósaintervenc¸ão(p<0,001).
Conclusões: Acinesioterapiadoassoalhopélvicoexerceefeitobenéficosobreosdomínios daqualidadedevida,func¸ãosexualesintomatologiaclimatéricaemmulherescomesem fibromialgianafasedoclimatério.Entretanto,afibromialgiapareceserfatorlimitantepara melhoresresultadosemalgunsaspectosavaliados.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Fibromyalgiaisoneofthemostcommonrheumaticdiseases, whosemaincharacteristicisadiffuseand chronic muscu-loskeletalpain.1,2Inadditiontothepainfulcondition,patients
oftencomplainoffatigue,sleepdisturbances,morning stiff-ness, paresthesias of the extremities, a subjective feeling ofedema, cognitivedisorders,urogynecology disordersand decreased libido. Although the etiology and pathogenesis offibromyalgiaisnotfullyunderstood,itisrecognizedasa complex and heterogeneous clinical entity, depending not onlyofbiologicalmechanismsbutalsoofinfluencesofthe psychosocial context.3,4 The diagnosis remains a complex
challenge for clinicians, by covering a variety of aspects, including thefact thatit isbased solelyon the perception ofsymptomsbythepatient,absenceofanobjectivetestto confirmordenythediagnosisandtheunpredictableresponse to various existing treatments. What is known is that, in mostpatients,thepainandsymptomsassociateddetermine anegativeimpactonqualityoflife.3
Studies have reported that about 80–0% of cases of fibromyalgia occur in the female population4,5 and that
women exhibit significantly more symptoms than men.6
Consideringthatthehighestprevalenceofthediseaseoccurs between50and65yearsofage,7,8 whichcoincideswiththe
climactericperiod,somesignsandsymptomsof fibromyal-giacanoftenbeconfusedwithmenopause-relatedsymptoms. Therefore, it is common that many patients initially seek medical carewith generalist physiciansand gynecologists, whichreinforcestheimportanceofinvestigatingthe associa-tionbetweenmenopauseandfibromyalgia.9,10
Studies examiningthis association havesuggested that those hormonal disturbances of the menopause may be directlyinvolvedinthegenesisofsymptomsassociatedwith fibromyalgiainmiddle-agedwomen.10However,considering
thattherearewomenwithfibromyalgiaoutsidethe climac-tericphase,itisclearthatthehormonaldeficitisnottheonly pathophysiologicalmechanisminvolvedinthegenesisofthis disease.10,11
aimed to analyze the effect of pelvic floor kinesiotherapy in menopause related symptoms, quality of life and sex-ualfunctioninwomenwithfibromyalgiaintheclimacteric period.
Methods
Aclinicaltrialinvolving90climactericwomenagedbetween 45 and 65 years, regardless ofrace, ethnicity and religion, wasconducted. Thewomenwere referred from outpatient clinics for menopause care (Centro de Saúde Reprodu-tiva Leide Morais and Maternidade Escola Januário Cicco; Natal,RN)andrheumatology (HospitalUniversitárioOnofre Lopes, Universidade Federal do Rio Grande do Norte and Clínica Integrada da Saúde, Universidade Potiguar; Natal, RN)afteraninitialscreening.Thestudy wasreviewedand approvedbytheResearch EthicsCommitteeofthe Univer-sidadePotiguar undertheprotocol number250/2010, CAAE 0252.0.052.000-10.All participantssignedanInformed Con-sentForm,accordingtothenormsoftheConselhoNacional deSaúde,Resolution196/1996.Theresearchwasconducted inaccordancewiththeDeclarationofHelsinki,asrevisedin 2008.
Consideringthat thestudy designinvolves estimates of frequenciesandmeanscores,samplingtechniqueswith sta-tisticalprocedureswere used,adoptinganalphaof5%and astatisticalpowerof80%.Takingintoconsiderationalsothe designeffectandtheoccurrenceofrefusalsandlosses,itwas decidedtoincreasethesamplesizetobuildinamarginof safetyforpossiblesamplelosses.
Thevolunteersweredividedintotwogroups:fibromyalgia (FM)(n=47)andcontrol(n=43)groups.Thefollowing inclu-sioncriteriawereconsideredforFMgroup:(a)adiagnosisof FMestablishedbyarheumatologist,accordingtothe Ameri-canCollegeofRheumatology(ACR)1990criteria2;(b)cognitive
abilitytounderstandthepurposeofthesurveyandtoanswer the questionnaires; (c) not to be performing, at least dur-ingonemonth,anytypeofphysicaltherapy.Forthecontrol group,all inclusion criteria above mentioned were obeyed, withtheexclusionofdiagnosisofFM.Exclusioncriteriafor bothgroupsincluded:(a)presenceofphysicallimitations;(b) previoushistoryofoophorectomy;(c)presenceofdiffuse con-nectivetissuediseases,chronicpelvicpainandirritablebowel syndrome.
The volunteers were subjected to pre- and post-interventionassessmentsthroughquestionnairesappliedby evaluatorstrainedinapplyingtheresearchtools,individually andinareservedplace.Allassessmentswereblinded,being carriedoutbyevaluatorsdifferentofthose whounderwent the physical therapy intervention. As for data collection, the authors usedasemistructured questionnairetoassess the demographic characteristics (age, years of education, occupation, householdincomeand maritalstatus), besides validatedinstrumentstomeasurequalityoflifespecifically duringmenopause,climactericsignsandsymptoms’severity andsexualfunction.
ThequalityoflifewasassessedbytheUtian Qualityof Life(UQoL)questionnaire,translatedandvalidatedinBrazilby Galvãoetal.(2007),12whichprovedtobeausefulinstrumentto
quantifyquality-of-lifeandwell-beingsubjectiveassessments inpre-and post-menopausalwomen. Theinstrument con-tains23questionsthatcomprisefourdistinctquality-of-life domains,namely:occupational,health,sexualandemotional domain.EachquestionofUQoLisansweredbymeansofa5 pointscale,whereinthemaximumandminimumvaluesvary ineachdomain.Thehighertheawardedscore,thebetterthe qualityoflife.
Theseverity ofclimactericsymptoms was measuredby Blatt–KuppermanMenopausalIndex(BKMI),13aninstrument
widelyusedbothinclinicalpracticeandinresearchsettings to monitortheeffects ofthose varioustreatments usedin theclimactericphase,demonstratinghightest–retest reliabil-ity power.BKMIconsistsof11items, forwhich thepatient attributesscoresaccordingtotheintensityofeachsymptom (0–none,1–mild,2–moderate,3–severe).Thefinalscoreis determinedbythesumoftherespectivescoresoftheabove symptoms,aftertheirmultiplicationbyconversionfactors,in ordertomeasurequantitativelytheintensityofclimacteric symptoms.
Theparticipants’sexualfunctionwasassessedbythe Sex-ualQuotientfemaleversionquestionnaire(SQ-F),developed and validated for the Portuguese idiom by Abdo (2006).14
Thistoolcontains questionsaboutvariousdomainsof sex-ual activityforwomen(sexualdesire,arousal,orgasm,and theirpsychophysicalcorrelates)scoredfrom0to100,where thecloserto100,thebetterthesexualfunction.
After the pre-intervention assessment, all participants initiated the proposed treatment, which wasperformed in 10 consecutive weeks,involving 20 sessions ofpelvic floor kinesiotherapy held twice a week, with 1-h/day duration, conductedbyoneoftheresearchers.Theproposedconduct obeyedthesequenceofperception,abdominoperineal dissoci-ation,voluntarycontractionandautomationofthepelvicfloor associatedwithfacilitatingpostures,pelvismobilizationand breathingtrainingatthetimeofpelvicfloorcontractions.Each exercisewasperformedwithaseriesoftenrepetitions;each contraction wassustainedfor5s,with10sofrestbetween contractions,progressingtoa10-ssupportwith20sofrest after10sessions.
Afterfinishingtheinterventionperiod,thepatientswere reassessed,usingthesamesurveyinstrumentsappliedinthe pre-interventionperiod.
with the statistical software Statistical Package for Social Science(SPSS)version20.0,andasignificancelevelof5%was adopted.
Results
Ofthe90womenselectedforthestudy,sevendroppedout duringtheinterventionordidnotperform80%ofthesessions (threeinthecontrolgroupandfourinFMgroup).Thealleged reasonsforwithdrawalwererelatedtopersonalreasonsandto incompatibilityoftime;thus,noadverseeventwasindicated asthecauseoftheinterruption.
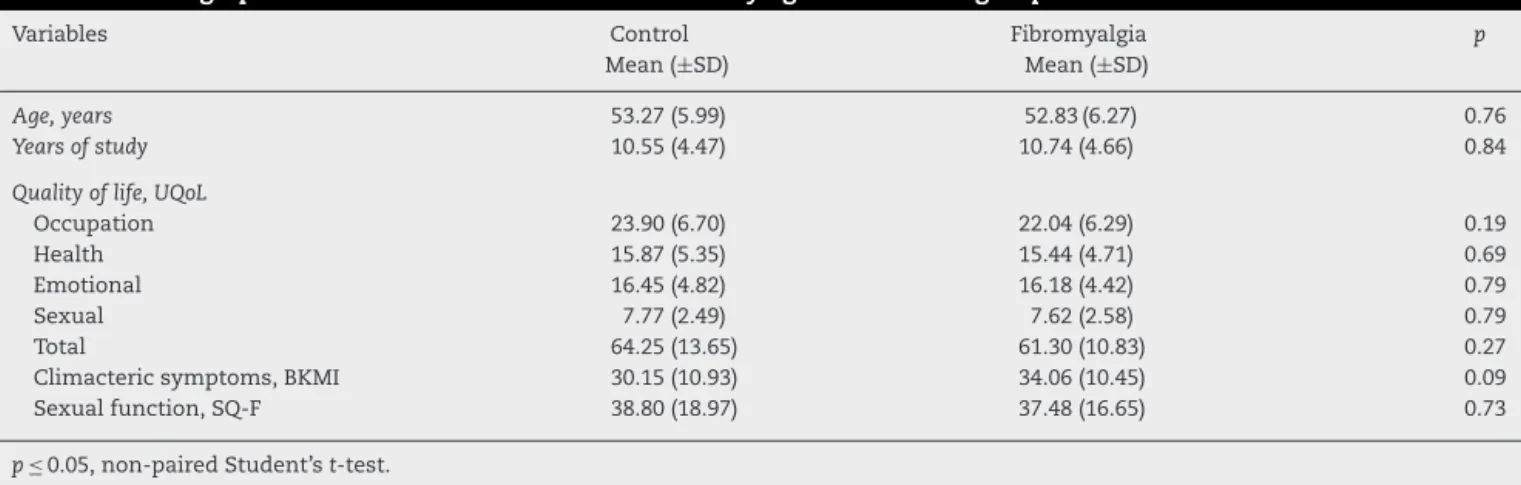
Atotalof83 participantscompletedthestudy,ofwhich 43werepartofFMgroupand40wereinthecontrolgroup. Withregardtodemographics,therewasnostatistically sig-nificantdifferencebetweengroupsatbaseline.Regardingthe variablesmaritalstatus,occupationandincome,nodifference wasobservedbetweengroups (p>0.05)and inthis sample, ingeneral,62 (74.7%)participantshad asteadypartner,43 (51.8%)exertedsomeoff-homeworkand43(51.8%)hada fam-ilyincomebetween2and4minimumwages.InTable1itcan beseenthatthegroupswerehomogeneousinallcontinuous variablesinvestigatedpreviouslytothetreatmentproposed inthestudy.Afterthestudyperiod,noadverseeventswere reported,andmostpatientsshowedsatisfactionwiththe pro-posedexercises.
RegardingthedomainsofqualityoflifeanalyzedbyUQoL, it wasobservedthat thekinesiotherapy protocol alloweda statisticallysignificantimprovementforbothFMandcontrol groups in all domains, when comparing pre- and post-interventionintragroupresults.Regardingtheeffectorclinical impactoftheinterventiononthedomainsofqualityoflife, itcanbeobservedthat,fortheclimactericgroup,alldomains ofUQoLshowedastrongeffect:physical(d=0.72),emotional (d=1.02), health(d=1.49)andsexual(d=1.69),andthis also occurredwiththeFMgroup:occupational(d=0.62),emotional (d=0.62), health(d=0.97) and sexual (d=1.00). In the post-interventionintergroupevaluation,astatisticallysignificant differencewasobservedinthreeofthefourUQoLdomains: occupational(p=0.01), health(p=0.03)and sexual(p≤0.00), andkinesiotherapyprovidedbetterresultsinwomeninthe controlgroup(Table2).
Intheevaluationofsexualfunction,itcanbeobservedin
Table3that,aftertheintervention,bothFM(37.48vs.43.34,
p<0.001,d=0.36)andcontrol(38.80vs.50.67,p<0.001,d=0.67) groupshad theirscoresincreased,withstatistically signifi-cantdifferences.Aweakclinicalimpactoftheintervention forFMgroupandastrongimpactforthecontrolgroupwere identified. In intergroup comparison, a statistically signifi-cantdifference(p=0.01)wasdetected,evidencingamoreclear improvementinthecontrolgroup.
By analyzing the intensity ofmenopause-related symp-toms by BKMI, it is observed in Table 3 that the protocol for pelvic floor kinesiotherapy resulted in a significant scorereduction forbothFM (34.06vs. 23.23; pre-vs. post-intervention,respectively,p<0.001,d=1.09)andcontrol(30.15 vs. 19.20, p<0.001, d=1.08) groups, with a strong clini-cal impact ofthe intervention for both groups. As forthe
intergroupanalysis,therewasnostatisticallysignificant dif-ferencebetweengroups(p=0.73).
Discussion
Ourfindingsdemonstratethatpelvicfloorkinesiotherapyin climactericwomencanimprove theirqualityoflife,sexual functionandclimactericsymptoms.Despitetheveryfrequent complaintsofsexualdysfunction,menopause relatedsigns and symptomsandanegativeimpactonthequalityoflife inwomenwithfibromyalgia,15–20 anddespiteprevious
stud-iesshowingpositiveeffectsofpelvicfloorkinesiotherapyfor thesecomplaints,21,22todatetherewerenoreportsinthe
liter-atureontheuseofthisinterventionaspartofthetreatmentof suchdisordersconsideringthisparticulargroupofclimacteric women.Thus,thisisthefirstreportintheliteraturepointing out thattheclinicalimpactofpelvicfloorkinesiotherapyis differentinwomenwithanassociateddiagnosisof fibromyal-gia,whichmayhaveimportantimplicationsfortheclinical managementofthesepatients.
Regarding the domains of quality of life, a significant improvement in both groups was demonstrated after the pelvic floor kinesiotherapy sessions, which corroborates the results of previous studies demonstrating that such physicaltherapy interventionprovides significant improve-ment inqualityoflifeofwomen withdysfunctionalpelvic floor.21–23ArecentstudyinNigerianwomenintheclimacteric
phase, which aimed to investigate the effect of a twelve-weekprogramofphysicalexercisesand pelvicfloormuscle strengthening,showedthattheinterventionledtoa signifi-cantimprovementonqualityoflifeingeneral.24
Althoughfibromyalgiaisdirectlylinkedtoemotionaland psychologicaldisorders,25theclimactericperiod,byitself,is
adifficulttransitionphase,whichinvolvesacomplexprocess ofemotionalandbodilychanges,beingundertheinfluenceof multiplefactorssuchaspersonalandfamilylifehistory, envi-ronment,culture,customsand personalpeculiarities.Such aspectsresonatedifferentlyineachwoman,withdirect inter-ference in their feelings and quality of life,26 a fact that
resemblesandoftendefinesthesymptomsofmenopauseas beingpartoffibromyalgia.10
Intheanalyzedsample,FMgroupshowedlimitationsin the kinesiotherapeutic resultsin relationto “occupational” and“health”domainsofqualityoflife.Suchlimitationswere evidencedinanotherstudy27whichproposedtoanalyzethe
difficulty ofa continuous work forwomenwith fibromyal-gia;theauthorsobservedthatlimitationsinphysicalcapacity andtheincreasedneedforrest,duetothechronicityofthe painprocess,werethemainreasonsassociatedwiththe dif-ficultytomanagephysical,psychosocialandorganizational workdemands.Itisalsoknownthatfibromyalgiais charac-terizedbybeingapersistentanddebilitatingdisorder,causing anegativeeffectonpeople’slivesandaffectingtheirability toworkandengageindailyactivities.28,29Theseeffectsarise
Table1–Demographicandclinicalcharacteristicsoffibromyalgiaandcontrolgroupsatbaseline.
Variables Control
Mean(±SD)
Fibromyalgia Mean(±SD)
p
Age,years 53.27(5.99) 52.83(6.27) 0.76
Yearsofstudy 10.55(4.47) 10.74(4.66) 0.84
Qualityoflife,UQoL
Occupation 23.90(6.70) 22.04(6.29) 0.19
Health 15.87(5.35) 15.44(4.71) 0.69
Emotional 16.45(4.82) 16.18(4.42) 0.79
Sexual 7.77(2.49) 7.62(2.58) 0.79
Total 64.25(13.65) 61.30(10.83) 0.27
Climactericsymptoms,BKMI 30.15(10.93) 34.06(10.45) 0.09
Sexualfunction,SQ-F 38.80(18.97) 37.48(16.65) 0.73
p≤0.05,non-pairedStudent’st-test.
Table2–Analysisofintragroupandintergroupqualityoflife,consideringpre-andpost-interventionperiods.
Variables Control Fibromyalgia Intergroup
difference,P
Pre Post Intragroup
difference,p
Pre Post Intragroup
difference,p
Mean(±SD) Mean(±SD) Mean(±SD) Mean(±SD)
UQoLemotional 16.45(±4.82) 21.02(±4.12) <0.00a,b 16.18(±4.42) 18.79(±3.98) <0.00a,b 0.09 UQoLoccupational 23.90(±6.70) 28.37(±5.56) <0.00a,b 22.04(±6.29) 25.97(±6.68) <0.00a,b 0.01c UQoLhealth 15.87(±5.35) 23.55(±4.94) <0.00a,b 15.44(±4.71) 20.58(±5.81) <0.00a,b 0.03c UQoLsexual 7.77(±2.49) 11.72(±2.18) <0.00a,b 7.62(±2.58) 10.00(±2.14) <0.00a,b 0.00c
Pre-treatmentandpost-treatmentvaluesexpressedasmeanandstandarddeviation.
a p<0.001(pairedStudent’st-testforintragroupanalysis).
b Strongtomoderateclinicalimpactoftheintervention(Cohen’sKappatest).
c p<0.05(mixed-designanalysisofvariance(ANOVA)betweenparticipantsinintergroupanalysis).
Sexual function is currentlyregarded as a key element forthegeneralwell-beingandqualityoflifeinmiddle-aged women,andthisfactorisinfluencedbysocio-demographic, biologicalandbehavioralvariablesrelevanttothestageoflife wherethesewomenare.33,34Inpreviousstudiesonthe
inves-tigationofsexualdysfunctions,itwaspossibletoobservethat thiscomplaintisquite common inclimactericwomen;35,36
andwheninvestigatedinwomenwithrheumaticdiseases,it wasobservedthatwomenwithfibromyalgiaexhibitahigher frequency,comparedtootherdiseases.20
Pelvicfloor muscletraining providesstability, resistance and strength ofthese muscles, increasedvaginaltone and consequentlyanimprovementinsexualfunction,by allow-ingabetterawarenessandpossiblyapositiveimpact,bothon orgasm andinsexualarousal.37–39 In ourstudy,theeffects
observed in the FMgroup were less importantthan those observed in climacteric women without fibromyalgia. This finding canbeattributedtothefactthatpsychiatric symp-toms,suchasdepression,arequitecommoninwomenwith fibromyalgia, which could exert a direct and detrimental
Table3–Analysisofintra-andintergroupofsexualfunctionthroughSQ-Fquestionnaireandseverityofclimacteric symptoms,consideringpre-andpost-intervention.
Variables Control Fibromyalgia Intergroup
difference,P
Pre Post Intragroup
difference,p
Pre Post Intragroup
difference,p
Mean(±SD) Mean(±SD) Mean(±SD) Mean(±SD)
Sexualfunction, SQ-F
38.80(±18.97) 50.67(±16.46) <0.00a,b 37.48(±16.65) 43.34(±15.55) <0.00a 0.01c
Climacteric symptoms,BKMI
30.15(±10.93) 19.20(±9.34) <0.00a,b 34.06(±10.45) 23.23(±9.29) <0.00a,b 0.73
Pre-treatmentandpost-treatmentvaluesexpressedasmeanandstandarddeviation.
a p<0.001(pairedStudent’st-testforintragroupanalysis).
b Strongtomoderateclinicalimpactoftheintervention(Cohen’sKappatest).
influence on the sexual function of these women, thus complicatingtheattainmentofmoresignificanttherapeutic responses.40
Theclimactericsymptoms, duetohormonalchanges as hypoestrogenism,negativelyinfluencethequalityoflifeand functionalityofwomen whoare experiencingthis phase.41
Thetreatmentwithkinesiotherapyexercisesforpelvicfloor, although not related in previous studies as a therapeutic waytoeasetheintensityofclimactericsymptoms,allowed a homogeneous reduction in the scores of BKMI for both groups,showingthatthediagnosisoffibromyalgiadoesnot interferedirectlyintheimpactofanexerciseprogramfor cli-mactericsymptoms.Basedontheseresults,itisplausibleto suggest thatevenpatients withfibromyalgiawould benefit withpelvicfloorkinesiotherapy,forimprovementoftheir cli-mactericsymptoms.Despitethis,arecentstudyemphasizes thatwomenwithfibromyalgiaexhibithypersensitivitytopain andworseningofsignsandsymptomsrelatedtomenopause, whencompared tohealthy women, inconsequenceofthe earlyonsetofmenopauseand,thus,areducedexposuretime ofthesewomentoestrogen.42
Given the findings highlighted in this study, we may suggestthatpelvicfloorkinesiotherapyprovidessignificant improvement in quality of life in occupation, emotional, healthandsexualdomains,aswellasinclimacteric symp-toms and also in sexual function. However, when the improvementinthegroupdiagnosedwithfibromyalgiawas comparedwiththatinthecontrolgroup,itwasobservedthat fibromyalgiaexertsalimitingeffectontheimprovementin health,occupationalandsexualdomainsofqualityoflifeand alsoinsexualfunctioninginclimactericwomen.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. WolfeF,RossK,AndersonJ,RussellIJ.Aspectsoffibromyalgia inthegeneralpopulation:sex,painthreshold,and
fibromyalgiasymptoms.JRheumatol.1995;22:151–6.
2. WolfeF,SmytheHA,YunusMB,BennettRM,BombardierC, GoldenbergDL,etal.TheAmericanCollegeofRheumatology 1990criteriaforclassificationoffibromyalgia:reportofthe multicentercriteriacommittee.ArthritisRheum.
1990;33:160–72.
3. InstituteforClinicalSystemsImprovement(ICSI).
Assessmentandmanagementofchronicpain.Bloomington, MN:InstituteforClinicalSystemsImprovement(ICSI);2007, 87pp.
4. HootenWM,SmithJM,EldrigeJS,OlsenDA,MauckWD, MoeschlerSM.Painseverityisassociatedwithmuscle strengthandpeakoxygenuptakeinadultswithfibromyalgia. JPainRes.2014;3:237–42.
5. GranJT.Theepidemiologyofchronicgeneralized musculoskeletalpain.BestPractResClinRheumatol. 2003;17:547–61.
6. OstensenM,RugelsjøenA,WigersSH.Theeffectof
reproductiveeventsandalterationsofsexhormonelevelson thesymptomsoffibromyalgia.ScandJRheumatol.
1997;26:355–60.
7.CavalcanteAB,SauerJF,ChalotSD,Assumpc¸ãoA,LageLV, MatsutaniLA,etal.Theprevalenceoffibromyalgia:a literaturereview.RevBrasReumatol.2006;46:40–8.
8.MartinezJE,AtraE,FerrazMB,SilvaPSB.Fibromialgia: aspectosclínicosesocioeconômicos.RevBrasReumatol. 1992;32:225–30.
9.YunusM,MasiAT,CalabroJJ,MillerKA,FeigenbaumSL. Primaryfibromyalgia(fibrositis):clinicalstudyof50patients withmatchednormalcontrols.SeminArthritisRheum. 1981;11:151–71.
10.BlümelJE,PalaciosS,LegorretaD,VallejoMS,SarraS.Is fibromyalgiapartoftheclimactericsyndrome?Maturitas. 2012;73:87–93.
11.BaldursdóttirS.Juvenileprimaryfibromyalgiasyndrome– review.Laeknabladid.2008;94:463–72.
12.GalvãoLLLF,Dissertac¸ão[Mestrado]emCiênciasdaSaúde Traduc¸ão,Adaptac¸ãoeValidac¸ãodaVersãoBrasileirado QuestionárioUtianQualityOfLife(UQOL)ParaAvaliac¸ãoda QualidadedeVidanoClimatério.Natal,RN:Universidade FederaldoRioGrandedoNorte,UFRN;2007.
13.SousaRL,SousaESS,SilvaJCB,FilizolaRG.Fidedignidadedo teste-retestenaaplicac¸ãodoíndicemenopausaldeBlatte Kupperman.RevBrasGinecolObstet.2000;22:481–7.
14.AbdoCHN.Elaborac¸ãoevalidac¸ãodoquocientesexual– versãofeminina:umaescalaparaavaliarafunc¸ãosexualda mulher.RevBrasMed.2006;63:477–82.
15.CavalcanteA,SauerJ,ChalotS,Assumpc¸ãoA,LageL, MatsutaniL,etal.Aprevalênciadefibromialgia:umarevisão daliteratura.RevBrasReumatol.2006;46:40–8.
16.CamposRP,VázquezMI.Theimpactoffibromyalgiaon health-relatedqualityoflifeinpatientsaccordingtoage. Rheumatology.2013;33:1419–24.
17.KalichmanL.Associationbetweenfibromyalgiaandsexual dysfunctioninwomen.ClinRheumatol.2009;28:365–9.
18.BirttaneM,UzuncaK,TunaH.Theevaluationofqualityoflife infibromyalgiasyndrome:acomparisonwithrheumatoid arthritisbyusingSF-36HealthSurvey.ClinRheumatol. 2007;26:679–84.
19.BurckhardtCS,ClarkSR,BennettRM.Fibromyalgiaand qualityoflife:acomparativeanalysis.Rheumatology. 1993;20:475–9.
20.FerreiraCC,MotaLM,OliveiraAC,CarvalhoJF,LimaRA, SimaanCK,etal.Frequencyofsexualdysfunctioninwomen withrheumaticdiseases.RevBrasReumatol.2013;53: 41–6.
21.PaulsRN,CrispCC,NovickiK,FellnerAN,KleemanSD. Impactofphysicaltherapyonqualityoflifeandfunction aftervaginalreconstructivesurgery.FemalePelvicMed ReconstrSurg.2013;19:271–7.
22.FanHL,ChanSS,LawTS,CheungRY,ChungTK.Pelvicfloor muscletrainingimprovesqualityoflifeofwomenwith urinaryincontinence:aprospectivestudy.AustNZJObstet Gynaecol.2013;53:298–304.
23.StüppL,ResendeAP,OliveiraE,CastroRA,GirãoMJ,Sartori MG.Pelvicfloormuscletrainingfortreatmentofpelvicorgan prolapse:anassessor-blindedrandomizedcontrolledtrial.Int UrogynecolJ.2011;22:1233–9.
24.OgwumikeOO,SanyaAO,ArowojoluAO.Enduranceexercise effectonqualityoflifeandmenopausalsymptomsin Nigerianwomen.AfrJMed.2011;40:187–95.
25.BernikM,SampaioTP,GandarelaL.Fibromyalgiacomorbid withanxietydisordersanddepression:combinedmedical andpsychologicaltreatment.CurrPainHeadacheRep. 2013;17:358.
26.FreitasKM,SilvaARV,SilvaRM.Mulheresvivenciandoo climatério.ActaSci.2004;26:121–8.
28.OncüJ,Bas¸o ˘gluF,KuranB.Acomparisonofimpactoffatigue oncognitive,physical,andpsychosocialstatusinpatients withfibromyalgiaandrheumatoidarthritis.Rheumatology. 2013;33:3031–7.
29.MannerkorpiK,GardG.Hindersforcontinuedworkamong personswithfibromyalgia.MusculoskeletDisorders. 2012;13:96.
30.BjörnsdóttirSV,JónssonSH,ValdimarsdóttirUA.Functional limitationsandphysicalsymptomsofindividualswith chronicpain.ScandJRheumatol.2013;42:59–70.
31.BennettRM.Clinicalmanifestations.Diagnosisof fibromyalgia.RheumDisClinNAm.2009;35:215–32.
32.Mendonc¸aLLF,MarquesAP,MatsutaniLA,FerreiraEAG. Exercíciosdealongamentoparapacientescomfibromialgia. RevBrasReumatol.2002;42:49–50.
33.LindauST,GavrilovaN.Sex,health,andyearsofsexually activelifegainedduetogoodhealth:evidencefromtwoUS populationbasedcrosssectionalsurveysofageing.BMJ. 2010;340:810.
34.ValadaresAL,Pinto-NetoAM,OsisMJ,CondeDM,SousaMH, Costa-PaivaL.SexualityinBrazilianwomenaged40to65 yearswith11yearsormoreofformaleducation:associated factors.Menopause.2008;15:264–9.
35.ChedrauiP,Pérez-LópezFR,SánchezH,AguirreW,Martínez N,MirandaO,etal.Assessmentofsexualfunctionof mid-agedEcuadorianwomenwiththe6-itemFemaleSexual FunctionIndex.Maturitas.2012;71:407–12.
36.CabralPU,CanárioAC,SpyridesMH,UchôaSA,EleutérioJJr, Gonc¸alvesAK.Determinantsofsexualdysfunctionamong middle-agedwomen.IntJGynaecolObstet.2013;120: 271–4.
37.AthanasiosGZ,MariaVK,PolyanthiDP.Pelvicfloormuscle trainingimprovessexualfunctionofwomenwithstress urinaryincontinence.IntUrogynecolJ.2008;19:401–6.
38.LowensteinL,GruenwaldI,GartmanI,VardiY.Canstronger pelvicmusclefloorimprovesexualfunction.IntUrogynecolJ. 2010;21:553–6.
39.StafneSN,SalvesenKÅ,RomundstadPR,TorjusenIH, MørkvedS.Doesregularexerciseincludingpelvicfloor muscletrainingpreventurinaryandanalincontinence duringpregnancy.Arandomisedcontrolledtrial.BJOG. 2012;119:1270–80.
40.AydinG,Bas¸arMM,Keles¸I,ErgünG,OrkunS,BatislamE. Relationshipbetweensexualdysfunctionandpsychiatric statusinpremenopausalwomenwithfibromyalgia.Urology. 2006;67:156–61.
41.PamukON,CakirN.Thevariationinchronicwidespreadpain andothersymptomsinfibromyalgiapatients.Theeffectsof mensesandmenopause.ClinExpRheumatol.2005;23: 778–82.