Jebmh.com
Original Article
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 3/Issue 45/June 06, 2016 Page 2236
OSTEOARTHRITIS OF KNEE JOINT AND ITS RISK FACTOR IN POPULATION OF BIHAR
Mahesh Prasad1, Neelu Prasad21Assistant Professor, Department of Orthopaedics, Nalanda Medical College, Patna, Bihar. 2Assistant Professor, Department of Anatomy, Nalanda Medical College, Patna, Bihar.
ABSTRACT
BACKGROUND
In study of Orthopaedic diseases, Osteoarthritis (OA) is one of the most prevalent condition resulting to disability particularly in population of old age people and is a leading cause of chronic disability. The knee is the commonest of the large joints in the body to be affected by Osteoarthritis. Osteoarthritis is a very chronic joint disorder in which there is progressive softening and disintegration of articular cartilage accompanied by new growth of cartilage and bone at the joint margins (Osteophytes) and the capsular fibrosis.
METHODS
A total of 100 cases and 100 controls were taken in the Bihari Population. For each case, an age matched control of same sex was taken, who had no complaints pertaining to knee.
RESULTS
In this study, old age, female sex, obesity, hypertension, family history of knee pain, Indian toilet habits, history of knee trauma/disease, sitting cross-legged for longer period, sitting before Computer for long hours, using cell phone with improper body posture and increased frequency of knee bending were found to be predisposing factors for knee Osteoarthritis.
CONCLUSION
Keeping weight under control, modifying daily habits such as sitting cross-legged and squatting along with using western toilet can significantly reduce the toll of knee osteoarthritis. Any trauma to knee should be dealt with utmost care, so as to maintain joint congruity and to prevent its progression to osteoarthritis in future is also strongly recommended.
KEYWORDS
Osteoarthritis, Risk Factors, Indian Toilet habits, Modern Life Style like Prolonged Mobile and Computer Use.
HOW TO CITE THIS ARTICLE: Prasad M, Prasad N. Osteoarthritis of knee joint and its risk factor in population of Bihar. J. Evid. Based Med. Healthc. 2016; 3(45), 2236-2239. DOI: 10.18410/jebmh/2016/495
INTRODUCTION: Osteoarthritis constitutes a large
proportion of cases attending orthopaedic or rheumatology clinic. Osteoarthritis of knee is one of the five leading causes of physical disability in non-institutionalised elderly men and women. Osteoarthritis is a chronic joint disorder in which there is progressive softening and disintegration of articular cartilage and bone at the joint margins (Osteophytes) and the capsular fibrosis. It is not a purely degenerative disorder and the term “Degenerative Arthritis” which is often used as a synonym for Osteoarthritis is a misnomer. The knee is the commonest of the large joints in the body to be affected by Osteoarthritis. The aim of the study was to evaluate the role of the risk factors responsible for the development of Osteoarthritis of the knee in population of Bihar, India.
Known Risk Factors for the Osteoarthritis Knee:
Primary risk factors for Osteoarthritis knee are genetic predisposition, obesity, age, gender, bone density and
secondary risk factors are previous injury, muscle weakness, joint infection and diet.
There are no published epidemiological studies from the country on Osteoarthritis of the knee. No aetiological factors known to cause this disease are clearly identified. There have been a number of studies implicating various factors like age, sex, obesity, etc. But there is no uniform opinion about the various factors and their pathomechanics. It is in this context that factors responsible for higher prevalence of knee Osteoarthritis in Orientals become necessary so that if some clues about aetiology of the diseases are found, its prevention may be advised.
MATERIAL AND METHODS:
Study Population: Patients who attended Orthopaedics Outpatient Department (OPD) as well as in patient’s admissions in orthopaedic ward of Nalanda Medical College & Hospital, Patna, Bihar. A total of 100 cases and 100 controls were taken for the study.
Selection of Case Inclusion Criteria:
Patients of age group 35 to 75 years of both gender male and female patients.
Clinical as well as radiological evidence of grade II or more osteoarthritis (according to Lawrence and Kellgren) willing to give informed consent.
Financial or Other, Competing Interest: None. Submission 12-04-2016, Peer Review 21-04-2016, Acceptance 16-05-2016, Published 06-06-2016. Corresponding Author:
Dr. Mahesh Prasad,
Aastha Lok Hospital, N/4, Professor Colony, Kankarbagh, Patna-800020, Bihar.
Jebmh.com
Original Article
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 3/Issue 45/June 06, 2016 Page 2237 Exclusion Criteria: Patients not willing to give informed
consent.
Selection of Controls: For each case, an age matched control of same sex was taken, who had no complaints pertaining to knee.
Radiological Examination: All the patients and controls were subjected to radiological examination which consisted of X-rays both knee anteroposterior (AP) weight bearing and lateral (Lat.). The X-rays were then studied for evidence of knee osteoarthritis. The degree of osteoarthritis was graded according to Lawrence and Kellgren criteria as given below: Grade 1: Small Osteophytes of doubtful significance. Grade 2: Definite osteophytes but joint space not impaired. Grade 3: Moderate diminution of joint space.
Grade 4: Extensive loss of joint space with sclerosis of the subchondral bone.
Statistical Analysis: The data thus obtained was analysed so as to find out role of various risk factors in causation of osteoarthritis of the knee, especially in context with its higher frequency in Orientals (racial difference), using statistical method.
OBSERVATIONS:
Age: The maximum number of cases in the study of osteoarthritis falls between age group 50 to 59 years followed by age group of 60 to 69 years, while age group of 70 to 79 years constitutes least number of cases.
Sex: Females constitutes 54% of cases as compared to males 46%.
Economic Class: Majority cases were from middle and lower middle class and there was no significant difference from control group.
History of Smoking: There is higher incidence of osteoarthritis in non-smokers than smokers. 18 out of 100 controls gave history of smoking (18%), whereas 10 out of 100 cases were known smokers (10%).
Alcohol Intake: There was no significant difference
in the alcohol intake among cases and controls.
History of Diabetes: There was no major difference
in prevalence of diabetes among cases and controls and majority of cases were non-diabetics.
History of Hypertension: 50% of cases were
hypertensive as compared to controls among which only 34% patients were hypertensive.
Family History of Knee Pain: 26% of cases had family history of knee pain whereas only 8% of controls had family history of knee pain.
History of Other Joint Pains: Majority of cases had
no history of other joint pains and there was no significant difference between the cases and controls regarding this factor.
Obesity: Majority of cases (78%) were obese or moderately obese as compared to controls (only 42% were obese or moderate obese).
Obesity for More Than 20 Years: 10% of cases had obesity for more than 20 years while only 2% among controls was obese for more than 20 years.
Obesity Increase after Osteoarthritis:
Osteoarthritis did not affect obesity in 96% of cases suggesting that obesity is a cause rather than effect of osteoarthritis knee.
Physical Demand: Most of the cases were
moderate workers and there was no significant difference in physical demand among cases and controls.
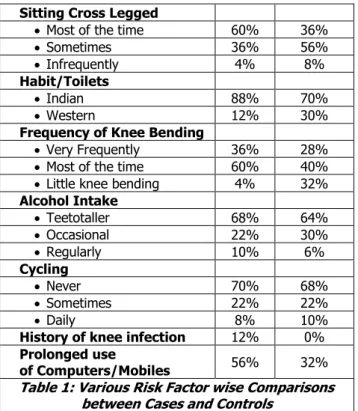
Sitting Cross-Legged: It has significant impact on
development of osteoarthritis. Cases used to sit cross-legged for longer period of time as compared to controls.
Frequency of Knee Bending: 96% of cases used
to bend their knees either most of the time or very frequently while only 68% of controls used to do so. Daily Activities: About 88% of cases were using Indian toilet or had daily activities with Indian habits while about 70% of controls had so.
Cycling: There was no significant difference in the cycling among the cases and controls.
Using Computers/Mobiles: Using computers for
long hours have become a general habit in modern days and one does not maintain the proper posture for long, but there is no significant difference among the cases and controls using computers and mobile phone.
Side of Involvement: Unilateral joint involvement
was more common (62%) as compared to bilateral (38%). Among unilateral cases, right-sided knees were more commonly affected (total 24 cases) than left knees (cases). In bilateral cases, pain used to start more often in right knee than left.
Grading: Most of the cases had grade III or grade
IV osteoarthritis suggesting that they seek medical attention late when the disease has progressed significantly.
Risk Factors Cases Controls
Smoking
Non Smoker 90% 82%
Occasional Smoker 4% 8%
Regular Smoker 6% 10%
Diabetes 14% 12%
Hypertension 52% 34%
Family history of knee pain 26% 8%
History of other joint pain 14% 12%
Obesity
Obese 34% 4%
Moderate Obese 44% 38%
Non Obese 22% 58%
Obesity increases after
Osteoarthritis 4%
Physical Demand
Heavy worker 18% 10%
Moderate worker 70% 80%
Jebmh.com
Original Article
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 3/Issue 45/June 06, 2016 Page 2238 Sitting Cross Legged
Most of the time 60% 36%
Sometimes 36% 56%
Infrequently 4% 8%
Habit/Toilets
Indian 88% 70%
Western 12% 30%
Frequency of Knee Bending
Very Frequently 36% 28%
Most of the time 60% 40%
Little knee bending 4% 32%
Alcohol Intake
Teetotaller 68% 64%
Occasional 22% 30%
Regularly 10% 6%
Cycling
Never 70% 68%
Sometimes 22% 22%
Daily 8% 10%
History of knee infection 12% 0%
Prolonged use
of Computers/Mobiles 56% 32%
Table 1: Various Risk Factor wise Comparisons between Cases and Controls
RESULT: In this study, old age, female sex, obesity, hypertension, family history of knee pain, Indian toilet habits, history of knee trauma/disease, sitting cross-legged for longer period, prolonged use of Computer and Cell Phone with improper body posture and increased frequency of knee bending were found to be predisposing factors for knee Osteoarthritis.
DISCUSSION: Not much work has been done from India,
especially from Bihar to find out the aetiology of this disease which will definitely cripple generations, as life expectancy improves. In the West, primary osteoarthritis of the hip is very common, whereas it is relatively less common in India. One of the important fact which has implicated in different incidence of knee and hip osteoarthritis is activities of daily living, where knee is used in extreme position like squatting, etc. Whereas incidence of osteoarthritis has been shown to increase with age (Felson, et al 1987).1 In this study, the
peak incidence affecting 38% of cases was in the age group of 50 to 59 years.
The male: female ratio has been same as those observed in other studies2 i.e. slight preponderance in
female. In this study, 86% of cases were not diabetics, thereby suggesting that osteoarthritis was not particularly common in diabetics and there was no significant difference between the prevalence of diabetes in case and control group. In this study, cases do have significant higher prevalence of hypertension as compared to their control counterparts (52% of cases were hypertensive).
One of the reasons for this higher prevalence of higher hypertension might be the higher incidence of obesity in case group.
There was positive family history of knee osteoarthritis in 26% of the patients compared to controls, i.e. 8%
suggesting some genetic component behind the
osteoarthritis of knee as was described in earlier studies by
Naeme et al(2004).3 Anderson and Felson
(1988).1,4,5,findings strongly suggested obesity as a cause of
knee osteoarthritis. In this series, 78% had overweight in relation to their age confirming to the other studies. Smoking seems to have protective effect on the pathogenesis of osteoarthritis of knee. 10% of the cases were smokers whereas 18% of controls were smokers. Felson DT (1989).6
in his study suggested that smoking protects against osteoarthritis.
There was no difference of the alcohol intake among cases and controls suggesting that alcohol does not affect the prevalence of osteoarthritis. One important finding of this study was that about 88% of cases used to use Indian Toilet thus by modifying Indian daily habits/toilets, prevalence of osteoarthritis of knee can be decreased. Cycling has no effect on prevalence of osteoarthritis of knee. In previous reports (Kohatsu Neal 1989),7 osteoarthritis was
found to be two or three times more likely in heavy workers than control. Our study showed that moderate workers were affected maximum 70%. Sitting cross-legged and squatting was another factor that had significant impact in the development of osteoarthritis. Vaidya et al (1986)8 study
showed that squatting in the presence of other knee bending activities, knee injury or obesity were the major predisposing factors for osteoarthritis. Jensen LK et al (2000)9 suggests
that work in which a considerable amount of time is spent in knee-straining position may be a risk factor for the development of knee osteoarthritis above the age of 50 years.
Roos (2005).10 suggested joint injury as an important
cause of osteoarthritis knee. Though in most of the cases there was no direct underlying factor for the pathogenesis of osteoarthritis knee; in 6% patients (12% cases), there was history of preceding trauma/infection of knee. Maximum number of cases was in radiological grade III osteoarthritis, suggesting that most of the patients seek attention after the disease has progressed. There are no studies from India to find out possible risk factors that may be operational in causing knee osteoarthritis. This study has tried to evaluate the epidemiology of osteoarthritis and thus to identify the possible risk factors.
SUMMARY AND CONCLUSION: In this study old age,
female sex, obesity, hypertension, family history of knee pain, Indian Toilets/ Habits, history of knee trauma/ disease, sitting cross-legged for longer period, prolonged use of Computer and Cell Phone with improper body posture and increased frequency of knee bending were found to be predisposing factor for osteoarthritis. Diabetes mellitus, history of other joint pains, cycling, alcohol intake had no effect on the prevalence of knee osteoarthritis in study while smoking seems to have protective effect as suggested by decreased prevalence among smokers as compared to non-smokers.
Jebmh.com
Original Article
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 3/Issue 45/June 06, 2016 Page 2239
maintain joint congruity and to prevent its progression to osteoarthritis in future is also strongly recommended.
REFERENCES
1. Felson DT, Allan Nalmerk, Janiffer Anderson, et al. The prevalence of knee osteoarthritis in the elderly. The Framingham osteoarthritis study. Arthritis Rheum 1987;30(8):914-918.
2. Wilson MG, Michael CJ, Ilstrep DM, et al. Idiopathic symptomatic osteoarthritis of the hip and knee: a population bases incidence study. Mayo Clinic Proc 1990:65(9):1214-1221.
3. Neame RL, Muir K, Doherty S, et al. Genetic risk of knee osteoarthritis: a sibling study. Ann Rheum Dis 2004;63(9):1022-1027.
4. Anderson JJ, Felson DT. Factors associated with osteoarthritis of the knee in the first national health and nutrition examinations survey (HANES-1). Evidence for an association with overweight race and physical demand of work. Am J Epidemiol 1988;128(1):179-189.
5. Felson DT. Osteoarthritis. Rheum Dis Clin North Amn 1990:16(3):499-512.
6. Felson DT, Anderson JJ, Nalmerk A, et al. The prevalence of chondrocalcinosis in the elderly and its association with knee osteoarthritis: the Framingham study. J Rheumatol 1989;16(9):1241-1245.
7. Kohatsu ND, Schurman DJ. Risk factors for the development of osteoarthritis of the knee. Clin Orthop Relat Res 1990;(261):242-246.
8. Vaidya Itis S, Ray G, Samant RS, et al. Activity profile in 100 consecutive patients with osteoarthritis of knee. Journals of Indian Rheumatism Association 1996;4(3):88-90.
9. Jensen LK, Mikkelsen S, Lott IP, et al. Radiographic knee osteoarthritis in floor layers and carpenters. Scand J work Environ Health 2000;26(3):257-262. 10. Roos EM. Joint injury causes knee osteoarthritis in