w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Serum
Clara
cell
16-kDa
protein
levels
and
lung
impairment
in
systemic
sclerosis
patients
Anna
Olewicz-Gawlik
a,∗,
Dorota
Trzybulska
a,
Barbara
Kuznar-Kaminska
b,
Katarzyna
Katulska
c,
Aleksandra
Danczak-Pazdrowska
d,
Halina
Batura-Gabryel
b,
Pawel
Hrycaj
aaDepartmentofRheumatologyandClinicalImmunology,PoznanUniversityofMedicalSciences,Poznan,Poland
bDepartmentofPulmonology,AllergologyandPulmonaryOncology,PoznanUniversityofMedicalSciences,Poznan,Poland
cDepartmentofGeneralRadiologyandNeuroradiology,PoznanUniversityofMedicalSciences,Poznan,Poland
dDepartmentofDermatology,PoznanUniversityofMedicalSciences,Poznan,Poland
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received22April2014 Accepted30April2015 Availableonline12August2015
Keywords: CC16
Interstitiallungdisease Systemicsclerosis
a
b
s
t
r
a
c
t
Objective:Toassess clinicalutilityofserumClaracell16-kDaproteinmeasurements in relationwithstagingsystemforsystemicsclerosisassociatedinterstitiallungdisease. Materialsandmethods:SerumlevelsofClaracell16-kDaproteinweredeterminedbyELISAin 28systemicsclerosispatientsand30healthycontrols,andcorrelatedwithstagingsystem forsystemicsclerosisassociatedinterstitiallungdiseaseinsystemicsclerosispatients.Lung involvementwasassessedfunctionally(bodyplethysmography,diffusingcapacityofthe lungforcarbonmonoxide)andradiologically(anaveragediseaseextentonhighresolution computedtomographyofthelungs)inSScpatients.
Results:WeobservedstatisticallysignificantdifferencesinserumClaracell16-kDaprotein levelsbetweensystemicsclerosispatientsandhealthycontrolsonlyinnon-smokers. How-ever,serumClaracell16-kDaproteinconcentrationsweresignificantlyelevatedinpatients withhighresolutioncomputedtomographyextent>20%incomparisontopatientswith highresolutioncomputedtomographyextent<20%(p=0.01).Theycorrelatedpositivelywith averagediseaseextentonhighresolutioncomputedtomography(p=0.04),anextentofa reticularpatternonhighresolutioncomputedtomography(p<0.01),andnegativelywitha totallungcapacity(p=0.03)andtheresultsofthe6-minwalktest(p<0.01).
Conclusions: Claracell16-kDaproteinlevelscanbeconsideredasasupplementalserum biomarkerforsystemicsclerosisassociatedinterstitiallungdisease.
©2015ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](A.Olewicz-Gawlik). http://dx.doi.org/10.1016/j.rbre.2015.07.005
Níveis
séricos
de
proteína
de
células
de
Clara
de
16
kDa
e
comprometimento
pulmonar
em
pacientes
com
esclerose
sistêmica
Palavras-chave: CC16
Doenc¸aintersticialpulmonar Esclerosesistêmica
r
e
s
u
m
o
Objetivo: Avaliarautilidadeclínicadasmedic¸õesséricasdaproteínadecélulasdeClarade 16-kDaemrelac¸ãoaosistemadeestadiamentoparadoenc¸apulmonarintersticialassociada aesclerosesistêmica.
Materiaisemétodos: ForamdeterminadososníveisséricosdeproteínadecélulasdeClara de16-kDaporELISAem28pacientescomesclerosesist ˛emicae30controlessaudáveis,e correlacionadoscomosistemadeestadiamentoparadoenc¸pulmonarintersticialassociada aesclerosesist ˛emicaempacientescomesclerosesist ˛emica.Oenvolvimentopulmonarfoi avaliadofuncionalmente(pletismografiacorporal,capacidadededifusãodemonóxidode carbono)eradiologicamente(extensãomédiadadoenc¸anatomografiacomputadorizada dealtaresoluc¸ãodospulmões)empacientescomesclerosesist ˛emica.
Resultados: Foramencontradasdiferenc¸asestatisticamentesignificativasnosníveisséricos deproteínadecélulasdeClarade16-kDaentrepacientescomesclerosesist ˛emicae con-trolessaudáveisapenasemnãotabagistas.Noentanto,asconcentrac¸õesséricasdeproteína decélulasdeClarade16-kDaeramsignificativamenteelevadasempacientescomextensão >20%natomografiacomputadorizadadealtaresoluc¸ãoemcomparac¸ãoapacientescom extensão<20%natomografiacomputadorizadadealtaresoluc¸ão(p=0,01).Osníveisséricos deproteínadecélulasdeClarade16-kDasecorrelacionarampositivamentecoma exten-sãomédiadadoenc¸anatomografiacomputadorizadadealtaresoluc¸ão(p=0,04)ecoma extensãodepadrãoreticularnatomografiacomputadorizadadealtaresoluc¸ão(p<0,01),e negativamentecomacapacidadepulmonartotal(p=0,03)ecomosresultadosdotestede caminhadade6min(p<0,01).
Conclusões: OsníveisdeproteínadecélulasdeClarade16-kDapodemserconsiderados comobiomarcadoresséricossuplementaresparaadoenc¸apulmonarintersticialassociada aesclerosesist ˛emica.
©2015ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Systemicsclerosis(SSc)isachronic,autoimmuneconnective tissuedisease characterisedbyvasculopathy, inflammation and progressive fibrosis of the skin and internal organs. Theleading causes ofmorbidity and mortality inpatients
with SSc are two SSc-related pulmonary syndromes:
pul-monaryarterialhypertension(SSc-PAH)andinterstitiallung disease (SSc-ILD).1 Toassess SSc-ILD, high-resolution
com-putedtomography(HRCT)andpulmonaryfunctiontestsare
performed.Inaddition,afewlung-specificserological mark-ersofSSc-ILD havebeen described.2–4 Thisgroup includes
Clara cell 16-kDa protein (CC16). It is one of the major
proteins secreted by Clara cells and there is growing evi-denceonitsprotectiveroleagainstpulmonaryinflammatory response.5
CC16isa15.8-kDahomodimericproteinencodedbyagene localisedtochromosome11.6Ithaspotentnatural
immuno-suppressiveandanti-inflammatoryproperties.CC16hasbeen showntomodulateinflammatoryresponse,including inhibi-tionofcytosolicphospholipaseA2activityandinterferon-␥in vitro.7ChangesinserumCC16concentrationswereobserved
inpatientswithdifferentdisordersaffectingthelungs, includ-ingdecreasedCC16levelsinbronchialasthmaandincreased insarcoidosisandidiopathicpulmonaryfibrosis.8,9Theywere
alsonotedafterexposuretolung irritants.10 Moreover,the
serum level ofCC16has been found tobe an indicatorof
activepulmonaryfibrosisinSScpatients.11 Inregardtothis
finding,inthepresentstudyweevaluatedserumCC16levels andexaminedtheirassociationwithSSc-ILDassessmentin patientswithSSc.
Materials
and
methods
Werecruitedforthestudy28consecutivepatientswithSSc(25 femalesand3males,agedbetween24and70years) accord-ing totheAmerican CollegeofRheumatologyclassification criteria.12Allpatientswerealsoanalysedwiththeuseof2013
classificationcriteriaforSSc.13Patientsweregrouped
accord-ingtothe2-cutaneoussubsetclassificationashavingdiffuse cutaneous(dcSSc)orlimitedcutaneous(lcSSc)formofthe dis-easeonthebasisoftheextentoftheirskininvolvement.14
Healthy controls(n=30) were non-smoking volunteers and were statisticallymatchedbygenderand age(18–29,30–44, 45–54and55–70yearsofage).Thestudywasapprovedbythe InstitutionalReviewBoardatPoznanUniversityofMedical Sci-encesandwritteninformedconsentwasobtainedfromevery participant.Aprotocoloftheconductedresearchconformsto theprinciplesoftheWorldMedicalAssociation’sDeclaration ofHelsinki.
Clinicalassessmentcomprisedthecompletemedical
assessmentandevaluationofskininvolvementusing mod-ifiedRodnanskinthicknessscore.15EuropeanLeagueAgainst
Rheumatism (EULAR) Scleroderma Trials and Research
(EUSTAR) Systemic Sclerosis Activity Score was calculated
for all SSc patients. Disease duration was measured from
the onset of the first symptom, other than Raynaud’s
phenomenon,consistent withSSc.Pulmonary involvement
wasassessedfunctionally(bodyplethysmography,diffusing capacityofthelungforcarbonmonoxide[DLCO]andthe 6-minwalktest)andradiologically(highresolutioncomputed tomographyofthelungs,HRCT)asproposedbyGohetal.16
Moreover,HRCTimageswerealsoassessedforthefollowing findings:theaverage extentofthedisease,the extentofa reticularpattern,theextentofgroundglassappearanceand
thepresenceofhoneycombing.AllHRCTexaminationswere
evaluatedbyaradiologyexpertonHRCTILD.TodescribeSSc patientsas‘withoutpulmonaryfunctionimpairment’,three functionalparameters:totallungcapacity(TLC),vital capac-ity (VC) and DLCO were defined as >80% predicted. Blood samplesfrompatientswerecollectedatthetimeofthe
clin-ical examination on fasting conditions and obtained sera
werestoredat−70◦Cbeforetheassayswereperformed.The
inflammatoryactivitywasdeterminedbytheerythrocyte sed-imentationrate(ESR,Westergren),high-sensitivityC-reactive
proteinconcentration (CRP, enzyme-linkedimmunosorbent
assay(ELISA),BioCheck,USA)andcomplementcomponents
C3andC4levels(radial immunoelectrophoresis).Thetitres ofantinuclear antibodies (ANAs)were assessedbyan indi-rectimmunofluorescenceassaywithtwoBIOCHIPsperfield containingHEp-20-10cellsandmonkeylivertissue (Euroim-mun,Germany).Antibodies toextractablenuclear antigens
(ENA) were determined using blot type test ANA Profile 3
(Euroimmun,Germany).SerumconcentrationsofCC16were
measuredusingcommerciallyavailableELISAkits(BioVendor, theCzechRepublic)accordingtothemanufacturer’sprotocol. Patients’demographicdatawereanalysedusing descrip-tivestatisticsandthedataweretestedfornormaldistribution usingtheKolmogorov–Smirnovtest.Theresultsarepresented throughoutthearticleasthemean±standarddeviation(SD) fornormallydistributeddataorasthemedian(interquartile range,IQR)fornon-normally distributed data.Associations
betweendifferentvalues were examinedusing Spearman’s
rank-order correlation analysis. Differences between the
groupswere calculatedusing the Mann–Whitney U test. A
p-value less than 0.05 was considered statistically signifi-cant.AllstatisticalanalyseswereperformedwithSTATISTICA dataanalysissoftwaresystem(StatSoft,Inc.,2011,version10, www.statsoft.com).
Results
Outof28SScpatients,11haddcSSc(9femalesand2males) and17hadlcSSc(16femalesand1male).Tenpatients(35.7%) hadamodifiedRodnanskinthicknessscoreofmorethan14 and 7(25%)had activedisease according toEUSTAR activ-ityscore. Onepatient (3.6%)had SSc-PAH and noneofthe patientshadimpairedrenalfunction.In27patients(96.4%)
lung-functiontestsshoweddecreasedDLCO,VCwas
dimin-ishedin4patients(14.3%)andTLCin1patient(3.6%).There
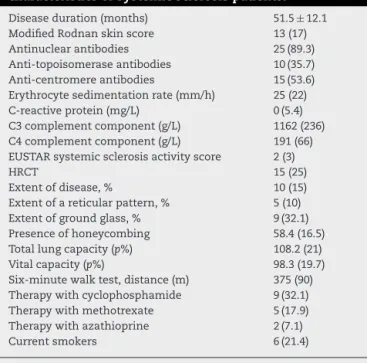
Table1–Clinical,laboratoryandradiological characteristicsofsystemicsclerosispatients.
Diseaseduration(months) 51.5±12.1 ModifiedRodnanskinscore 13(17) Antinuclearantibodies 25(89.3) Anti-topoisomeraseantibodies 10(35.7) Anti-centromereantibodies 15(53.6) Erythrocytesedimentationrate(mm/h) 25(22) C-reactiveprotein(mg/L) 0(5.4) C3complementcomponent(g/L) 1162(236) C4complementcomponent(g/L) 191(66) EUSTARsystemicsclerosisactivityscore 2(3)
HRCT 15(25)
Extentofdisease,% 10(15) Extentofareticularpattern,% 5(10) Extentofgroundglass,% 9(32.1) Presenceofhoneycombing 58.4(16.5) Totallungcapacity(p%) 108.2(21) Vitalcapacity(p%) 98.3(19.7) Six-minutewalktest,distance(m) 375(90) Therapywithcyclophosphamide 9(32.1) Therapywithmethotrexate 5(17.9) Therapywithazathioprine 2(7.1) Currentsmokers 6(21.4)
HRCT,highresolutioncomputedtomography.
Data presented as the median (interquartile range), mean±standarddeviationorasn(%).
wasnocaseofconcomitantbronchialasthmaorsarcoidosisin theinvestigatedgroup.ComparisonbetweendcSScandlcSSc revealednostatisticallysignificantdifferencesinpulmonary functiontestswithregardtopercentageofpredictedTLC,VC andDLCO.SignificantabnormalitiesonHRCT(ILDextentof >5%)were observedin53.6%ofthepatientsandILDextent >20% waspresent in32.1%ofthe patientswithSSc.There werenopatientswiththeindeterminateextentofthedisease onHRCT.Furthercharacteristicsofthepatientgroupatthe timeofexaminationisshowninTable1.
We did not observe statistically significant differences
in serum CC16 levels between SSc patients (median 9.9
(7.3)ng/mL) and healthy controls (median 8.4 (3.7)ng/mL) (Fig. 1), or between dcSSc and lcSSc subgroups. However,
35
0
Systemic sclerosis Control 5
10
CC16 [ng/mL]
15 20 25 30
Median
Systemic sclerosis non-smokers Control 0
2 4 6 8 10 12 14 16 18 20 22 24 26 28
CC16
[n
g/
m
L]
Median
Fig.2–SerumCC16(ng/mL)concentrationsinnon-smoker
patientswithsystemicsclerosis(n=22)andinhealthy
controls(n=30).
exclusionofsmokersfromthisanalysisrevealedsignificantly
increased serum CC16 concentrations in non-smoker SSc
patientsincomparisontothecontrols(median10.2(5.8)vs. 8.4 (3.7) ng/mL, p=0.03) (Fig. 2). In the whole investigated
SSc group CC16 concentrations were also associated with
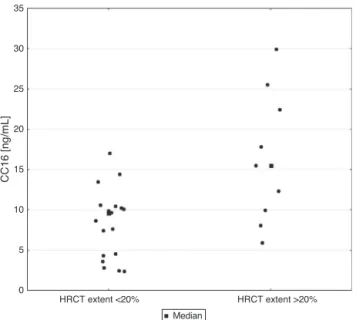
patients’age(r=0.41,p=0.03)andweresignificantlydecreased insmokers(p=0.03).SerumlevelsofCC16weresignificantly elevatedinpatientswithHRCTextent>20%incomparison topatients withHRCT extent<20% (p=0.01)(Fig. 3). More-over,CC16 levelssignificantly correlated withHRCT extent whenpresentedasacontinuousvariable(r=0.44,p=0.04)and withthe extentofreticular pattern (r=0.61, p<0.01). With regardtopulmonaryfunctiontestsCC16concentrationswere
35
30
25
CC16 [ng/mL]
HRCT extent <20% HRCT extent >20% 20
15
10
5
0
Median
Fig.3–SerumCC16(ng/mL)concentrationsinsystemic sclerosispatientswithHRCTextent<20%andHRCTextent >20%.
associatednegativelywithTLC(r=−0.41,p=0.03)andwiththe resultofthe6-minwalktest(r=−0.55,p<0.01).Noother statis-ticallysignificantassociationsweredetectedbetweenserum CC16levelsandclinical orlaboratoryfindings,asshownin Table1.
Discussion
Thecurrent reportfocuses onserum levels ofCC16 inSSc patientsinrelationtostagingsystemofSSc-ILD.
WefoundstatisticallysignificantdifferenceinserumCC16
levels onlybetween non-smoker SSc patients and healthy
controls,butnotwhensmokerandnon-smokerSScpatients were analysed together as a whole group. It is consistent withtheresultsfromthepreviousreport,whereSScpatients had higher,but notstatisticallysignificant,serum levelsof CC16comparedwiththelevelsofhealthycontrols.11However,
we cannotexcludea biascaused byasmall sample
num-berofsmokersandarelativelylownumberofallindividuals includedtothestudy.
Further,wedidnotobservearelationshipbetweenCC16 levelsandVC,asitwasreportedbytheothers.11Themost
probable explanation for these discrepancies is the differ-enceintreatment(notreatmentvs.57.1%ofpatientstreated
with immunosuppressivedrugsin ourstudy).These
diver-gentresultscanalsobeinfluencedbyasmallsamplesizein thepresentstudy.However,wefoundthatCC16levelswere significantly elevated in SSc patients with average disease extentonHRCT>20%comparedtopatientswithaverage dis-easeextent<20%,andthatserumCC16significantlycorrelated withtheaverageextentofthediseaseonHRCTwhenanalysed ascontinuousvariable.Theseobservationsareinagreement withthefindingthatserumCC16levelsinSScpatientswith pulmonaryfibrosiswereremarkablyhigherinactivevs. inac-tivelungdisease.InthestudybyHasegawaetal.,diagnosis ofactive pulmonaryfibrosis wasbased on thepresenceof ground-glassappearanceorreticularpatternonHRCTofthe chestand>10%changeinVCor>15%changeinDLCOwithin1 year.Asourstudywasbasedonthecase-controlapproach,we couldnotjudgetheSSc-ILDactivitybasingonthesame crite-ria,butourresultsalsoindicateCC16asamarkerofSSc-ILD, asweshowedanassociationofCC16serumlevelswiththe extentofreticularpatternonHRCT.Thisfindingisof particu-larclinicalimportanceasinthestudybyGohetal.16mortality
in SSc patients wasstrongly linkednot onlytothe extent ofdisease on HRCT, but alsotothe extentof thereticular pattern.Therefore,elevatedserumCC16levelcanbea can-didateforaprognosticmarkerinSScpatients,especiallyin non-smokers.
Additionally, inthis study we observeddecreased CC16 serumconcentrationsinsmokingSScpatients.Itis concord-ant withthepreviousresults,whichshowedapproximately 30%reductionofCC16levelsinsmokers.17
Tosumup,ourdataindicatethatelevatedCC16 concentra-tionsreflectthedegreeoflungdamageinthecourseofSScas scoredwithstagingsystembyGohetal.16Further,CC16level
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The research reported here and the preparation of this
manuscriptwerepartiallyfundedbyMinistryofScienceand HigherEducationofPoland(grantNN402472737).Wewould
like to thankMs. Ewa Mazurkiewicz for the review ofthe
manuscript.
r
e
f
e
r
e
n
c
e
s
1. LePavecJ,LaunayD,MathaiSC,HassounPM,HumbertM. Sclerodermalungdisease.ClinRevAllergyImmunol. 2011;40(2):104–16.
2. HasegawaM,AsanoY,EndoH,FujimotoM,GotoD,IhnH, etal.Serumadhesionmoleculelevelsasprognosticmarkers inpatientswithearlysystemicsclerosis:amulticentre, prospective,observationalstudy.PLOSONE.2014;9(2):e88150. 3. AozasaN,AsanoY,AkamataK,NodaS,MasuiY,TamakiZ,
etal.Clinicalsignificanceofserumlevelsofsecretory leukocyteproteaseinhibitorinpatientswithsystemic sclerosis.ModRheumatol.2012;22(4):576–83.
4. BonellaF,VolpeA,CaramaschiP,NavaC,FerrariP,SchenkK, etal.SurfactantproteinDandKL-6serumlevelsinsystemic sclerosis:correlationwithlungandsystemicinvolvement. SarcoidosisVascDiffuseLungDis.2011;28(1):27–33.
5. BernardA,DumontX,RoelsH,LauwerysR,DierynckI,DeLey M,etal.Themolecularmassandconcentrationsofprotein1 orClaracellproteininbiologicalfluids:areappraisal.Clin ChimActa.1993;223(1–2):189–91.
6. HayJG,DanelC,ChuCS,CrystalRG.HumanCC10gene expressioninairwayepitheliumandsubchromosomallocus suggestlinkagetoairwaydisease.AmJPhysiol.1995;2684Pt 1:L565–75.
7.BroeckaertF,ClippeA,KnoopsB,HermansC,BernardA.Clara cellsecretoryprotein(CC16):featuresasaperipherallung biomarker.AnnNYAcadSci.2000;923:68–77.
8.ShijuboN,ItohY,YamaguchiT,SugayaF,HirasawaM, YamadaT,etal.SerumlevelsofClaracell10-kDaproteinare decreasedinpatientswithasthma.Lung.1999;177(1):45–52. 9.HermansC,PetrekM,KolekV,WeynandB,PietersT,Lambert
M,etal.SerumClaracellprotein(CC16),amarkerofthe integrityoftheair-bloodbarrierinsarcoidosis.EurRespirJ. 2001;18(3):507–14.
10.BernardA,HermansC,VanHouteG.Transientincreaseof serumClaracellprotein(CC16)afterexposuretosmoke. OccupEnvironMed.1997;54(1):63–5.
11.HasegawaM,FujimotoM,HamaguchiY,MatsushitaT,Inoue K,SatoS,etal.Useofserumclaracell16-kDa(CC16)levelsas apotentialindicatorofactivepulmonaryfibrosisinsystemic sclerosis.JRheumatol.2011;38(5):877–84.
12.MasiA,RodnanG,MedsgerT,AltmanR,D’AngeloW,FriesJ, etal.Preliminarycriteriafortheclassificationofsystemic sclerosis(scleroderma).ArthritisRheum.1980;23(5):581–90. 13.vandenHoogenF,KhannaD,FransenJ,JohnsonSR,BaronM,
TyndallA,etal.2013classificationcriteriaforsystemic sclerosis:anAmericancollegeofrheumatology/European leagueagainstrheumatismcollaborativeinitiative.Ann RheumDis.2013;72(11):1747–55.
14.LeRoyE,BlackC,FleischmajerR,JablonskaS,KriegT,Medsger T,etal.Scleroderma(systemicsclerosis):classification, subsets,andpathogenesis.JRheumatol.1988;15(2):202–5. 15.ClementsP,LachenbruchP,SieboldJ,WhiteB,WeinerS,
MartinR,etal.Interandintraobservervariabilityoftotalskin thicknessscore(modifiedRodnanTSS)insystemicsclerosis.J Rheumatol.1995;22(7):1281–5.
16.GohNS,DesaiSR,VeeraraghavanS,HansellD,CopleyS, MaherT,etal.Interstitiallungdiseaseinsystemicsclerosis:a simplestagingsystem.AmJRespirCritCareMed.
2008;177(11):1248–54.
17.ShijuboN,ItohY,YamaguchiT,AbeS.Developmentofan enzyme-linkedimmunosorbentassayforClaracell10-kDa protein:inpursuitofclinicalsignificanceofserainpatients withasthmaandsarcoidosis.AnnNYAcadSci.