RevBrasAnestesiol.2016;66(5):536---538
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
CLINICAL
INFORMATION
Inappropriate
fixation
of
an
endotracheal
tube
causing
cuff
malfunction
resulting
in
difficult
extubation
Deb
Sanjay
Nag
∗,
Devi
Prasad
Samaddar
DepartmentofAnaesthesiology&CriticalCare,TataMainHospital,Jamshedpur,Jharkhand,India
Received27April2013;accepted10June2013 Availableonline26October2013
KEYWORDS
Endotracheal; Tube; Fixation; Cuff;
Difficultextubation
Abstract Wediscussacaseofdifficultextubation,duetoinadequatedeflationofthetracheal tubecuff,despitecollapseofthepilotballoon,onitsaspiration.Thiswascausedbyinadvertent kinkingofthepilotballoontubingduetoinappropriatetapefixationoftheendotrachealtube. ©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Endotraqueal; Tubo;
Fixac¸ão; Manguito; Extubac¸ãodifícil
Fixac¸ãoinadequadadetuboendotraqueal,resultandoemmaufuncionamento domanguitoeextubac¸ãodifícil
Resumo Relatamosocasodeextubac¸ãodifícildevidoàdesinsuflac¸ãoinadequadadocuffdo tubotraqueal,adespeitodocolapsodobalãopiloto,emsuaaspirac¸ão.Issofoicausadopela torc¸ãoinadvertidadotubocombalãopilotodevidoàfixac¸ãoinadequadodotuboendotraqueal comfitaadesiva.
©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Case
report
A 65-year-old, 60kg hypertensive and diabetic male was scheduled for a laparoscopic cholecystectomy after pre-operative optimizationof diabetes andhypertension from the pre-anesthesia clinic. The patient was premedicated withintravenous midazolam 1mg. After pre-oxygenation,
∗Correspondingauthor.
E-mail:[email protected](D.S.Nag).
anesthesiawasinducedwithintravenousfentanyl100mcg, thiopentonesodium300mgandvecuronium6mg.
Trachealintubationwasaccomplishedsmoothlyusingan 8.5mmcuffedpolyvinylchloridetrachealtube(Apex Endo-tracheal Tube, Apex Laboratories Ltd., Hospital Products Division,India)andfixedwiththinstripsofelasticadhesive bandage(Leukoband,NeptuneOrthopaedics,India). Anes-thesia was maintained with isoflurane, nitrous oxide and oxygen usingthecircle system.The intraoperative period wasuneventful withstablehemodynamicsthroughout the procedure which lastedfor 60min. On completion of the
http://dx.doi.org/10.1016/j.bjane.2013.04.009
0104-0014/©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC
Inappropriatefixationofanendotrachealtube 537
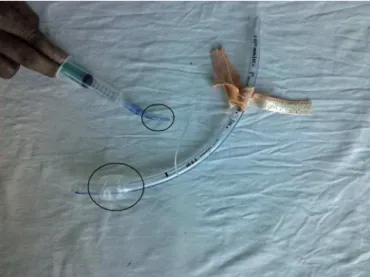
Figure1 Partiallyinflatedcuffwiththecollapsedpilot bal-loon.
Figure2 Kinkonthepilottubingatthepointofinappropriate fixation.
surgery, the neuromuscular blockade was reversed with glycopyrrolate0.5mgandneostigmine2.5mg.Fiveminutes later the patient was awake and responding well to ver-balcommand.Pilotballoonwasdeflatedbeforeattempting extubation. Whileattempting extubation slight resistance wasfelt, but theextubation process wascompleted with additional traction on the tube. Examination of the tube revealedthatcuffwasonlypartiallydeflatedalthoughthe pilotballoonwascompletelycollapsed(Fig.1).Onfurther carefulexamination toidentifythereasonfor this partial deflation,itwasnotedthatthe tubeconnecting thepilot balloon tothe cuffwaskinkedat one point (Fig.2).This kinkingprobablyhadledtopartialdeflationofthe endotra-cheal tubecuff.Cuff wasagainfullyinflated withair and deflatedtoconfirmrecurrenceofpartialdeflation.During thisattempt,thepilotballoonagaingotdeflatedbut cuff remainedpartiallyinflated.
Thepatienthadanuneventfulrecoverywithoutanysore throatandwasdischargedfromthehospitalthenextday. Duringfollow-upoverthenextonemonthattheout-patient
department(OPD),noadverse effectwasreportedbythe patient.
Discussion
Difficultextubation isveryrarely encountered problemin anesthesiapractice,1butforcefulextubationhasbeen
asso-ciatedwithfatality.2 Thisalsohasbeenreportedtocause
vocal cordedema, dislocation of the arytenoids cartilage andlaryngealtrauma.3Difficultextubationsituation
there-foreshouldbehandledwithcautionandcare.
Multiplefactorshadbeenidentifiedasthecauseof diffi-cultextubationsuchasinadvertentfixationofendotracheal tubeorpilotballoontubingwithorofacialsofttissues dur-ingsurgical interventions, tangling of pilot tube withthe nasogastrictubeandmalfunctioningofthecuffassembly.1
Outoftheallthepossiblecauses,cuffmalfunctionhasbeen reportedasthecommonestcauseofdifficult extubation.1
Improper deflation of the tracheal cuff can result from kinkingofthepilottubedistaltothepilotballoon(between balloonandpointofattachmenttotheendotrachealtube) orseveredpilottube atthe pointofattachmentwiththe endotrachealtube.1
Kinking ofthe pilottube had takenplacedistal tothe pilotballooninthecasereportedbyus.Thekinkprevented completedeflationoftheendotrachealtubecuffdespitean apparentlydeflatedpilotballoon.The negativesuction on thepilotballoonallowedthewallsoftheballoontocomein appositiontoeachotherwithoutcompletedeflationofthe cuffand thus prevented the transmission of the negative pressuretothecuff.Thishypothesis wasproved whenwe triedtoreinflatethecufffollowingextubation.Under posi-tivepressurethecuffgotinflated,butonapplyingnegative pressuretheballoongotdeflatedcompletelywhilethecuff stillremainedpartiallyinflated.
Furtherexaminationoftheendotrachealtube revealed thatthekinkhadresulted duetoimproperfixationofthe endotrachealtubewiththeadhesivetapes.Itwasidentified thatthepilottubingwasalsofixedwiththeadhesivetape whilesecuringtheendotrachealtube.Thiscausedthekink andcuffmalfunction,andsimilarmechanismhadonlybeen reportedasthecauseofdifficultextubationintwocasestill date.4,5
Althoughwe hadpulledthetube outby applying addi-tional traction on the tube without any adverse effect, multiplemeasureshadbeensuggested intheliteratureto overcomesuchasituation.Examinationofthepilottubing hasbeensuggestedastheinitialmeasuretoidentify kink-ingof pilottube.6 Insertionof aneedle(withan attached
syringe)distal to the kinked portionhad been advocated asthe nextcorrective measuretodeflatethecuff.6 This,
however,couldbedifficulttoaccomplishandpossibilityof needlestickinjurytotheoperatorandpatientshouldalways beconsideredasapossibility.Alternatively,thetubecanbe pulledoutuntilthecuffisjustvisibleattheunder-surfaceof thevocalcordsfollowedbydeflationofthecuffby punctur-ingitwithasharpobject.7Thismethodalsocarriessimilar
riskofinjurytothepatient.
538 D.S.Nag,D.P.Samaddar
suchmeasurebymentioningthat inflatedcuffhadhelped in removing the secretions from the upper trachea and glottis during the process of extubation.8 However, such
practicehasbeencriticizedforlackofevidenceandbeing ‘‘antitheticaltothestandardpracticeandteachingofthe entire medicalcommunity’’.9 We of course had usedthis
techniquewithoutrealizingthecauseofdifficultextubation atthatpointoftime.
Retrospectively,wefeelthattopreventsuch complica-tion,thepilottube shouldnotbefixed withtheadhesive tape. However this also had been advocated by certain authors and it is a matter of debate.10 ‘‘Thomas
Endo-tracheal Tube Holder (Laerdal)’’ had been suggested as alternative measuretoensure proper fixationof endotra-chealtube. This probably canavoid use oftape andsuch complications.11However,thisisnotastandardpracticeand
thecost effectiveness of such devicesin absence of high levelevidenceisaconcern.
Nodefiniterecommendationcanbegiventomanagesuch situations.Awareness, identification andanalysis of prob-lem, however,can help usin takingone ofthe suggested methodsweighingtheriskbenefitratio.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Nakagawa H, Komatsu R, Hayashi K, et al. Fiberoptic eval-uation of the difficult extubation. Anesthesiology. 1995;82: 785---6.
2.Dryden DE. Circulatory collapse after pneumonectomy (an unusualcomplicationfromtheuseofacatheter):casereport. AnesthAnalg(Cleve).1977;56:451---2.
3.HulmeJ,AgarwalS.Failuretodeflateanendotrachealcuff. ActaAnaesthesiolScand.2008;52:719.
4.TanskiJ,JamesRH.Difficultextubationduetoakinkedpilot tube.Anaesthesia.1986;41:1060.
5.SumanS,GanjooP,TandonMS.Difficultextubationdueto fail-ureofanendotrachealtubecuffdeflation.JAnaesthesiolClin Pharmacol.2011;27:141---2.
6.HartleyM,VaughanRS.Problemsassociatedwithtracheal extu-bation.BrJAnaesth.1993;71:561---8.
7.GuntupalliKK,BouchekCD.Cricothyroidpunctureofan unde-flatableendotrachealtubecuff.CritCareMed.1984;12:924.
8.ShamsaiJ.Anewtechniqueforremovalofendotrachealtube. AnesthAnalg.2006;103:1040.
9.Wax D. Where is the evidence? Anesth Analg. 2007;105:285 [authorreply].
10.AdhikarySD,GeorgeSP,KorulaG.Failureofendotrachealcuff deflation.ActaAnaesthesiolScand.2005;49:590.