The
Brazilian
Journal
of
INFECTIOUS
DISEASES
w w w . e l s e v i e r . c o m / l o c a t e / b j i d
Review
article
Kidney
involvement
in
leishmaniasis—a
review
Geraldo
Bezerra
da
Silva
Junior
a,b,
Elvino
José
Guardão
Barros
c,
Elizabeth
De
Francesco
Daher
a,∗aPost-GraduationPrograminMedicalSciences,DepartmentofInternalMedicine,UniversidadeFederaldoCeará(UFC),Fortaleza,CE,
Brazil
bSchoolofMedicine,MasterinCollectiveHealth,HealthSciencesCenter,UniversidadedeFortaleza,Fortaleza,CE,Brazil
cDepartmentofInternalMedicine,SchoolofMedicine,UniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30September2013 Accepted11November2013 Availableonline29March2014
Keywords:
Visceralleishmaniasis
Americancutaneousleishmaniasis Kala-azar
Kidneydisease
a
b
s
t
r
a
c
t
LeishmaniasisisaninfectiousdiseasecausedbyprotozoaofthegenusLeishmania trans-mittedbyinsectsofthegenusLutzomyiasp.orPhlebotomussp.Themainsyndromesare cutaneousleishmaniasis,mucocutaneousleishmaniasis,visceralleishmaniasis(kala-azar) andpost-kala-azardermalleishmaniasis.Thisarticlereviewskidneyinvolvementin cuta-neousandvisceralleishmaniasis,highlightingtheaspectsoftheirpathophysiology,clinical manifestations,histopathologicalfindings,outcomeandtreatment.
©2014ElsevierEditoraLtda.Allrightsreserved.
Introduction
Leishmaniasis is an infectious disease caused by protozoa ofthegenusLeishmaniatransmittedbyinsectsofthegenus
Lutzomyia sp. or Phlebotomus sp.1 There are more than 20
species of leishmanias causing clinical manifestations in humans,andthemainsyndromesarecutaneous leishman-iasis, mucocutaneousleishmaniasis, visceral leishmaniasis (kala-azar),and post-kala-azardermal leishmaniasis.2 This
articlereviewskidneyinvolvementincutaneousandvisceral leishmaniasis.
∗ Correspondingauthorat:RuaVicenteLinhares,1198,60135-270,Fortaleza,Ceará,Brazil.
E-mail addresses: [email protected] (G.B. da Silva Junior), [email protected] (E.J. Guardão Barros), [email protected](E.DeFrancescoDaher).
Cutaneous
leishmaniasis
Kidneyinvolvementincutaneousleishmaniasis
There havebeen few studiesshowingrenal dysfunctionin Americancutaneousleishmaniasis(ACL),whichis,insome cases,associatedwiththeuseofspecifictreatmentwith pen-tavalentantimonialdrugs.3,4
In arecentstudy performed inourregion, atotal of73 patients admitted with ACL were evaluated. Acute kidney injury(AKI)wasobservedin17cases(23.2%),andoliguriawas
http://dx.doi.org/10.1016/j.bjid.2013.11.013
seeninonecase.Meanvalueofmaximumserumcreatinine (SCr)levelsduringhospitalstaywas1.6±0.6mg/dL.Risk fac-torsforAKIwereadvancedage,longertimebetweensymptom onsetandhospitaladmissionandlongerhospitalstay. Com-pleterenalfunctionrecoverywasobservedin11cases(64.7%) atthe time ofhospital discharge.5 Thissame study found
urinary abnormalities, including proteinuria (4.1%), hema-turia(4.1%)andleukocyturia(5.4%).Hypokalemiawasfound in12.3%ofcases.5ProteinuriaandAKIhadbeenpreviously
reportedinotherstudies.6,7
Decreasedurinaryconcentratingability,withnoreduction ofglomerularfiltrationrate(GFR),wasdemonstratedbyVeiga etal.,8whostudiedananimalmodelofleishmaniasistreated
withhighdosesofmeglumineantimoniate.Thisabnormality inurineconcentrationresultsfromtheactionofantidiuretic hormone(ADH) and also bya directactionof the drug in tubularcells.8 Highdoses ofantimonialdrugsalsocause a
reductioninGFR.
ACLishighly prevalent inthestate ofCeará,Northeast ofBrazil.Lowtreatmentadherence favorsthe development ofthemucocutaneousforms,whichrequireshigherdosesof antimonialdrugsforlongerperiods,which,inturn,increases itstoxicityevenfurther.Arecentstudywasperformedinthis regioninordertoinvestigaterenalabnormalitiesinpatients withACL.Oliveiraetal.9studied37patientswithconfirmed
diagnosisofACL,performedurinaryconcentrationand acid-ificationtestsandalsoinvestigatedtheexpressionofurinary exosomes inthe urine of thesepatients.3 Urinary
concen-tration deficit was found in 77% of cases. The expression of aquaporin was significantly reduced, while NKCC2 was increased,incomparisontothatinacontrolgroup.Urinary acidification deficit was less frequent (40.5%). The expres-sionofNHE3,H+-ATPaseandpendrinwassignificantlyhigher amongpatientsthanincontrols.3Inthissamecohort,a
uri-naryconcentrationdeficitwasshownin27cases(77%)before treatment with Glucantime®, while after treatment it was observedin31patients(88%)(p=0.344).Itisthenpossiblethat ACLcancauseurinaryconcentrationdeficitandspecific treat-mentsdonotdecreasethisdefect,althoughitdoesnotcause significantrenalfunctionimpairment.
Combineddefects(concentrationand acidification)were seenin12patients.Comparingthepatientswithand with-outtubulardysfunction,therewerenodifferencesregarding age,gender,timeofdisease,andnumberofcutaneouslesions. Therewasnosignificantabnormalityregardingexcretion frac-tion of sodium, potassium, calcium and phosphate. There wasasignificantdifferenceinserummagnesium concentra-tionsbetweenpatientswithandwithoutacidificationdeficit (2.15±0.06 vs. 2.33±0.04,p=0.02). Nopatient withurinary concentrationoracidificationdeficithadalbumin/creatinine ratio>30mg/g3.
Otherinfectiousdiseaseswithpredominantinvolvement ofskinandnerves,suchasleprosy,canalsoleadtoglomerular dysfunction.Oliveira etal.,9ina prospectivestudy with59
patientswithleprosy,showeddecreasedGFRin50%ofcases whenconsideringGFR<80mL/min/1.73m2,andin5%when consideringGFR<50mL/min/1.73m2.
Microalbuminuria is a known marker of glomerular dysfunction in diabetes mellitus10 and also in
cardiovas-cular diseases.11,12 Microalbuminuria higher than 30mg/g
creatininewasobservedin35%ofpatientswithACLfollowed inahealthcenterinthestateofCeará,Brazil,beforespecific treatment,andinonly8%ofpatientsaftertreatment,3
sug-gestingthe presenceofincipientglomerularlesioninduced byACLitself,withoutconcomitantGFRdecrease.
UrinaryexosomeswerealsofoundtobealteredinACL.3
Somestudieshaveshownthataquaporin-2(AQP2)isexcreted inurineintheformofvesicles.Itsamountcorrelateswith circulatinglevels,andisusedinstudiestoinvestigatebody waterbalance.13,14InthecohortofpatientswithACLstudied
byOliveiraetal.,3 anincreasedpercentageofpatientswith
urineconcentrationdeficitwasobservedandthiswas asso-ciatedwithlower expressionofAQP2.3 Theincreaseinthe
expressionofNKCC2canoccur asacompensatory mecha-nism.Abnormalitiesinthetransportersinvolvedinacid–base regulationwerealsoobserved,includinganincreased expres-sionofNHE3(proximaltubule),H-ATPaseandpendrin(distal tubule)inpatientswithACL,whichcouldexplaintheurinary acidificationdeficit.3
Pentavalent antimonial drugs are rapidly eliminated through the kidneys,15 so their use should be avoided in
patients with renal dysfunction, due to cardiotoxicity and renal functionworsening.Urinaryconcentratingdefecthas alsobeendescribedandtheheavymetalusedinantimonial compositionisthemainfactorresponsibleforthetoxicity.16
AKImaybeduetomassivedepositionofimmunecomplexes formedafter Leishmaniadestruction byantimonialdrugs, a phenomenonsimilartothatofHerxheimerreaction.17
Sam-paio et al.18 evaluated 11 patients with ACL who received
adoubledoseofantimonials(40mgSbv/kg/dayfor30days), andobservedthatonepatientdevelopedAKI.Eightpatients showedadecreaseinGFRafter30daysoftreatment.Theyalso observeddistalandproximaltubulardysfunction,evidenced asadecreaseinurinaryconcentrationabilityandincreased sodiumexcretionfraction.
Rarely,treatmentwithmeglumineantimoniatecancause AKIduetointerstitialnephritis.16Atlowdosesandforashort
period,pentavalent antimonialshowslowrenal toxicity.In ACL treatment,however, itismanytimesnecessary touse higherdosesofpentavalentantimonial,whichincreases tox-icity.
Visceral
leishmaniasis
Visceralleishmaniasisisachronic,lethal,parasiticdisease, causedbytheLeishmaniaparasite,anintracellularprotozoan. A large spectrum of clinical manifestations accompanies the Leishmania attack on reticuloendothelial tissues –liver, spleen, bonemarrow, lymph nodes,and the digestive sys-tem. Symptoms range from irregular and recurrent fever to pancytopenia, hemorrhagic spells, and liver and spleen enlargement.19
Kidneyinvolvementinchronicleishmaniasisisfrequent and associated with increased mortality. It is endemic in southern Europe and in tropical and sub-tropical areas of the globe,withaworldwideincidenceofapproximately0.5 millioncases/year.20Whenuntreated,itsmortalityratecan
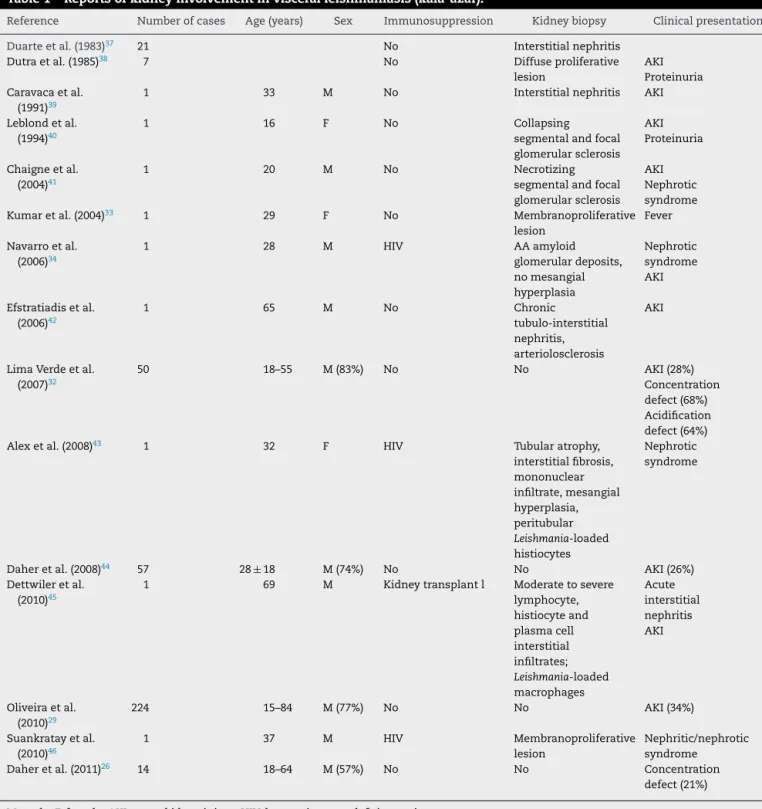
Table1–Reportsofkidneyinvolvementinvisceralleishmaniasis(kala-azar).
Reference Numberofcases Age(years) Sex Immunosuppression Kidneybiopsy Clinicalpresentation
Duarteetal.(1983)37 21 No Interstitialnephritis
Dutraetal.(1985)38 7 No Diffuseproliferative
lesion
AKI Proteinuria Caravacaetal.
(1991)39
1 33 M No Interstitialnephritis AKI
Leblondetal. (1994)40
1 16 F No Collapsing
segmentalandfocal glomerularsclerosis
AKI Proteinuria
Chaigneetal. (2004)41
1 20 M No Necrotizing
segmentalandfocal glomerularsclerosis
AKI Nephrotic syndrome
Kumaretal.(2004)33 1 29 F No Membranoproliferative
lesion
Fever
Navarroetal. (2006)34
1 28 M HIV AAamyloid
glomerulardeposits, nomesangial hyperplasia
Nephrotic syndrome AKI
Efstratiadisetal. (2006)42
1 65 M No Chronic
tubulo-interstitial nephritis, arteriolosclerosis
AKI
LimaVerdeetal. (2007)32
50 18–55 M(83%) No No AKI(28%)
Concentration defect(68%) Acidification defect(64%)
Alexetal.(2008)43 1 32 F HIV Tubularatrophy,
interstitialfibrosis, mononuclear infiltrate,mesangial hyperplasia, peritubular
Leishmania-loaded histiocytes
Nephrotic syndrome
Daheretal.(2008)44 57 28±18 M(74%) No No AKI(26%)
Dettwileretal. (2010)45
1 69 M Kidneytransplantl Moderatetosevere
lymphocyte, histiocyteand plasmacell interstitial infiltrates;
Leishmania-loaded macrophages
Acute interstitial nephritis AKI
Oliveiraetal. (2010)29
224 15–84 M(77%) No No AKI(34%)
Suankratayetal. (2010)46
1 37 M HIV Membranoproliferative
lesion
Nephritic/nephrotic syndrome
Daheretal.(2011)26 14 18–64 M(57%) No No Concentration
defect(21%)
M,male;F,female;AKI,acutekidneyinjury;HIV,humanimmunodeficiencyvirus.
Leishmaniachagasi. Humansare infectedthroughthevector insect, Lutzomyia longipalpis.21 Kala-azar diagnosis is
con-firmed by demonstrating the presence of the parasite in tissuesusingGiemsastain,inadditiontodetectionofparasite antigenK-39.19
Kidneyinvolvementinvisceralleishmaniasis
Patients presenting with chronic kala-azar can have mild proteinuria,microscopichematuriaandleukocyturia. Hypoal-buminemia,hypergammaglobulinemiaandincreasedplasma
levels of both IgG and b2-microglobulins were found in a groupof55patientswithvisceralleishmaniasis.22Increased
albuminexcretionhasbeenobservedin44%ofpatients. Pro-teinuria consisted predominantly of low molecular weight protein fractions that migrated with alpha1, alpha2, beta, and especially gammaglobulins. Urinary b2-microglobulin excretion was elevated in all patients. Microalbuminuria was detected in more than 40% of patients with vis-ceral leishmaniasis, even in those with normal creatinine levels.23Interstitialnephritiswithglomerularchangescanbe
membranoproliferative lesion is not rare.19 Additionally,
amyloid deposits can occur in chronic disease. Yet, renal involvementis usuallymild and transitory. Lossof kidney functionand urinarysedimentchangeshavebeenreported invisceralleishmaniasis.Prospectivestudieswithkala-azar patientshavedemonstratedhematuria,mildtomoderate pro-teinuria,andincreasedurineleukocytesinover50%ofcases.24
Alarge,retrospectivestudydemonstratedthatmorethan11% ofpatientswithchronicLeishmaniadiseasehaddecreased fil-trationrateathospitaladmission–withanti-parasitictherapy, changes disappear. Table 1 depicts known kidney involve-mentinkala-azar.Interestingly,hypoalbuminemia,polyclonal hypergammaglobulinemiaand leukopenia usuallyoccur in chronicleishmaniasis.19
Other less frequent disorders have been described in visceral leishmaniasis, including hormone and electrolyte abnormalities.InastudybyLimarVerdeetal.,of72patients
with visceral leishmaniasis, plasma ACTH (corticotrophin) wasfoundtobesignificantlyhigheramongpatientsin com-parisontonormalsubjects,aswellasplasmareninactivity. Primary adrenal insufficiency was observed in half of the patients: they showed low aldosterone/renin plasma ratio, lowdailyurinaryaldosteroneexcretionandlowtranstubular potassiumgradient.Inthesamestudy,allpatientshadnormal plasmaADHconcentrations,hyponatremia,andhighurinary osmolality,andmorethanhalfofthepatientshadlowplasma parathyroidhormoneandhypomagnesemia.Inanotherstudy from the same group, of 55 patients with visceral leish-maniasisand20normalindividuals,hyponatremiaandhigh urinary sodium were detected in all patients, suggesting persistent ADH secretionwith noevidence ofextracellular volumedepletion.NormalplasmaADHlevelswereobserved in kala-azarpatients. The syndromeof inappropriate ADH secretioncouldberesponsibleforthesefindings.25Electrolyte
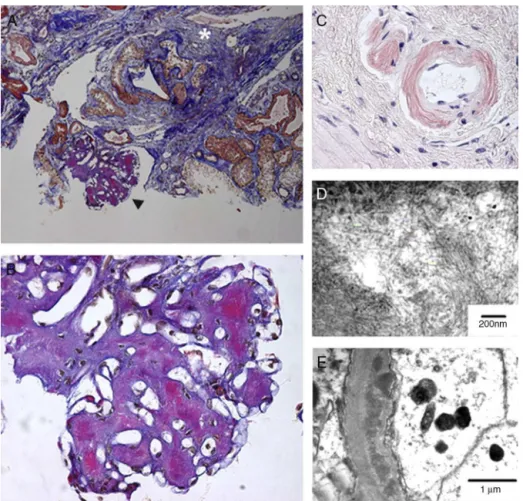
Fig.1–Kidney:glomerulonephritispatternindogswithnaturallyacquiredVL.Histopathology(lightmicroscopy)and ultrastructure.(1)Minorglomerularabnormalities.Glomerular,visceral,andepithelialcellvacuolizationandprotein dropletsinthecytoplasmofthepodocytes(arrow).Footprocesseffacement(arrowhead)canbeseen.EM.Bar=500m;(2)
focal,segmentalglomerulosclerosis.Swellingandeffacementofvisceralandepithelialcellfootprocesses.Absenceof electron-denseparticlesfromtheglomerularcapillarybasementmembrane.EM.Bar=2170m;(3)diffuse,
membranoproliferativeglomerulonephritis.Segmentalthickeningandduplicationoftheperipheralglomerularcapillary wall.PAMS.Bar=25m;(4)diffuse,mesangialproliferativeglomerulonephritis.Normalglomerularcapillarywall.PAMS.
Bar=25m;(5)crescenticglomerulonephritis.FibrocellularorfibrousproliferationoccupyingpartoftheBowman’sspace.
PAMS.Bar=25m;and(6)chronicglomerulonephritis.Intenseactivityoffibroblasts,collagenproliferation,andcell
remnantsininterstitialspace.Bar=350m.
disturbances found in patients with visceral leishman-iasis include hyponatremia (94.6%), hypokalemia (26%), hypochloremia (27.2%), hypocalcemia (32%), and hypomag-nesemia (41.8%).22 Increased urinary excretion fraction of
sodium, potassium,chloride, calcium,inorganic phosphate anduricacidwasfoundinone-thirdofthepatients.Urinary excretionfractionofmagnesiumwashighinallpatients.22
Urinary concentration and acidification defects were also foundinpatientswithvisceralleishmaniasis.26
Therearesomedifferencesbetweenadultsandchildren withvisceralleishmaniasis.Thetimebetweensymptomonset andbeginningoftreatmentisusuallylongerinadults(89.5 vs.48.5days,p<0.001).Treatmentfailurewithglucantimeis morecommoninadults(17.6%vs.8.8%,p=0.008).AKI associ-atedwithvisceralleishmaniasis,whichwasobservedin37% ofcases,ismoresevereinadults.RiskfactorsforAKIinadults werehypokalemia,leukopenia,chillsandamphotericinBuse. Inchildren,secondaryinfectionswerefoundtoincreasethe riskforAKI.27
AKIcan befoundinasignificant proportionofpatients with visceralleishmaniasis.28,29 In a study of 146 children
withvisceralleishmaniasis,AKIwasfoundin45.9%ofcases.
PatientsintheAKIgroupweresignificantlyyounger,andhad jaundiceandsecondaryinfectionsmoreoftenthannon-AKI patients.TheAKIgrouphadsignificantlylowerserumsodium, potassium,andalbuminlevels,elevatedserumglobulinsand amoreprolongedprothrombintime.TheriskfactorsforAKI weresecondaryinfections(OR:3.65,p=0.007),serumalbumin decrement(OR:1.672,p=0.019),andhighserumglobulin(OR: 1.35,p=0.029).28Inastudyof224adultswithvisceral
leish-maniasis, AKIwasobservedin33.9%ofcases,and therisk factorsforAKIweremalegender(OR:2.2;p=0.03),advanced age(OR:1.05;p<0.001),andjaundice(OR:2.9;p=0.002).
Table 1summarizes previous reportsonkidney involve-mentinvisceralleishmaniasis.
Pathophysiology
Mostparasiticdiseasesevolveintochronicillness,with fluc-tuationsinantigenemiaandhostresponse.Thereareseveral possibleexplanations,suchaslownaturalimmuneresponse or the parasite’s abilityto evade the hostimmune system attack. Ithasbeendemonstrated thatdevelopmentofhost resistanceisusuallydependentuponT-CD4+cellsproducing
interferongamma(IFN)–aTH1-typecell.However,amixed TH1andTH2responseseemstobeinvolvedinextracellular parasiteeradication.30 TheLeishmania isabletomanipulate
thehostimmunesystembyinducingtheproductionofgrowth factorb,amacrophage-inhibitingcytokine,and interleukin-10,besidesinterferinginIFN-gammasignaling,allofwhich affectcellularimmuneresponseandinducepolyclonalB-cell activation,whichhasbeenassociatedwithkala-azar glomeru-lardisease.30 Antibodiesproduced inresponse toinfection
canbetrappedinglomerulibydifferentmechanisms, such as immune complexes, in situ development of complexes (antibodieslinkedtopreviouslyimplantedglomerular anti-gens),ordirectlyattachedtoglomerularantigens.Yet,recent studiesdemonstrated that antibodies alone donotexplain theoccurrenceofproteinuria.30,31Macrophages,granulocytes,
andnatural-killerlymphocytesareallpartofhostdefenses, andparticipateinthegenesisofglomerularlesionsthroughan intricatechainofcytokinesandinflammatorymediators,as demonstratedexperimentally.30,31 Itispossiblethatreduced
tubularconcentrationandacidificationfunctionsarecaused byIgGoverloadoftubularcells,inpatientspresentingwith majorchanges in plasma globulin levels.32 Adistal tubule
acidificationdefectcanoccur.
Histopathology
Mesangial proliferative, membranoproliferative, and col-lapsing FSGS seem to be the patterns that are most frequentlyseen inassociation withkala-azar nephropathy, the severityofwhich can vary from mononuclear intersti-tial infiltration to a severe, diffuse, inflammatory infiltrate consistingofmacrophages,lymphocytesandplasmacells.33
On immunofluorescence microscopy,IgG, IgM, IGA and C3 deposits in the mesangial matrix can be found.33
Experi-mentally,tubularandinterstitiallesionshavebeenthemost frequentlyseenkala-azar-associatedkidneylesions.However, amyloiddeposits and rapidly progressive glomerulonephri-tiswithnephroticsyndromehavebeen reportedinhuman leishmaniasis.34,35 ExperimentalinfectionbyL.donovanican
resultinamyloiddeposition,followinganinitiallydiffuse pro-liferativeglomerularlesion.36 Thefindingoftheamastigote
formsinthekidneyisarareevent,yetitispossibletoidentify
Leishmaniaantigensininflammatoryinfiltrate.30Figs.1and2
illustratethepathologicalfindingsinvisceralleishmaniasis.
Treatment
Pentavalent antimonial compounds are still the drugs of choicewhentreatingvisceralleishmaniasis.However, ampho-tericinBmightbeequallyeffective.Kidneyalterationsusually disappearsoonafterinfectioncontrol.
Funding
Elzabeth De Francesco Daher received a grant (number: 300405/2012-0)fromtheBrazilianResearchCouncil(Conselho NacionaldeDesenvolvimentoCientíficoeTecnológico–CNPq; “ProdutividadeemPesquisa”).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MagillAJ.Leishmaniaspecies:visceral(kala-azar),cutaneous, andmucosalleishmaniasis.In:MandellGL,BennettJE,Dolin R,editors.Mandell,Douglas,andBennett’sprinciplesand practiceofinfectiousdiseases.7thed.London:Churchill Livingstone;2009.p.3463–80.
2.ClementiA,BattagliaG,FlorisM,CastellinoP,RoncoC,Cruz DN.Renalinvolvementinleishmaniasis:areviewofthe literature.NDTPlus.2011;4:147–52.
3.OliveiraRA,DinizLF,TeotônioLO,etal.Renaldysfunctionin patientswithAmericancutaneousleishmaniasis.KidneyInt. 2011;80:1099–106.
4.OliveiraRA,LimaCG,MotaRM,MartinsAM,SanchesTR, SeguroAC.Renalfunctionevaluationinpatientswith Americancutaneousleishmaniasisafterspecifictreatment withpentavalentantimonial.BMCNephrol.2012;
13:44.
5.DaherE,SilvaJuniorG,OliveiraJ,etal.Renalabnormalitiesin patientswithAmericancutaneousleishmaniasis[abstract MO226].In:Abstractsfromtheworldcongressofnephrology. 2011.Availablefromhttp://www.abstracts2view.com/wcn [accessedApril2011].
6.BalsanM,FenechF.Acuterenalfailureinvisceral
leishmaniasistreatedwithsodiumstibogluconate.TransR SocTropMedHyg.1992;86:515–6.
7.SampaioRNR,VeigaJPR,LimeiraOM,VexenatA,MarsdenPD. Insuficiênciarenalagudaemleishmaniosetegumentar americanatratadacomassociac¸ãodeglucantime®e alopurinol.AnBrasDermatol.1991;66:133–4.
8.VeigaJPR,KhananR,RosaTT,etal.Pentavalentantimonial nephrotoxicityintherat.RevInstMedTropSãoPaulo. 1990;32:304–9.
9.OliveiraRA,SilvaJuniorGB,SouzaCJ,etal.Evaluationofrenal functioninleprosy:astudyof59consecutivepatients. NephrolDialTransplant.2008;23:256–62.
10.RussoLM,BakrisGL,ComperWD.Renalhandlingofalbumin: acriticalreviewofbasicsconceptsandperspective.AmJ KidneyDis.2002;39:899–919.
11.RoseBD,BakrisGL.Microalbuminuriaandcardiovascular disease.UpToDate12.3;2004.
12.WachtellK,IbsenH,OlsenMH,etal.Albuminuriaand cardiovascularriskinhypertensivepatientswithleft ventricularhypertrophy:theLIFEstudy.AnnInternMed. 2003;139:901–6.
13.WenH,FrokiaerJ,KwonTH,NielsenS.Urinaryexcretionof aquaporin-2inratismediatedbyavasopressin-dependent apicalpathway.JAmSocNephrol.1999;10:1416–29. 14.MartinPY,AbrahamWT,LeimingX,etal.Selective
V2-receptorvasopressinantagonismdecreasesurinary aquaporin-2excretioninpatientswithchronicheartfailure.J AmSocNephrol.1999;10:2165–70.
15.MelbyPC,KreutzerRD,McMahon-PrattD,etal.Cutaneous leishmaniasis:reviewof59casesseemattheNational InstituteofHealth.ClinInfectDis.1992;15:924–37. 16.CucéLC,BeldaJ,DiasW.NephrotoxicytytoGlucantime®in
thetreatmentofleishmaniasis.RevInstMedTropSãoPaulo. 1990;32:249–51.
18.SampaioRNR,PaulaCDR,SampaioJHD,etal.Avaliac¸ãoda tolerânciaenefrotoxicidadedoantimonialpentavalente administradonadosede40mgSbv/kg/diapor30diasna formacutânea-mucosadeleishmaniose.RevSocBrasMed Trop.1997;30:457–67.
19.Mandell:Mandell,Douglas,andBennett’sprinciplesand practiceofinfectiousdiseases.7thed.Philadelphia,PA: ChurchillLivingstoneElsevier;2010.
20.Dantas-TorresF,Brandão-FilhoSP.Visceralleishmaniasisin Brazil:revisitingparadigmsofepidemiologyandcontrol.Rev InstMedTropSãoPaulo.2006;48:151–6.
21.AlbuquerquePL,SilvaJuniorGB,FreireCC,etal.Urbanization ofvisceralleishmaniasis(kala-azar)inFortaleza,Ceará, Brazil.RevPanamSaludPública.2009;26:330–3.
22.LimaVerdeFAA,LimaVerdeFA,DaherEF,SantosGM,Saboia NetoA,LimaVerdeEM.Renaltubulardysfuncioninhuman visceralleishmaniasis(kala-azar).ClinNeprhol.
2009;71:492–500.
23.ElnojomiN,MusaAM,YounisBM,etal.Surrogatemarkersof subtlerenalinjuryinpatientswithvisceralleishmaniasis. SaudiJKidneyDisTranspl.2010;21:872–5.
24.SalgadoFilhoN,FerreiraTMAF,CostaJML.Envolvimentoda func¸ãorenalempacientescomleishmaniosevisceral (calazar).RevSocBrasMedTrop.2003;36:217–21.
25.LimaVerdeFA,LimaVerdeFA,NetoAS,AlmeidaPC,Lima VerdeEM.Hormonaldisturbancesinvisceralleishmaniasis (kala-azar).AmJTropMedHyg.2011;84:668–73.
26.DaherEF,RochaNA,OliveiraMJ,etal.Renalfunction improvementwithpentavalentantimonialagentsinpatients withvisceralleishmaniasis.AmJNephrol.2011;33:332–6. 27.RochaNA,OliveiraMJ,FrancoLF,etal.Comparativeanalysis
ofpediatricandadultvisceralleishmaniasisinBrazil.Pediatr InfectDisJ.2012[Epubaheadofprint].
28.LibórioAB,RochaNA,OliveiraMJ,etal.Acutekidneyinjuryin childrenwithvisceralleishmaniasis.PediatrInfectDisJ. 2012;31:451–4.
29.OliveiraMJC,SilvaJuniorGB,AbreuKLS,etal.Riskfactorsfor acutekidneyinjuryinvisceralleishmaniasis(kala-azar).AmJ TropMedHyg.2010;82:449–53.
30.CostaFA,PriantiMG,SilvaTC,SilvaSM,GuerraJL,GotoH.T cells,adhesionmoleculesandmodulationofapoptosisin visceralleishmaniasisglomerulonephritis.BMCInfectDis. 2010;10:112.
31.PriantiMG,YokooM,SaldanhaLCB,CostaFAL,GotoH. Leishmania(Leishmania)chagasi-infectedmiceasamodel forthestudyofglomerularlesionsinvisceralleishmaniasis. BrazJMedBiolRes.2007;40:819–23.
32.LimaVerdeEM,LimaVerdeFAA,LimaVerdeFA,etal. Evaluationofrenalfunctioninhumanvisceralleishmaniasis (kala-azar):aprospectivestudyon50patientsfromBrazil.J Nephrol.2007;20:432–8.
33.KumarPV,DaneshbodY,SadeghiporrA.Leishmaniainthe Glomerulus.ArchPatholLabMed.2004;128:935–6.
34.NavarroM,BonetJ,BonalJ,etal.Amyloidosissecundariapor leishmaniasisvisceralcomocausadefrecasorenalagudo irreversibleenpacienteconSIDA.Nefrología.2006;26: 745–6.
35.DeVallièreS,MaryC,JonebergJE,etal.AA-amyloidosis causedbyvisceralleishmaniasisinahuman
immunodeficiencyvirus-infectedpatient.AmJTropMedHyg. 2009;81:209–12.
36.OliveiraAV,Roque-BarreiraMC,SartoriA,etal.Mesangial proliferativeglomerulonephritisassociatedwithprogressive amyloiddepositioninhamstersexperimentallyinfectedwith leishmaniadonovani.AmJPathol.1985;120:256–62.
37.DuarteMI,SilvaMR,GotoH,etal.Interstitialnephritisin humankala-azar.TransRSocTropMedHyg.1983;77: 531–7.
38.DutraM,MartinelliR,deCarvalhoEM,etal.Renal involvementinvisceralleishmaniasis.AmJKidneyDis. 1985;6:22–7.
39.CaravacaF,Mu ˜nozA,PizzaroJL,etal.Acuterenalfailurein visceralleishmaniasis.AmJNephrol.1991;11:350–2. 40.LeblondV,BeaufilsH,GinsburgC,etal.Collapsingfocal
segmentalglomerulosclerosisassociatedwithvisceral leishmaniasis.NephrolDialTransplant.1994;9:1353. 41.ChaigneV,KnefatiY,LafargeR,etal.Leishmaniosevisceral
autochtoneavecinsuffisancerénaleaiguëpar glomérulonéphriteinfectieuse.Nephrologie.2004;25: 179–83.
42.EfstratiadisG,BouraE,GiamalisP,etal.Renalinvolvementin apatientwithvisceralleishmaniasis.NephrolDial
Transplant.2006;21:235–6.
43.AlexS,CriadoC,Fernandez-GuerreroML,etal.Nephrotic syndromecomplicatingchronicvisceralleishmaniasis: re-emergenceinpatientswithAIDS.ClinNephrol. 2008;70:65–8.
44.DaherEF,EvangelistaLF,SilvaJuniorGB,etal.Clinical presentationandrenalevaluationofhumanvisceral leishmaniasis(kala-azar):aretrospectivestudyof57patients inBrazil.BrazJInfectDis.2008;12:329–32.
45.DettwilerS,McKeeT,HadayaK,etal.Visceralleishmaniasis inakidneytransplantrecipient:parasiticinterstitial nephritis,acauseofrenaldysfunction.AmJTransplant. 2010;10:1486–9.
46.SuankratayC,SuwanpimolkulG,WildeH,etal.Autochtonous visceralleishmaniasisinahumanimmunodeficiencyvirus (HIV)-infectedpatient:thefirstinThailandandreviewofthe literature.AmJTropMedHyg.2010;82:4–8.