1
Effects of electroacupuncture on the BIS and anxiety in anxious volunteers:
a prospective, randomized, blinded study
Silva, N1; Coelho1, R; Liça1, N; Greten J1, Correia, N3 , Rodrigues, A2; Bressan, N2, Amorim2, P
1
Instituto de Ciências Biomédicas Abel Salazar, Universidade do Porto, Portugal
2
Hospital Geral de Santo António, Porto, Portugal;
3
Hospital Geral de São João, Porto, Portugal
ABSTRACT
Introduction Acupuncture is a low-risk intervention that is increasingly used. Some studies examined the
potential clinical effects of acupuncture on anxiety and the bispectral index of the EEG (BIS), used as an objective and indirect measure of anxiolysis. Those studies used the same acupuncture point and achieved conflicting results.
Methods Anxious subjects were recruited for a prospective, controlled and crossover study with random
group allocation. Acupuncture was performed on different sessions at the experimental point He7 (Heart 7) and at a control point Lu 9 (Lung 9). Participants were asked to fill an anxiety visual analog scale (VAS) before and after the acupuncture procedure. BIS was evaluated at 3 different stages, (1) rest state (10 min.) (2) during electro-acupuncture (20min.) (3) post acupuncture (5 min.).
Results Acupuncture significantly decreased self-assessed anxiety levels both on the control and the
experimental group (p=0,002 and p=0,001); however, there was no difference between the groups. Acu-puncture on He7 did not show a significant decrease in BIS values compared to the rest state (89,7 ± 5,0 to 86,5 ± 7,2; p>0,05). However, acupuncture on He7 was related to a significant decrease in BIS values as compared to acupuncture on Lu9 (means: 90,7 ± 4,3 to 86,5 ± 7,2; p=0,009. Minimum BIS was also significantly lower for He7 (80,6 ± 9,6 to 71,9 ± 12,3; p=0,011).
Discussion and Conclusions Acupuncture on He7 was superior over acupuncture on Lu9 to decrease
BIS values in anxious volunteers but it didn’t show to decrease BIS compared to the rest state, possibly due to a high standard deviation. Self-perceived anxiety decreased with acupuncture on both acupunc-ture points. However acupuncacupunc-ture on He7 was not superior to acupuncacupunc-ture on Lu9 in decreasing anxiety VAS scores. Our study found that He7 is another possible point for assessing acupuncture effects on anxiety.
KEYWORDS: acupuncture, bispectral index
of the EEG, electro-acupuncture, anxiety
INTRODUCTION
Acupuncture is increasingly used in western
countries. In France 21% of the population
experienced acupuncture (Fisher, et al.,
1994) (Barnes, et al., 2004) and 20% of
medical doctors in United States and United
Kingdom recommended acupuncture to
their patients (White, et al., 1997).
Acupuncture can be defined as the insertion
of one or more needles on specific points on
the body’s surface with therapeutic means
and originally a part of Traditional Chinese
Medicine (TCM) (Nasir, 2002). Acupuncture
points can be stimulated by electrical
cur-rent, heat, pressure, laser light (Whittaker,
2004) and shockwaves (Everke, 2005).
Acupuncture has the advantages of safety
and low side effects. Severe side effects
occur rarely and are associated with
trau-matic injury of internal organs
(pneumotho-2
rax and cardiac tamponade) and hepatitis C
virus and HIV infection (Ernst, et al., 1997).
Several large prospective studies have
shown that such severe side effects are
extremely rare (White, et al., 2001). It was
also demonstrated that mild and transient
side effects such as pain secondary to
nee-dle insertion and bleeding occurred in
7-11% of all cases (Birch, et al., 2004).
In 1997, the USA National Institute of
Health, declared that acupuncture had
proven benefits for several medical
condi-tions (NIH Consensus Statement Online,
1997) and a review by the World Health
Organization in 2003 concluded that
acu-puncture is efficient in 28 medical conditions
(World Health Organization, 2003). This
document has been criticised as being too
optimistic and not sufficiently supported by
scientific evidence. Some authors claim that
acupuncture is effective in a myriad of
medical conditions while others claim the
opposite. According to Ernst, the evidence
from systematic reviews invalidates both
perspectives (Ernst, 2006) as none of them
takes in account the totality of scientific
knowledge. Moreover there still is a
com-plex issue: the difficulty in implementing an
efficient double-blinded method to perform
well designed controlled studies.
The EEG is used to assess cerebral
func-tion, namely in relation to central nervous
system physiologic alterations (sleep) and
disease. It is also used to assess the effect
of drugs on the brain. Due to the complexity
of the EEG signal, processed indexes
de-rived from the EEG have been introduced in
order to allow clinicians an easier evaluation
of cortical electrical activity. The Bispectral
Index of the EEG (BIS) is the most widely
used of such indexes. In 2004, the FDA
approved the BIS for reducing the incidence
of intra-operative awareness during general
surgery (Joahansen, 2000). Bispectral
analysis employs statistical equations to
study phenomena with nonlinear character,
representing a different description of the
EEG, and it predominantly quantifies the
coherence of different frequencies in the
EEG (Joahansen, 2000).
The BIS algorithm uses a complex formula
that combines several EEG variables into a
single index of hypnotic level with advanced
artefact rejection techniques to define a
dimensionless BIS value from 0 (isoelectric
EEG) to 100 (alert and oriented) that is
rela-tively independent of hypnotic agent
(Joahansen, 2000). BIS monitoring is
mov-ing out of the operatmov-ing room and ICU into
hands of practitioners using conscious
se-dation in a variety of locations (Morse, et al.,
2002) (Overly, et al., 2005)(Miner, et al.,
2003)(Bell, et al., 2004)(Motas, et al.,
2004)(Matsuzaki, et al., 2004)(Coimbra, et
al., 2003).
Our aim was to evaluate acupuncture point
He7 (Heart 7) commonly used for treating
anxiety and it’s possible impact in
decreas-ing subjective anxiety and the Bispectral
Index (BIS) in anxious volunteers,
com-pared to Lu9 (Lung 9), a neutral point,
nor-mally not used for anxiety. Almost all
previ-3
ous studies focused on extra-1 acupuncture
point over subjective anxiety and BIS values
but no published experiment had ever
tested He7 acupuncture point isolated,
al-though many practitioners use this point
frequently in their practice to treat anxiety. A
recent animal experiment showed that
acu-puncture on He7 but not on S36 (Stomach
36) decreased anxious behaviour in anxious
rats (Park, 2005).
In the current experiment we hypothesized
that electro-acupuncture on H7 could
de-crease subjective anxiety and BIS values
comparatively to acupuncture on L9 in
anx-ious subjects.
MATERIAL AND METHODS
Subjects
Participants were recruited among students
present in the premises of the University by
mid afternoon. Potential participants were
asked to fill a questionnaire to assess
whether they were in a state of anxiety.
In-clusion criteria were: age between 18 and
40; being in a state of anxiety. Anxiety was
assessed by a version of Zung Anxiety
Rat-ing Scale gauged for the Portuguese
popu-lation (Serra, et al., 1982) and defined as a
score above 37 (strong suspicion of being
anxious).
All the participants gave their written
in-formed consent. Exclusion criteria were:
cardiac, respiratory, neurological or
psychi-atric disease; pregnancy or lactancy;
anti-coagulant medication,
psychopharmaceuti-cals or regular use of dietetic supplements;
smoking more than 10 cigarettes/day;
hav-ing had a meal or coffee less then 1 hour
previously; having ever been acupunctured
and having needles’ phobia.
Before the experimental procedure,
se-lected subjects filled in a questionnaire to
assess biometric parameters and their
ex-pectations about acupuncture.
Study Design
Nineteen subjects were enrolled in this
pro-spective, crossover experiment. The
proce-dure was briefly outlined and a four-lead
BIS sensor (X4 sensor from ASPECT
Medi-cal provided by the manufacturer for this
study) was placed on the forehead. Blood
pressure and heart rate were also
evalu-ated. Headphones were placed and
non-monotonous solo instrument music was
played along the procedure so that
envi-ronmental sounds would be smoothed but
sleep was not facilitated. From then on any
contact with the participants was made via a
microphone connected to the headphones.
Subjects were asked to answer (yes or no)
to any question made during the procedure
by moving the head. They were asked to
keep their eyes closed and to lye still.
The experimental procedure was composed
of 3 parts: (1) the stabilization period,
corre-sponding to the first 10 minutes, so that a
baseline could be established for posterior
comparisons; (2) the acupuncture period,
when a needle was inserted in the control or
the experimental point and stimulated by
electrical current during 20 minutes (3) the
4
post-acupuncture period, when the electrical
current was switched off and the recordings
continued for 5 minutes more.
Subjects were assessed their level of
anxi-ety by means of a visual analog scale (VAS)
with maximum serenity on one extreme and
maximum anxiety on the other
(correspond-ing to a 0 and 10 score, respectively); this
evaluation was performed twice: right
be-fore the experimental procedure and at the
end. After the acupuncture session,
partici-pants filled a questionnaire about biometric
parameters, and stated their perception of
whether the control or experimental point
was used and also if he/she had fall asleep.
At least 1 week later, the subjects returned
to repeat the procedure but this time on the
experimental or on the control acupuncture
point, whether acupuncture was applied on
the control or on the experimental point in
the previous session. In order to ensure
participants commitment for the 2 sessions
a monetary incentive was offered.
Acupuncture
Acupuncture was performed by
post-graduates in Traditional Chinese Medicine
at the Biomedical Sciences Institute Abel
Salazar – University of Porto (ICBAS-UP),
Portugal. They all had an education session
about He7 and Lu9 location and needle
insertion technique with Henry J. Greten,
M.D., DGTCM Chairman (Deutsche
Gesell-schaft für Traditionelle Chinesische Medizin)
and the TCM Post-graduation Chairman at
ICBAS-UP.
He7 was the experimental point and is
lo-cated on the wrist crease, in the medial
side, in a small depression just lateral to the
pisiform bone. Lu9, the control point,
thought to have a neutral action on anxiety,
is located also in the wrist crease, laterally
to the radial artery. The EA was applied
unilaterally.
Acupuncture points stimulation was
per-formed with electrical current
(electro-acupuncture).
Electro-acupuncture
(EA)
was chosen for 3 reasons mainly: first, it is
measurable and reproducible; second, it
has been shown to produce a stronger
ef-fect than manual acupuncture although for
other purposes (Ulett, et al., 1998); also, it
allows a continuous and stable stimulation
for any period of time.
The decision on what point to acupuncture
first, the control point or the experimental
point, was randomly made by the
acupunc-turist by coin flip. The selected point was
then registered using an alphabetical code,
so that all other investigators who analyzed
the data did not know to which group
(con-trol or experimental) it corresponded. Only
after the end of the entire study did the
acu-puncturists reveal the codification key. The
acupuncturist and the researcher controlling
data capture were separated by a screen,
so that the acupuncturist could not see the
BIS values and the staff person collecting
the data could not see which point was
be-ing acupunctured.
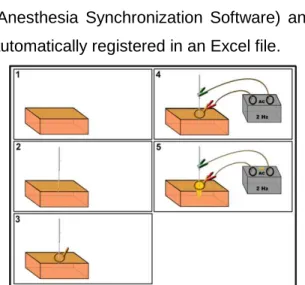
A device was created to effectively apply
the stimulation only to the point being
ana-5
lyzed (Fig. I). Once the device was in place,
EA with continuous waves, 2Hz and
10-50mA was started and the subject was
asked to tell when an electrical sensation
was felt. From then on, each 5 minutes, the
acupuncturist increased the current slightly.
Stainless
needles
were
used,
0,25mmx25mm and the EA device was the
Multi-Purpose Health Device, KWD-808.
Electrical current frequency and intensity
were calibrated with a multimeter Meterman
37XR(True RMS).
Data collection
BIS values were assessed using a Model
A-2000™ (Aspect Medical Systems, Inc.,
Na-tick, MA) 4.0 software version. BIS data was
captured and synchronized each 5 seconds
through ASYS (Bressan, et al., 2008)
(Anesthesia Synchronization Software) and
automatically registered in an Excel file.
Fig. I – EA device (1) Skin’s scheme (2) Needle insertion on the acupuncture point (3) Placement of a copper ring around the needle (attached to the skin with adhesive, not shown in the illustra-tion) (4) Electrodes attachment to the needle and copper ring (5) Electrical current initiation. The light gray triangle is the most probable elec-trical current flow representation.
Blood pressure was assessed twice, one 5
minutes after the start of the experiment and
the other at the end of the Pos-Acupuncture
period. Heart rate was assessed each 2
minutes. Both heart rate and blood pressure
were manually registered.
Statistical Analysis
Data are presented as mean ± standard
deviation. Intra-session and inter-session
group comparisons were done with the
Wil-coxon signed-rank test. P<0,05 was
as-sumed as significant.
RESULTS
For BIS analysis, 3 time frames were
con-sidered. First, the basal status was defined
as the 5 minutes that preceded
acupunc-ture; second, acupuncture period
corre-sponded to the total electro-acupuncture
time less the 2 initial minutes (18 minutes)
as needle insertion distorts the BIS pattern;
third, the 5 minutes measurements after
electrical-current was switched off was
con-sidered to be the post-acupuncture period.
Nineteen subjects were recruited for the
study but 4 were eliminated due to BIS data
acquisition abnormalities. From the 15
sub-jects under analysis, 10 were female and 5
were male; mean BMI was 21,1 ± 2,1, mean
age was 21,6 ± 2,4 and mean Zung’s
Anxi-ety Rating Scale score was 41 ± 4,7; all
were Caucasian.
We did not find significant correlation
be-tween acupuncture expectations, Zung’s
scale score and self-perceived group
alloca-tion compared to BIS variables. Also,
blood pressure and heart rate changes had
6
no correlation with self-perceived anxiety or
BIS values.
BIS missing values were replaced using a
linear interpolation method.
For the effects of acupuncture on the BIS
and anxiety VAS, the within analysis refers
to comparisons between the acupuncture
period and the rest state; the between
analysis refers to comparisons of
acupunc-ture period on the experimental point over
acupuncture period on the control point, so
that we could compare if there was a
signifi-cant difference of acupuncture on He7 over
acupuncture on Lu9. Basically, within
analy-sis refers to an intra-session analyanaly-sis and
between to an inter-session analysis.
Anxiety VAS scores were significantly lower
in both groups after acupuncture (table 1).
However, no significant difference was
found between acupuncture on He7 and
Lu9, represented as the percent decrease in
VAS scores after acupuncture compared to
VAS before acupuncture between groups.
Table 1 - VAS Comparison within groups Before A vs After A Before B vs After B
3,83 ± 2,01 2,32 ± 1,62 3,60 ± 1,89 1,79 ± 1,37
p=0,002 p=0,001
VAS between groups B and A
-39,9% ± 27,5 -40,5% ± 59,8
p>0,05
For BIS, the within analysis showed no
sig-nificant differences, comparing the
acupunc-ture with the rest state on both the
experi-mental and the control group. Also, there
was no significant relation when comparing
BIS in the post acupuncture period and the
rest state (table 2).
Table 2 – BIS Comparison within group
Rest A vs Acup A Rest B vs Acup B Rest B vs PosAcup B
89,3 ± 5,6 90,7 ± 4,3 89,7 ± 5,0 86,5 ± 7,2 89,3 ± 5,6 88,8 ± 5,9
p>0,05 p>0,05 p>0,05
Between analysis showed a significant
de-crease of BIS values during acupuncture on
the experimental point (He7) compared to
the control point (Lu9), but this difference
was lost during the 5 minutes after current
was switched off (post-acupuncture period).
A corrected between analysis was
per-formed so that before BIS averages were
compared between control and
experimen-tal groups, corrected to the respective rest
state. The corrected between analysis also
showed a significant decrease upon
acu-puncture on He7 compared to acuacu-puncture
on Lu9, (table 3). BIS minimum values were
identified and compared between the
expe-rimental and the control groups:
significant-ly lower BIS minimum values were found
with acupuncture on He7 in comparison to
acupuncture on Lu9 (table3).
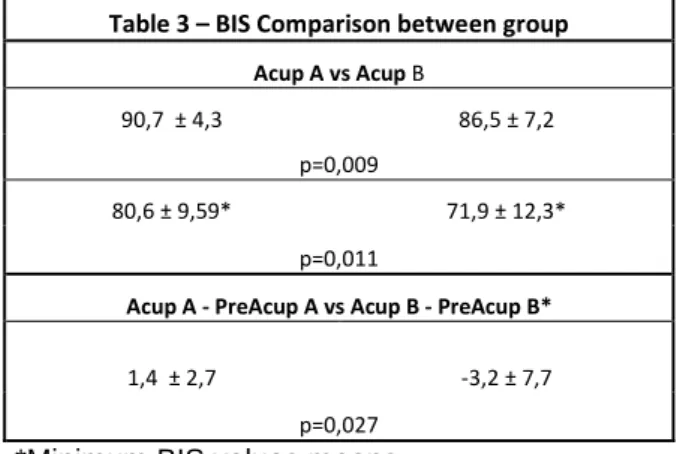
Table 3 – BIS Comparison between group Acup A vs Acup B
90,7 ± 4,3 86,5 ± 7,2
p=0,009
80,6 ± 9,59* 71,9 ± 12,3*
p=0,011
Acup A - PreAcup A vs Acup B - PreAcup B*
1,4 ± 2,7 -3,2 ± 7,7
p=0,027
*Minimum BIS values means
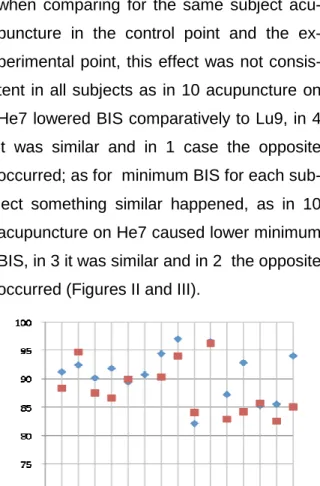
The average BIS and the minimum BIS for
each subject for acupuncture on He7 and
Lu9 were evaluated. Although there was a
significant decrease in overall average BIS,
7
when comparing for the same subject
acu-puncture in the control point and the
ex-perimental point, this effect was not
consis-tent in all subjects as in 10 acupuncture on
He7 lowered BIS comparatively to Lu9, in 4
it was similar and in 1 case the opposite
occurred; as for minimum BIS for each
sub-ject something similar happened, as in 10
acupuncture on He7 caused lower minimum
BIS, in 3 it was similar and in 2 the opposite
occurred (Figures II and III).
Figure II – Individual BIS means for the control (lozenges) and acupuncture group (squares). The x axis represents the subject’s code number and the y axis the BIS.
Graph III – Individual BIS minimums for the con-trol (lozengues) and acupuncture group (squares). The x axis represents the subject’s code number and the y axis the BIS.
Figure IV - Mean BIS values over time for the control point (Lu9) and experimental point (He7). Note the significant difference between acu-puncture on the He7 (light gray) and on P9 (dark grey), and the non-significant difference be-tween the acupuncture period (Acupuncture) and the rest state (Rest) within He7 (light gray). The thin lines represent polynomial regression lines for each group.
DISCUSSION
Our study focused on anxious subjects in
order to assess a clinically relevant
popula-tion.
After a careful analysis of the studies on
acupuncture, BIS and anxiety we tried to
improve some methodological issues in
terms of objectivity and reproducibility.
Since manual acupuncture and acupressure
are difficult in terms of standardization of
frequency and pressure amount during a
period of time we chose to use
electro-acupuncture, which can be applied with a
certain frequency and current intensity that
can be easily reproduced by others and
minimizes acupuncturists possible bias In
order to be able to precisely apply the
cur-rent to the desired acupuncture point we
built and used a simple device in which a
copper ring is placed around the needle and
electrodes were connected to both, inducing
current flow in the direction of the
acupunc-8
ture point. Previous studies used manual
recording of BIS; since BIS is updated every
second and variability is present, we
per-formed BIS data acquisition and
synchroni-zation from the BIS monitor using a new
software (ASYS) that we helped develop,
which allowed automatic recording of BIS
values every 5 seconds during the entire
procedure.
A crossover design was implemented to
eliminate inter-individual variability when
comparing control point versus the
experi-mental point, also representing a
methodo-logical improvement in comparison to
previ-ous studies.
Although control and experimental points
significantly decreased self-perceived
anxi-ety, acupuncture on He7 didn’t show
supe-rior benefit over acupuncture on Lu9. This
fact may be interpreted as proof that
acu-puncture in itself may lower anxiety levels,
but that stimulation of a point specific for
anxiety (He7), as a demonstrable and
measurable cerebral effect. The BIS levels
achieved with stimulation of He7 are the
values observed when pharmacological
sedation is performed.
Because of difficulties in assessing anxiety
levels in individuals and due to many
possi-ble bias and confounding variapossi-bles when
performing anxiety tests, we evaluated the
BIS as it is being increasingly used as an
indirect measure of anxiety levels and
seda-tive interventions, in which anxiolysis
corre-sponds to a milder form of sedation. BIS
absolute means and minimums means were
significantly reduced by acupuncture on
He7 compared to acupuncture on Lu9. In
the meanwhile, none of the acupuncture
groups showed a significant decrease in
BIS means when comparing the
acupunc-ture period to the rest state. However it
should be noted that acupuncture on He7
was related to a relevant (but
non-significant) decrease in BIS means
com-pared to the rest state but with a high
stan-dard deviation. A larger sample could
pos-sibly have shown a statistical significant
difference.
Another interesting finding was that
acu-puncture on He7 did not produce consistent
effects on all the individuals, showing a
variable response between subjects to
acu-puncture.
Immediately after electrical current was
switched off and BIS values were recorded
for 5 more minutes, the post-acupuncture
period, the BIS normalized to values similar
to the rest state, showing that the decrease
of BIS values with acupuncture on He7
compared to acupuncture on Lu9 dissipated
after the current was switched off.
Regarding possible mechanisms that
under-lie the effect of He7 acupuncture on anxiety
and BIS, current research is very insufficient
to give a satisfactory answer. Most of the
research on acupuncture focused on
anal-gesic properties and underlying
mecha-nisms, consistently showing that endorphins
play an essential role in mediating the
anal-gesic effect of acupuncture and
electro-acupuncture (Han, 2004). In the meanwhile,
9
previous studies showed that the effect of
extra-1 point acupuncture on BIS and
sub-jective anxiety was not related to a change
in β-endorphin and melatonin plasma levels
(Fassoulaki, et al., 2007). Consistent with
this findings is preliminary evidence
demon-strating that remifentanil, an opioid, even at
large doses, produced no modification of
BIS (Hans, et al., 2000) (Guignard, et al.,
2000)(Koitabashi, et al., 2002).
The only experiment addressing the effects
of acupuncture on He7 was performed in
maternally separated rats, a model for
anxi-ety studies in rats, showed a decrease in
anxious behaviour and a correspondent
increase in the expression of neuropeptide
Y in the basolateral amygdale, compared to
acupuncture on S36 (stomach 36). Those
findings suggested that acupuncture
treat-ment might reduce anxiety-like behaviour in
adult rats following maternal separation by
modulating the NPY system in the
amyg-dale (Park, 2005).
Furthermore, stimulation frequency is a
de-terminant factor in electro-acupuncture as
different frequencies correlate with different
neurotransmitters and hormones secretion
(Han, 2003)(Iverfeldt, 1989)(He, et al.,
1990)(Racke, 1989)(Frank, 1993).
In conclusion, our results demonstrate that
low-frequency electro-acupuncture on He7
significantly, decreased the Bispectral Index
of the EEG (BIS) when compared to
acu-puncture on Lu9 Acuacu-puncture on He7 was
related to a larger BIS mean variation (90,7
± 4,3 to 86,5 ± 7,2) than did a 10mg single
dose of diazepam (96.1±1.8 to 93.5±3.5)
compared to control groups (Hirota, et al.,
1999)
LIMITATIONS
AND
FUTURE
PERSPECTIVES
Acupuncture on He7 can be of therapeutical
usefulness in the future, constituting an
al-ternative or complement to current anxiolytic
therapies. Moreover acupuncture is a very
low risk technique with minimal interactions,
making it suitable to be used in almost any
patient and it is a low cost intervention. In
the meanwhile, further research is needed,
to evaluate it’s efficacy in different and
lar-ger samples as well as to clarify the
under-lying mechanisms (Birch, et al., 2004). It
could also be interesting to study the effects
of He7 acupuncture compared to a
conven-tional therapy like an anxiolytic drug on the
BIS and subjective anxiety perception.
Acupuncturist blinding difficulties remains a
major methodological concern and a
possi-ble source of significant bias. The current
study, although patient blinded and
re-searchers blinded, didn’t eliminate this
fac-tor as well as almost all other acupuncture
studies in humans. Also, the sample size
was small and further studies could address
this issue on a bigger sample as well as
assessing variable responses between
indi-viduals to acupuncture and the underlying
causes.
10
AKNOWLEDGEMENTS
Special thanks to everyone who contributed
to this research: Ana Castro, Rui Oliveira,
Carlos Ferreira, Jaime Babulal and Florian
Beissner.
BIBLIOGRAPHY
Barnes PM [et al.] Complementary and
alternative medicine use among adults: United States [Journal] // Advance Data from Vital and Health Statistics. - 2004. - 343. - p. 1.
Bell J K, Laasch H U and Wilbraham L et al
Bispectral index monitoring for conscious sedation in intervention: better, safer, faster [Journal] // Clinical Radiology. - 2004. - 59. - pp. 1106–1113.
Birch S [et al.] Clinical research on acupuncture: Part 1. What have reviews of the efficacy and safety of acupuncture told us so far? [Journal] // Journal of Alternative and Complementary Medicine. - 2004. - 10. - pp. 468-80.
Bressan N [et al.] Automation in Anesthesia:
Computer controlled propofol infusion and data acquisition [Conference] // Proceedings of the 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS'08 - "Personalized Healthcare through Technology". - 2008. - pp. 5543-5547. - 4650470.
Coimbra C, Choiniere M and Hemmerling T M
Patient-controlled sedation using propofol for dressing changes in burn patients: a dose-finding study [Journal] // Anesthesia & Analgesia. - 2003. - 97. - pp. 839-842.
Ernst E Acupuncture - a critical analysis
[Journal] // Journal of Internal Medicine. - 2006. - 259. - pp. 125-137.
Ernst E and White A Life-threatening adverse
reactions after acupuncture? A systematic review [Journal] // Pain. - 1997. - 71. - pp. 123-6.
Everke H Die Stosswellenakupunktu [Journal] //
Dtsch Z Akup. - 2005. - 48. - pp. 12-21.
Fassoulaki A [et al.] Acupressure on the
Extra-1 Acupoint: The effect on Bispectral Index, Serum Melatonin, Plasma beta-endorphin and stress [Journal] // Anesthesia and Analgesia. - 2007. - 104. - pp. 312-7.
Fisher p and Ward A Complementary Medicine
in Europe [Journal] // BMJ. - 1994. - 309. - pp. 107-11.
Frank J et al Differential release od endogenous 5-hydroxy-tryptamine, substance P, neurokinin A from rat ventral spinal cord in respond to electrical stimulation [Journal] // J Neurochem. - 1993. - 61. - pp. 704-11.
Guignard B, Menigaux C and Dupont X et al
The effect of remifentanil on the bispectral index change and hemodynamic responses after orotracheal intubation [Journal] // Anesthesia & Analgesia. - 2000. - 91. - pp. 161-67.
Han Ji-Sheng Acupuncture and endorphins
[Journal] // Neuroscience Letters. - 2004. - 361. - pp. 258-261.
Han Ji-Sheng Acupuncture: neuropeptide
release by electrical stimulation of different frequencies [Journal] // Trends in Neurosciences. - 2003. - 1 : Vol. 26.
Hans P, Bonhomme V and al Born J D et
Target-controlled infusion of propofol and remifentanil combined with bispectral index monitoring for awake craniotom [Journal] // Anaesthesia. - 2000. - 55. - pp. 255-259.
He C M and Han J S Attenuation of low rather
11
following microinjection of beta-endorphin antiserum into the periaqeductal gray in rats [Journal] // Acupunct. Sci. Int. J.. - 1990. - 1. - pp. 94-99.Hirota K and Matsunami K Relation between
bispectral index and plasma cathecolamines after oral diazepam premedication [Journal] // European Journal of Anaesthesiology. - 1999. - 16. - pp. 516-518.
Iverfeldt K et al Differential release of
coexisting neurotransmitters: frequency dependence of the efflux of substance P, thyrotropin releasing hormone and serotonin from tissue slice of rat ventral cord [Journal] // Acta Physiologica Scandinavia. - 1989. - 137. - pp. 63-71.
Joahansen W Update on Bispectral Index
monitoring [Journal] // Best Practice & Research Clinical Anestesiology. - 2000. - 1 : Vol. 20. - pp. 81-99.
Koitabashi T, Johansen J W and Sebel P
Remifentanil dose/electroencephalogram bispectral response during combined propofol/regional anesthesia [Journal] // Anesthesia & Analgesia. - 2002. - 94. - pp. 1530-1533.
Matsuzaki S and Tanaka H The feasibility of
bispectral index monitoring for intravenous sedation during dental treatment [Journal] // Anesthesia Progress. - 2004. - 51. - pp. 52-55.
Miner J R [et al.] Bispectral
electroencephalographic analysis of patients undergoing procedural sedation in the emergency department [Journal] // Academic Emergency Medicine. - 2003. - 10. - pp. 638-643.
Morse Z [et al.] BIS monitoring during
midazolam and midazolam-ketamine conscious intravenous sedation for oral surgery [Journal]. - [s.l.] : Oral Surgery, Oral Medicine, Oral
Pathology, Oral Radiology, & Endodontics, 2002. - 94. - pp. 420-424.
Motas D [et al.] Depth of consciousness and
deep sedation attained in children as administered by nonanaesthesiologists in a children’s hospital [Journal] // Paediatric Anaesthesia. - 2004. - 14. - pp. 256-260.
Nasir LS Acupuncture [Journal] // Primary Care
Clinical Office Practice. - 2002. - 29. - pp. 393-405.
NIH Consensus Statement Online
Acupuncture. - November 3-5, 1997. - Vol. 15. - pp. 1-34.
Overly F L, Wright R O and al Connor F A et
Bispectral analysis during deep sedation of pediatric oral surgery patients [Journal] // Journal of Oral & Maxillofacial Surgery. - 2005. - 63. - pp. 215–219.
Park Hi-Joon et al The effect of acupuncture on
anxiety and neuropeptide Y expression in the basolateral amygdala of maternally separated rats [Journal] // Neuroscience Letters. - 2005. - 377. - pp. 179-184.
Racke K et al frequency-dependent effects of
activation and inhibition of protein kinase C on neurohypophysial release of oxytocin and vasopressin [Journal] // Naunyn Schmiedebergs Arch Pharmacol. - 1989. - 339. - pp. 617-624.
Serra A V, Ponciano E and relvas J Aferição
da escala de auto-avaliação de ansiedade, de Zung, numa amostra da população portuguesa - II - Sua avaliação como instrumento de medida [Journal] // Psiquiatria Clínica. - 1982. - 4 : Vol. 3. - pp. 203-213.
Sleigh et al The Bispectral index: a measure of
depth of sleep? [Journal] // Anesthesia and Analgesia. - 1999. - 88. - pp. 659-61.
Ulett Georges A, Han Songping and Han Ji-Sheng Electroacupuncture: Mechanisms and
12
Clinical Application [Journal] // Biological Psychiatry. - 1998. - 44. - pp. 129-138.White A, Hayhoe S and Hart A Ernst, E
Adverse events following acupuncture: prospective survey of 32000 consultations with doctors and physiotherapists [Journal] // British Medical Journal. - 2001. - 323. - pp. 485-486.
White AR and Resch KL Ernst, E
Complementary Medicine: use and attitudes among general practitioners [Journal] // Family Practice. - 1997. - Vol. 14. - pp. 302-6.
Whittaker P Laser Acupuncture: past, present
and future [Journal] // Lasers Medical Science. - 2004. - 19. - pp. 69-80.
World Health Organization Acupuncture:
Review and analysis of reports on controlled clinical trials . - 2003.