Diagnosing human asymptomatic visceral leishmaniasis
in an urban area of the State of Minas Gerais, using
serological and molecular biology techniques
Diagnóstico da leishmaniose visceral humana assintomática
em uma área urbana do Estado de Minas Gerais, usando
métodos sorológicos e biologia molecular
Elizabeth Castro Moreno
1, Maria Norma Melo
2, José Roberto Lambertucci
3,
José Carlos Serufo
3, Antero S.R. Andrade
4, Carlos Maurício F. Antunes
5Odair Genaro† and Mariângela Carneiro
2ABSTRACT
A po pulatio n-b ase d c r o ss-se c tio nal study was se t up in Sab ar á c o untr y, So uthe aste r n B r azil, to ide ntify asympto matic human visc e r al le ishmaniasis in an ur b an ar e a o f lo w dise ase pr e vale nc e . B lo o d was c o lle c te d o n filte r pape r ( n= 1 ,6 0 4 inhab itants) and examined b y indir ec t immuno fluo r esc ent test, enzyme-link ed immuno so r b ent assay and immuno c hr o mato gr aphic str ip te st. The pr e vale nc e r ate s o f infe c tio n r ange d fr o m 2 .4 to 5 .6 % de pe nding o n the te st use d. One ye ar late r, ve no us b lo o d was c o lle c te d in a sub se t o f 2 2 6 par tic ipants ( 1 0 2 se r o po sitive and 1 2 4 se r o ne gative ) . The te sts pe r fo r me d we r e IFAT, ELISA, r k 3 9 -ELISA, po lyme r ase c hain r e ac tio n and hyb r idizatio n with Le ishmania do no vani c o mple x pr o b e . No c linic al signs o r sympto ms of leishmaniasis were observed. Using hybridization as a referenc e test, the sensitivity and spec ific ity of serology were respec tively: 2 4 .8 and 7 1 % ( ELISA) ; 2 6 .3 and 7 6 .3 % ( r k -3 9 ) ; 3 0 .1 and 6 3 .4 % ( IFAT) . Due to disagr e e me nts, diffe r e nt c r ite r ia we r e te ste d to de fine the infe c tio n and hyb r idizatio n sho uld b e c o nside r e d in e pide mio lo gic al studie s.
Ke y- wo r ds: Asympto matic visc e r al le ishmaniasis. Le ishmania c hagasi. Pr e vale nc e r ate . Diagno stic . Hyb r idizatio n.
RESUMO
Um e studo se c c io nal de b ase po pulac io nal fo i de se nvo lvido no munic ípio de Sab ar á, r e gião sude ste do B r asil, par a ide ntific ar a le ishmanio se visc e r al humana assinto mátic a e m uma ár e a ur b ana de b aixa pr e valê nc ia da do e nç a. Fo i c o le tado sangue e m pape l filtr o ( n= 1 .6 0 4 mo r ado r e s) , se ndo e xaminado s pe la r e aç ão de imuno fluo r e sê nc ia indir e ta, e nsaio imuno e nzimátic o e te ste imuno c r o mato gr áfic o ( str ip te st) . As taxas de pr e valê nc ia da infe c ç ão var iar am de 2 ,4 a 5 ,6 % , de pe nde ndo do te ste utilizado . Um ano de po is fo i c o le tado sangue ve no so de um sub gr upo de 2 2 6 par tic ipante s ( 1 0 2 so r o po sitivo s e 1 2 4 so r o ne gativo s) . Os te ste s r e alizado s fo r am IFAT, ELISA, r k 3 9 -ELISA, r e aç ão e m c ade ia da po lime r ase e hib r idizaç ão c o m so nda e spe c ífic a par a o c o mple xo Leishmania do no vani. Não fo i o b ser vado nenhum sinal c línic o o u sinto ma de leishmanio se. Usando a hib r idizaç ão c o mo te ste de r e fe r ê nc ia, a se nsib ilidade e e spe c ific idade do s te ste s so r o ló gic o s fo r am, r e spe c tivame nte : 2 4 .8 e 7 1 % ( ELISA) ; 2 6 ,3 e 7 6 ,3 % ( r k 3 9 -ELISA) ; 3 0 ,1 e 6 3 ,4 % ( IFAT) . De vido a disc o r dânc ias, dife r e nte s c r ité r io s fo r am te stado s par a de finir a pr e se nç a da infe c ç ão e a hib r idizaç ão de ve r ia se r c o nside r ada e m e studo s e pide mio ló gic o s.
Pa la vr a s- cha ve s: Le ishmanio se visc e r al assinto mátic a. Le ishmania c hagasi. Taxa de pr e valê nc ia. Diagnó stic o . Hib r idizaç ão .
1 . Fundaç ão Nac io nal de Saúde, B elo Ho r izo nte, MG. 2 . Depar tamento de Par asito lo gia do Instituto de Ciênc ias B io ló gic as da Univer sidade Feder al de Minas Ger ais, B elo Ho r izo nte, MG. 3 . Depar tamento de Clínic a Médic a da Fac uldade de Medic ina da Univer sidade Feder al de Minas Ger ais, B elo Ho r izo nte, MG. 4 . Co missão Nac io nal de Ener gia Nuc lear do Centr o de Desenvo lvimento da Tec no lo gia Nuc lear, B e lo Ho r izo nte , MG. 5 . Santa Casa de B elo Ho r izo nte, B elo Ho r izo nte, MG.†In me mo r iam. Par tially suppo r te d b y Ministr y o f He alth, B r azil, Pr o j e c t Vigisus, Co nse lho Nac io nal de De se nvo lvime nto Cie ntífic o e Te c no ló gic o , Fundaç ão de Ampar o a Pe sq uisa de Minas Ge r ais and UNICEF/UNDP/Wo r ld B ank /WHO Spe c ial Pr o gr amme fo r Re se ar c h and Tr aining in Tr o pic al Dise ase s ( TDR) .
Addr e ss to: Dr ª Mar iânge la Car ne ir o . De ptº de Par asito lo gia/ICB /UFMG. Av. Antô nio Car lo s 6 6 2 7 , Caixa Po stal 4 8 6 , 3 1 2 7 9 -9 0 1 B e lo Ho r izo nte , MG. B r asil. Te l: 5 5 3 1 3 4 9 9 - 2 8 3 9 ; Fax: 5 5 3 1 3 4 9 9 - 2 8 6 0
Mo r e no EC e t a l
Visc eral leishmaniasis ( VL) in Latin Americ a is c aused by Leishmania ( L.) chagasi, a protozoan belonging to the Leishmania donovani complex, mainly transmitted by a sand fly, Lutzomyia longipalpis. Dogs are considered as the principal parasite reservoir, playing a central role in the transmission cycle to humans. VL is endemic in the rural areas of most Northeastern Brazilian states. It is nowadays considered as a reemerging infection due to its rapid expansion to non-endemic areas. During the last decade, VL c linic al c ases and deaths have been repo rted in inc reasing numbers, in large cities located in different Brazilian states3 1 3 4.
The o c c ur r e nc e o f individuals har b o r ing asympto matic o r o ligo sympto matic L. c hagasi infe c tio ns in B r azil witho ut pr o gr essio n to the disease has been r epo r ted in investigatio ns c o nduc te d in No r the aste r n B r azil3 4 6 1 1 1 3 1 4 1 6 1 7 1 8. One o f the
mo st impo r tant dr awb ac k s in the se studie s is the diffic ulty o f diagno sing patie nts in this phase , b e c ause o f the lo w le ve l o f antib o die s and r e duc e d par asite numb e r s2 2 5 2 7.
Population-based studies in urban areas are scarce and, when c arried out, use immunologic al tests, mainly the enzyme-linked immuno so r bent assay ( ELISA) , indir ec t immuno fluo r esc ent antibody test ( IFAT) ; tests that present high sensitivity for disease, but do not disc riminate between past and c urrent infec tion; and the skin-test, positive in asymptomatic infec tion6 and in patients
with a past history of visc e r al le ishmaniasis. Spec ific antigens from the L. donovani c omplex have been used in ELISA and in an immunoc hromatographic strip test for the identific ation of ac tive, subc linic al and asymptomatic VL in spec ific population groups2 2 4 3 3. Molec ular biology tec hniques, suc h as polymerase
c hain reac tion ( PCR) alone or in c ombination with hybridization have been used, espec ially in blood, to c onfirm the VL diagnosis in suspec t c ases, due to their sensitivity ( ranging from 7 5 to 9 8 % ) and spec ific ity ( ranging of 9 7 to 1 0 0 % ) in identifying the infec tion in individuals with low levels of parasites and antibodies in the absenc e of symptoms1 2 2 1 2 6 2 7.
Re gar ding VL e xpansio n and ur b anizatio n in B r azil, mo r e pr e c is e e s tim a te s o f a s ym pto m a tic L. c h a ga s i in fe c tio n o c c ur r e nc e in a give n po pulatio n ar e ne c e ssar y in o r de r to unde r stand the e xte nsio n o f the tr ansmissio n. The o b j e c tive o f this study was the ide ntific atio n o f asympto matic VL c ase s in a po pulatio n r e side nt in an ur b an ar e a, assaying diffe r e nt immuno lo gic al and mo lec ular b io lo gy diagno stic tec hniques.
PATIENTS AND METHODS
St u d y d e s i g n a n d p o p u l a t i o n . T h i s s tu d y wa s c o nduc te d to e valuate asympto matic L. c hagasi infec tio n in an ur b an ar e a o f Ge ne r al Car ne ir o distr ic t with a po pulatio n o f 1 9 , 5 0 0 in h a b ita n ts , s itua te d in Sa b a r á Co un ty, o f th e Me tr o po litan Re gio n o f B e lo Ho r izo nte , c apital o f the Minas Ge r ais State , B r azil. Fo r the last 1 5 ye ar s se r o lo gic al c anine s ur ve ys c o n duc te d r o utin e ly b y th e lo c a l Pub lic He a lth Se r vic e s have r e ve ale d pr e vale nc e r ate s r anging fr o m 5 to 1 0 % . Spo r adic human c ase s and de aths have b e e n r e po r te d. Fro m 1 9 8 9 to 2 0 0 4 , 1 3 c ases o f human VL have been repo rted
fr o m Ge ne r al Car ne ir o , with the o c c ur r e nc e o f o ne fatality. Additio n a lly, c uta n e o us le is h m a n ia s is c a us e d b y L. ( V. ) b r azilie nsis, has b e e n r e po r te d b y the he alth se r vic e s.
A c r o ss-se c tio nal study was c o nduc te d in 1 9 9 8 , using serologic al tests in blood samples c ollec ted in filter paper. The sample size ( n = 1 ,3 2 8 ) was c alc ulated based on the following par am e te r s: 1 ) an e stim ate d hum an infe c tio n pr e vale nc e rate of 3 .1 % , based on a study c onduc ted in the State of B ahia4;
2 ) pr e c is io n o f th e e s tim a te r a n gin g fr o m 2 . 2 % to 4 % ; 3 ) a error = 0 .0 5 and 4 ) population in the study area = 1 9 ,5 0 0 inhabitants. For operational reasons, households were used as sampling units. A simple random sample of c ity bloc ks was selec ted proportionally to the existent bloc ks, and within eac h selec ted bloc k, a random sample of households was drawn, proportionally to the number of existent houses. All inhabitants of the selec ted houses were eligible and were enrolled in the c ross- sec tional study. A total of 4 4 0 households were visited and 1 ,6 0 4 inhabitants were selec ted ( 8 .2 % of the population of General Carneiro) .
The mean age o f the 1 ,6 0 4 par tic ipants was 2 6 .8 ( ± 1 8 .6 ) years, the median age was 2 3 years ( 2 5 and 7 5 % inter-quartile r ange we r e 1 3 and 3 8 , r e spe c tive ly) ; 5 1 .7 % we r e fe male ; 6 9 .7 % had r e c e ive d o nly e le me ntar y sc ho o l e duc atio n and 9 .8 % had never go ne to sc ho o l. The mean per io d o f r esidenc e in this ar e a was 1 5 ( ± 1 1 .2 ) ye ar s.
After 1 2 mo nths, a sub set o f 1 2 8 par tic ipants, who pr o ved po sitive in se r o lo gic al te sts, was e nr o lle d to inve stigate the c o ur se o f the infe c tio n. A r ando m sub se t o f 1 2 8 ne gative par tic ipants was also inc lude d as a c o mpar iso n gr o up. The par tic ipants wer e c linic ally examined fo r signs and sympto ms o f VL in an o utpatie nts c linic o f the Ge ne r al Car ne ir o Pub lic He alth Se r vic e s, inte r vie we d, and a sam ple o f b lo o d was c o lle c te d a n d te s te d fo r in fe c tio n us in g s e r o lo gic a l a n d mo le c ular me tho ds.
The study was appr o ve d b y the Ethic al Re vie w B o ar d o f the Federal University o f Minas Gerais. All partic ipants o r their le gal guar dians, in the c ase o f mino r s, we r e r e quir e d to sign an Info r me d Co nse nt Fo r m b e fo r e data c o lle c tio n. Me dic al atte ndanc e and tr e atme nt, if ne c e ssar y, we r e guar ante e d fo r all par tic ipants.
Da ta c o lle c tio n. I n the c r o ss- se c tio nal study, b lo o d samples were c ollec ted by finger pric k onto filter paper ( Klabin nr 2 5 , B razil) dried and stored at 4 ºC until testing. Spots of 5 mm in diameter were eluted in pho sphate-buffered saline ( PB S) and examined by IFAT; same size spots were eluted in c asein-PB S for testing by ELISA using c rude antigen and strip test. In the sec ond evaluation c arried out after 1 2 months, blood was c ollec ted in a vac uum tube without antic oagulant; the sera were stored at -2 0 ºC and later tested by ELISA using both c rude and rk3 9 rec ombinant antigens and by IFAT. A sec ond vac uum tub e with EDTA was use d to c o lle c t b lo o d fo r pe r iphe r al mononuc lear c ells ( PB MC) , later used for DNA extrac tion.
Laboratory tests. Indirect immunofluorescent test: the IFAT was performed according to established methodology30; promastigotes
r o utine ly use d in the dia gno sis o f Le ishm ania, gr o wn to stationary phase in LIT ( Liver Infusion Tryptose) medium were u s e d . T h e s a m p l e s we r e c o n s i d e r e d p o s i ti ve wh e n fluo r e sc e nc e was o b se r ve d at 1 :4 0 dilutio n.
Enzyme-link ed immuno so r b ent assay: c r ude antige n was o b taine d fr o m the same L. amazo ne nsis str ain use d fo r IFAT, a c c o r din g to e s ta b lis h e d m e th o ds3 5; r k 3 9 r e c o m b in a n t
antige n ( spe c ific to the L. do no vani c o mple x) was use d, as pr e vio usly de sc r ib e d5. Antib o die s we r e de te c te d with go at
c o nj ugate d pe r o xidase -lab e le d anti-human IgG ( Sigma Co , US) . Re a c tio n s we r e r e a d a t 4 9 2 n m . Th e c ut- o ff va lue s established for eac h reac tion ( ELISA in filter paper and serum, and r k 3 9 -ELISA in se r um) we r e the me an ab so r b anc y value + 2 standar d de viatio ns fr o m 2 0 k no wn ne gative se r a at a 1 :8 0 dilutio n) .
Immunoc hromatographic strip test: this test used the rk3 9 antigen and was c onduc ted as previously desc ribed, using blood eluted from filter paper3 3. Three trained observers read the strips
independently; the test was only c onsidered to be positive when the results obtained by all three readers were in agreement.
An ti Tr yp a n o s o m a c r u zi a n ti b o di e s : du e to c r o s s -r e a c tivity in s e -r o lo gic a l te s ts , s e -r um s a m ple s we -r e a ls o assayed for T. c ruzi antibodies using indirec t hemagglutination ( Chagas Kit -FUNED-SES/MG, B r azil) and IFAT ( Chagas Kit – B io Manguinho s – FIOCRUZ, B r azil) .
DNA isolation: PB MC were isolated from 8 ml peripheral blood c ollec ted in EDTA-c oated tube after c entrifugation with Fic oll-Paque ( Pharmac ia, Uppsala, Sweden) . DNA was extrac ted by phenol/c hloroform/isoamyl alc ohol and ethanol prec ipitated, resuspended in 3 0 µl low TE buffer and stored at 4 ºC.
PCR amplific atio n: a pair o f pr imer s wer e used to amplify a fr agme nt o f 1 2 0 b p o f the c o nse r ve d r e gio n o f Le ishmania k DNA m in ic ir c le [ 5 ( G/C) ( G/C) ( C/G) CC( A/C) CTAT( A/T) TTACACCAACCCC - 3 ' and 5 ' -GGGGAGGGGCGTTCTGCGAA – 3 ' ]1 5 3 2. Fo r all r e ac tio ns 1 0 0 ng o f e ac h pr ime r, 2 mM dNTP
mixtur e , 1 .5 mM MgCl
2 , 2 .5 U Taq DNA po lyme r ase ( Amplitaq
go ld-Pe r k in Elme r ) we r e use d in a to tal r e ac tio n vo lume o f 2 5 ml, inc luding 1 ml o f sample o f DNA. The r e ac tio ns we r e c yc le d in a the r mal c yc le r ( PTC-1 0 0 , MJ Re se ar c h, Inc ) . The fo llo wing c o nditio ns we r e use d: an initial de natur atio n ste p at 9 5 ºC fo r 4 min, fo llo we d b y 3 0 c yc le s at 9 4 º fo r 3 0 se c , 5 0 º fo r 3 0 se c fo r anne aling, 7 2 º fo r 3 0 se c fo r e xte nsio n. In the final c yc le the e xte nsio n ste p was e xte nde d to 1 0 minute s. Po sitive and ne gative c o ntr o ls we r e use d in all r e ac tio ns pe r fo r me d. A 1 0 0 -b p DNA ladde r ( Gib c o B RL® ) was use d a s a m a r k e r. Sa m p le s we r e r e ga r de d a s p o s itive wh e n r e ve aling b ands o f 1 2 0 b p. Ne gative s sample s we r e te ste d fo r th e h um a n ß - glo b in ge n e to c o n fir m th a t DNA wa s n o t de gr ade d and that inhib itio n in PCR e xams had no t o c c ur r e d. Pr o c edur es to avo id c ar r yo ver c o ntaminatio n fr o m pr evio usly amplifie d DNA we r e use d r o utine ly1 9.
PCR produc t analyses and DNA hybridization: the reac tion p r o du c ts we r e vi s u a l i ze d i n 5 % p o l ya c r yl a m i de ge l elec trophoresis stained with silver2 9. The amplified DNA was
denatured and applied to nylon membranes ( Biodyne A, Gibc o
BRL ® ) using a bio-dot apparatus ( Hybri-dot manifold-BRL® ) . Probes c omposed of c loned minic irc les from L. c hagasi were radiolabeled with 3 2P - [ a] dCTP using the Rando m Pr ime r DNA
Labeling System ( Gibc o B RL)3 2. Hybridizatio n c o nditio ns were
as pr e vio usly de sc r ib e d1.
Positive and negative c ontrols: true negative and positive c ontrols; c onfirmed by c linic al, parasitologic al, serologic al and molec ular tests; were inc luded in all diagnostic tests performed. Re pr o duc ib ility: te n pe r c e nt o f b lo o d sample s c o lle c te d o n filte r pape r and DNA sample s we r e r ando mly se le c te d and m ar k e d fo r r e te sting; e ac h duplic ate r e c e ive d a diffe r e nt numb e r fr o m the o r iginal sample .
Nu tr i ti o n a l s ta tu s : m a l n u tr i ti o n wa s de te r m i n e d b y analyzing the c hildr e n’s we ight and he ight fo r age ac c o r ding to the po pulatio n patte r n o f the Re fe r e nc e Natio nal Ce nte r He alth Statistic s, using EPI-NUT/EPI-INFO ( ve r sio n 6 .0 4 d) . Par tic ipants o ve r te n ye ar s we r e e valuate d using the r atio o f we ight b y squar e he ight.
Statistic al analysis: the agreement between qualitative tests was e stimate d b y the k appa statistic2 8; q uantitative r e sults
we r e c o mpar e d b y Pe ar so n’s c o r r e latio n ( r ) , using lo g tite r + 1 ( IFAT) and ab so r b anc e s ( ELISA) .
RESULTS
Cr o ss- sectio nal study. The desc ription of the population studie d was r e alize d e lse whe r e2 2.
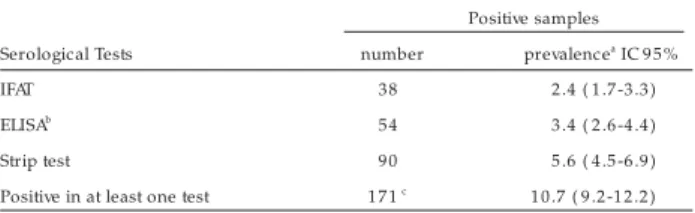
Tab le 1 sho ws the e stimate d pr e vale nc e r ate s b y e ac h se r o lo gic al te st pe r fo r me d in e luate s. Only e le ve n ( 6 .4 % ) sample s we r e simultane o usly po sitive in two te c hnique s. If we c o nsider as pro bably infec ted tho se samples whic h sho wed a po sitive r e sult in at le ast o ne te st pe r fo r me d, the e stimate d pr e vale nc e r ate was 1 0 .7 % ( 1 7 1 /1 6 0 4 ) .
Table 1 - Reactivity of the samples collected in filter paper in a serological survey ( n= 1 ,6 0 4 ) to identify the seroprevalence of infection by Leishmania in General Carneiro-Sabará/MG, 1 9 9 8 .
Positive samples
Serological Tests number prevalencea
IC 9 5 %
IFAT 38 2 .4 ( 1 .7 -3 .3 )
ELISAb 54 3 .4 ( 2 .6 -4 .4 )
Strip test 90 5 .6 ( 4 .5 -6 .9 )
Positive in at least one test 1 7 1 c
1 0 .7 ( 9 .2 -1 2 .2 )
aPrevalence = positive test/1 6 0 4 . bCrude antigen. c1 1 samples were positive in two tests
simultaneously: IFAT and ELISA= 8 ; Strip test and ELISA or IFAT= 3
The evaluatio n o f test repro duc ibility ( duplic ates) sho wed go o d agr e e me nt fo r IFAT ( k appa 0 .7 4 , 9 5 % CI 0 .4 0 -1 .0 ) , r e gular fo r ELISA ( k appa 0 .5 3 , 9 5 % CI 0 .1 8 -0 .8 9 ) and po o r agr eement fo r the str ip test ( kappa 0 .1 4 , 9 5 % CI -0 .1 1 -0 .4 0 ) . Pe ar so ns’ c o r r e latio n fo r ELISA ab so r b e nc y and IFAT tite r s fo r duplic ate s we r e r = 0 .6 3 and r = 0 .7 6 , r e spe c tive ly.
cross-sectional study: One hundred and eight positive participants included all the participants that were positive in ELISA or IFAT ( n= 8 4 ) and 5 0 % ( n= 4 4 ) of those positive in strip tests ( randomly chosen among those positive in this test; a decision based on the po o r r e pr o duc ib ility o f the te st) . A sub se t o f 1 2 8 ne gative participants was randomly selected among those negative in all tests performed.
Thirty partic ipants were lost during the follow up ( 2 6 among the positive group and 4 among the negative) due to refusals, death, reloc ation or insuffic ient biologic al material. The final sample evaluated c omprised 2 2 6 partic ipants: 1 0 2 positive and 1 2 4 negative. Comparison of the demographic c harac teristic s, suc h as age, gender and period of residenc e in General Carneiro, revealed no differences ( p > 0 .0 5 ) between the positive subjected inc luded and those not inc luded in this phase. The negative partic ipants showed a similar result ( p > 0 .0 5 ) among the negative population when the same variables were c ompared. The c harac teristic s of the 2 2 6 partic ipants are shown in Table 2 . This group c onstitutes a c ohort and the data showed refer to this first evaluation.
Table 3 shows the results of serologic al tests of the sera of the 2 2 6 partic ipants examined. Positive in sera inc lude both positive and negative in the cross-sectional study. It is worth noting that 1 3 0 ( 5 7 .5 %) were positive in at least one test and 4 9 ( 3 7 .7 %) were simultaneously positive in two or three tec hniques; 9 6 ( 4 2 .5 % ) were c onsidered negative in all the te sts pe r fo r me d.
Mo l e c u l a r t e s t r e s u l t s . Am o n g th e 2 2 6 s a m p l e s e xamine d, 1 3 3 we r e po sitive in hyb r idizatio n with a spe c ific pr o b e fo r the L. do no vani c o mple x.
Figur e 1 sho ws a r e pr e se ntative e le c tr o pho r e sis ge l o f PCR pr o duc ts and do t-b lo t hyb r idizatio n with spec ific pr o b es. The PCR and hyb r idizatio n ne gative sample s we r e analyze d b y PCR with spe c ific pr ime r s fo r the human ß -glo b in ge ne ; the tests c o nfirmed the presenc e o f human DNA in all samples. In additio n, the e valuatio n o f te st r e pr o duc ib ility, 2 3 b lind duplic ates, r evealed that PCR sho wed go o d agr eement ( kappa 0 .8 9 , 9 5 % CI 0 .6 7 -1 .0 ) .
Table 2 - Distribution of some demographical and social characteristics of the 2 2 6 participants from General Carneiro, Sabará/MG evaluated by serological and molecular techniques to diagnose asymptomatic visceral leishmaniasis
Variables Number Percentage
Gender
female 1 1 9 5 2 .7
male 1 0 7 4 7 .3
Race
white 55 2 4 .3
black 43 1 9 .0
mullato 1 2 8 5 6 .6
Age groups
> 1 0 years old 1 6 0 7 0 .8
1 – 1 0 years old 66 2 9 .2
Education1
college and high school 21 1 2 .0
elementary school 1 3 5 7 7 .1
no schooling 19 1 0 .9
Income ( minimum wage)
0 -3 1 0 2 4 5 .1
> 3 -1 5 1 2 4 5 4 .9
Natural of metropolitan region2
yes 1 4 6 6 8 .5
no 67 2 9 .6
Period of residence
1 -5 years 55 2 4 .3
> 5 years 1 7 1 7 5 .7
mean ± SD 1 6 .0 ± 1 1 .3
median ( IQR) 1 3 .5 ( 7 /2 4 )
IQR1 /Q3 = 2 5 % and 7 5 % inter quartil range
1only for more than 7 years old; n= 175. 2data for refusals, not known and not done are not shown
Table 3 -Reactivity of the 2 2 6 sera for Leishmania infection in follow-up phase, General Carneiro-Sabará/MG, 1 9 9 9 .
Positive samples
Serological Tests no proportiona ( %)
IFAT 74 3 2 .7
ELISA 60 2 6 .5
rk3 9 -ELISA 57 2 5 .2
positive in at least one test 1 3 0 b 5 7 .5
a
Proportion= positive test/2 2 6 . b 4 9 samples among of 1 3 0 samples were positive in
two or three tests simultaneously
Figur e 1 - Repr esentative po lyacr ylamide gel sho wing an amplificatio n pr o duct o f 1 2 0 bp fr o m kDNA minicir cles o f Leishmania in blo o d samples fr o m asympto matic individuals and do t blo t hybr idizatio n o f the same PCR pr o ducts per fo r med with L. do no vani co mplex specific kDNA pr o be. Lanes 3 ,4 ,6 ,8 show samples that wer e positive in the PCR and hybr idization assays; sample in lane 1 0 was po sitive fo r hybr idizatio n altho ugh the amplified pr oducts ar e not visible in the electr ophor esis gel. Lane 9 shows a weakly PCR po sitive sample but negative fo r hybr idizatio n. Lanes 1 and 1 6 : mo lecular size mar ker s ( 1 0 0 bp ladder ) . Po sitive co ntr o ls: lane 1 2 -amplificatio n pr o duct fr o m the blo o d o f a patient with kala- zar and lane 1 3 - DNA o f cultur ed L. chagasi. Negative co ntr o ls: lane 1 4 – no n- infected individual and lane 1 5 - no DNA in the PCR r eactio n mixtur e.
Co mpar iso n amo ng hybr idizatio n and ser o lo gical methods. The comparison of the results obtained in hybridization and serologic tests is shown in Table 4 . Among the 1 3 3 positive samples in hybridization, 7 4 ( 5 5 .6 %) were positive in at least one serological test and among the 9 3 negative in hybridization, 5 6 ( 6 0 .2 %) were positive in at least one serological test. Therefore, if the hybridization is c onsidered a referenc e diagnostic test for asymptomatic VL, the sensitivity estimate of serological techniques ranged from 24.8 to 30.1% and specificity ranged from 63.4 to 76.3%.
Cr o s s - r e a c t i o n wi t h Ch a g a s ’ d i s e a s e . E i g h t partic ipants were identified as sho wing po sitive tests ( Indirec t He m a gglutin a tio n a n d I FAT) in dic a tin g po s s ib le T. c r uzi infe c tio n; amo ng the se fo ur we r e also r e po r te d as having Chagas’ dise ase and six we r e po sitive in the hyb r idizatio n o r r k 3 9 -ELISA, sugge sting a T. c r uzi/L. c hagasi c o infec tio n.
Mo r e no EC e t a l
1 2 0 pb
Clinica l e x a mina tio n. Signs and sympto ms r elated to visc eral leishmaniasis were neither observed nor reported during c linic al examination. Only six partic ipants ( one c hild) showed low hematoc rit ( < 3 0 % ) , but with no signific ant differenc es in all o the r c linic al c r ite r ia use d to de fine infe c tio n; ( fe ve r, he pato me galy and/o r sple no me galy and we ight lo ss) .
Ma l n u t r i t i o n . E i gh t m a l n o u r i s h e d c h i l d r e n we r e ide ntifie d, tho ugh no ne o f the m pr e se nte d pr o gr e ssio n to c linic al dise ase . Two we r e po sitive in hyb r idizatio n and fo ur o f the m we r e po sitive o nly in se r o lo gic al te sts.
Cr iter ia for L. chagasi infection. Due to the disagreements found in the tests to identify asymptomatic infection using different diagnostic methods and the fac t that whic h subjec ts were in fac t infec ted remains undefined, different c riteria were proposed to define L. chagasi infection. Criterion 1 , greater specificity: include only partic ipants that were positive in the c rude antigen test and the spec ific antigen test and were c onfirmed by hybridization for L. c hagasi; 1 7 ( 7 .5 % ) partic ipants fulfilled this c riterion. Criterion 2 , parasite presenc e: inc lude all hybridization positive partic ipants; 1 3 3 ( 5 8 .8 % ) individuals were identified. Criterion 3 , positive serology and hybridization: inc lude all partic ipants with a positive hybridization and presenting, at least, one positive se r o lo gic al te st ( c r ude o r spe c ific antige n) ; 7 4 ( 3 2 . 7 % ) partic ipants were c onsidered as infec ted by L. c hagasi.
DISCUSSION
He r e i n , th e p r e s e n c e o f a s ym p to m a ti c i n fe c ti o n b y L. c hagasi in an ur b an ar e a o f So uthe ast B r azil was sho wn. The pr e vale nc e r ate s o f L. c hagasi infe c tio n e stimate d in a c r o ss-se c tio nal study, b y se r o lo gic al me tho ds, r ange d fr o m 2 .4 % ( IFAT) to 5 .6 % ( strip test) , depending o n the sero lo gic al te st use d. Whe n c o nside r ing tho se sample s that gave po sitive r e sults in at le ast o ne o f the te sts pe r fo r me d, the e stimate d pr e vale nc e r ate o f infe c tio n was 1 0 .7 % ( 1 7 1 /1 6 0 4 ) .
The lac k of c onc ordanc e among the serologic al tests was a limitation of the present investigation. The disc ordanc e among the serologic al tests c an not be explained by errors in c onduc ting the tests, bec ause the evaluation of test reproduc ibility revealed a go o d agreement fo r IFAT, and regular fo r ELISA; o nly the strip test revealed poor c o nc o r danc e in the duplic ate s. The
c o r r e la tio n s o f a b s o r b a n c e s ( ELI SA) o r tite r s ( I FAT) in duplic ate s also we r e go o d. The r e fo r e , it c an b e c o nc lude d that se r o lo gic al me tho ds ar e no t appr o pr iate fo r diagno sing asympto matic infe c tio n in ar e as o f lo w dise ase pr e vale nc e and o c c ur r e nc e o f c utane o us le ishmaniasis.
The DNA hybridization tec hnique identified a greater number of positive partic ipants when c ompared to the serologic al tests performed. Assuming DNA hybridization as the referenc e test for identifying individuals with ac tive L. c hagasi infec tion, the pa r tic ipa n ts wh o s h o we d po s itive s e r o lo gy a n d n e ga tive hybridization results c an be c onsidered as false-positives or self-c ured o f their infeself-c tio n. The po sitive sero lo gy in self-self-c ured subjec ts c ould be a c onsequenc e of a gradual and slow dec rease in titers, as demonstrated in other infec tions8 The serologic al
tests were able to identify the presenc e of infec tion in 3 0 .1 , 2 4 .8 and 2 6 .3 % of those with positive hybridization ( IFAT, ELISA and rk3 9 -ELISA, respec tively. Therefore, when the hybridization is c onsidered the referenc e test, serology ( positive for at least one serologic al test) was able to identify 5 5 .6 % ( 7 4 /1 3 3 ) of the individuals who were truly infec ted. Furthermore, serology was able to identify 3 9 .8 % ( 3 7 /9 3 ) of the individuals who were truly negative; spec ific ity of 6 3 .4 , 7 1 .0 and 7 6 .3 % , for IFAT, ELISA and rk3 9 -ELISA, respec tively.
The greatest c hallenge of this investigation was to understand the disagreement among the diagnostic methods used to identify asymptomatic L. c hagasi infec tion. The different antigens used to perform the tests may explain, in part, the low c onc ordanc e and c o r r elatio n amo ng ser o lo gic al tests. The antige n r k 3 9 pr esents high sensitivity and spec ific ity fo r the L. do no vani c omplex and has been assoc iated with ac tive disease2. In the
pr e se nt study, amo ng tho se po sitive in hyb r idizatio n, r k 3 9 showed high spec ific ity ( 7 1 /9 3 = 7 6 .3 % ) , but low sensitivity for asymptomatic individuals ( 3 5 /1 3 3 = 2 6 .3 %) . It is also known that ELISA with c rude antigen and IFAT present some limitations, suc h as c ross-reac ting with other parasitic infec tions ( eg T. c ruzi and o the r le ishmaniasis) o r the de te c tio n o f past infe c tio n2 2 6.
Therefore, the use of only one serologic test may not reflec t the true prevalenc e of an infec tion in a population at risk, leading to misc lassific ation bias in epidemiologic al studies.
The different algorithms proposed to identify infection present spec ific advantages and limitations. Criterion 1 is more rigorous in defining the infec tion; however, some true positives c ould have been exc luded bec ause the definition requires positive results in mo lec ular and ser o lo gic al tests with c r ude and spec ific antige ns. Se r a fr o m infe c te d patie nts may sho w distinc tive rec ognition of c rude and spec ific antigens and patients with asympto matic o r self-healing infec tio ns may present lo w o r undetec table levels of anti-k3 9 antibodies2. Criterion 2 suggests
the presenc e of c irc ulating parasites in the blood, inc luding individuals that were positive in hybridization, independent of the se r o lo gic al r e sults. In c r ite r io n 3 so me po sitive s we r e probably exc luded bec ause the algorithm is dependent on a serologic al test and, as mentioned elsewhere, asymptomatic individuals present low levels of antibodies and minute amounts o f c ir c ulating pa r a s ite s wh e n c o m pa r e d to s ym pto m a tic patie nts2 2 6. Thus, the pe r fo r manc e o f the se r o lo gic al te sts
Table 4 -Estimates of sensitivity and specificity of the diagnostic tests in identifying L. chagasi infection using the DNA hybridization as the reference test. General Carneiro -Sabará/MG, 1 9 9 9 .
Positive in Sensitivity Negative in Specificity
serology and ( IC 9 5 %)1
serology and ( IC 9 5 %)2
Serology hybridization hybridization
IFAT 40 3 0 .1 ( 2 2 .4 -3 8 .6 ) 59 6 3 .4 ( 5 2 .8 -7 3 .2 )
ELISA 33 2 4 .8 ( 1 7 .7 -3 3 .0 ) 66 7 1 .0 ( 6 0 .6 -7 9 .9 )
rk3 9 -ELISA 35 2 6 .3 ( 1 9 .1 -3 4 .7 ) 71 7 6 .3 ( 6 6 .4 -8 4 .5 )
Serological tests 74 5 5 .6 ( 4 6 .8 - 6 4 .3 )3
374
3 9 .8 ( 2 9 .8 -5 0 .5 )
1
positives in eac h serologic al test and hybridization /1 3 3 positive partic ipants in hybridization. 2 negatives in each serological test and hybridization /93 negative participants
in hybridization. 3
positives in at least one serological test and hybridization/1 3 3 positive participants in hybridization. 4 negatives in all serological tests and in hybridization/9 3
sho uld b e inte r pr e te d diffe r e ntly in e pide mio lo gic al studie s de vise d to ide ntify asympto matic infe c tio n in a po pulatio n and in studie s c o nduc te d to diagno se c linic al c ase s o r to c o nfir m suspe c te d c ase s. Mo r e o ve r, ne gative hyb r idizatio n may b e due to the amo unt o f b lo o d use d, whic h c o uld have b e e n insuffic ie nt to pe r mit the e xtr ac tio n o f par asite DNA2 3 .
The lac k of a gold standard tec hnique to c onfirm an ac tive L. c hagasi infec tion in asymptomatic individuals is an important drawbac k in population studies. The use of invasive proc edures to de te c t the par asite ( sple e n, b o ne mar r o w, lymph no de aspirates) it is not justified for ethic al reasons when the patient does not show any symptoms of the disease, whic h was the c ase in the present study. Blood c ulture is not the method of c hoic e to prove the presenc e of the parasite due to the low sensitivity when assayed in asymptomatic c arriers2 7. Although the molec ular
m e tho ds ar e no t e asily availab le fo r r o utine te sting, DNA hyb r idizatio n sho uld b e pr e fe r r e d in the ide ntific atio n o f asymptomatic infec tion. The hybridization is more spec ific than serologic al tests in identifying ac tive infec tion and c an be used to disc riminate false positives and false negatives. However, although it is high sensitivity, hybridization c an not identify 1 0 0 % of the true positive, sinc e parasite presenc e may be intermittent in peripheral blood2 0.
Othe r impo r tant finding o f this study is the ab se nc e o f c l i n i c a l di s e a s e . Th e o c c u r r e n c e o f a s ym p to m a ti c a n d s ub c lin ic a l illn e s s with n o n s pe c ific s ym pto m s h a s b e e n r e po r te d in inve stigatio ns c o nduc te d in No r the aste r n B r azil. Ho we ve r, in the se ar e as c linic al c ase s have b e e n fo und and the r atio o f infe c te d/dise ase d pe r so ns r ange d fr o m 6 .5 :1 to 2 8 :13 6 1 6. In the ar e a studie d, a po ssib le e xplanatio n fo r the
ab se nc e o f the dise ase wo uld b e the lo w le ve l o f malnutr itio n in the po pulatio n studie d, an impo r tant pr o gno stic fac to r fo r dis e a s e pr o gr e s s io n4 9. I n th is in ve s tiga tio n , o n ly e igh t
malno ur ishe d c hildr e n we r e ide ntifie d and no ne de ve lo pe d c linic al signs o r sympto ms o f VL. Similar results were o btained in c o ho r t studie s c ar r ie d o ut with c hildr e n in no r the aste r n B r azil, whe r e asympto matic and sub c linic al c ase s also did no t pro gress to the ac ute fo rm o f VL6 1 7 1 8
. If L. c hagasi infec tion do e s no t pr o gr e ss to visc e r al le ishmaniasis within the fir st o r sec o nd year after infec tio n, it is unlik ely to do so in o ther wise he althy individuals1 8. It is b e c o ming c le ar that asympto matic
infe c tio ns sho uld b e c o nside r e d an impo r tant aspe c t o f VL e pide mio lo gy. Pub lishe d r e sults sugge st that phle b o to mine sand flie s do no t ac quir e the infe c tio n fr o m asympto matic i n d i vi d u a l s1 0. Ne ve r th e l e s s , q u e s ti o n s r e g a r d i n g th e
c o mpe te nc e o f asympto matic individuals to infe c t the ve c to r, e spe c ially whe n fo und in high numb e r s, r e main unso lve d1 1.
The present VL c ontrol strategies in Brazil are based on the oc c urrenc e of symptomatic c ases; it is important from a public health perspec tive, to understand the role of asymptomatic c ases in maintaining the infec tion in urban areas and to identify risk fac to r s le ading to dise ase pr o gr e ssio n. Unfo r tunate ly, the disagr e e m e nts in the te st r e sults o b se r ve d in the pr e se nt investigation suggest that the available diagnostic tests are not adequate for identifying asymptomatic infec tion. Based on the present data, the PCR produc ts submitted to hybridization with
spec ific probes seem to disc riminate the real infec tions and will improve confidence in diagnosing asymptomatic subjects in areas of low prevalenc e of c linic al disease.
ACKNOWLEDGMENTS
To Sec r etar ia Munic ipal de Saúde de Sabar á, Minas Ger ais and Fundaç ão Nac io nal de Saúde , Minas Ge r ais, fo r the ir c o o pe r a tio n a n d lo gis tic a l s uppo r t. To Dr. Ste ve n R e e d ( Infe c tio us Dise ase Re se ar c h Institute , Se atle ) fo r pr o viding the r k 3 9 antige n and the str ip te st and Dr. Oc távio Fe r nande s ( Fundaç ão Oswaldo Cr uz, Rio de Jane ir o ) fo r pr o viding the pr o b e s fo r hyb r idizatio n. To Dr. Vandak No b r e Jr ( Fac uldade de Me dic ina, Unive r sidade Fe de r al de Minas Ge r ais) fo r c o llab o r atio n in c linic al e xams and Ro sange la Fátima Go me s a n d R o b e r to Te o do r o da Co s ta fo r la b o r a to r y te c h n ic a l suppo r t.
REFERENCES
1 . An dr a de ASR , Go m e s R F, Fe r n a n de s O, Me lo MN. Us e o f DNA- b a s e d
diagno stic me tho ds fo r human le ishmaniasis in Minas Ge r ais, B r azil. Ac ta
Tr o pic a 7 8 : 2 6 1 -2 6 7 , 2 0 0 1 .
2 . B adar ó R, B e nso n D, Eulálio MC, Fr e ir e M, Cunha S, Ne to EM, Pe dr
al-Sampaio D, Madur e ir a C, B ur ns JM, Ho ughto n RL, David JR, Re e d SG. r k 3 9 :
A c lo n e d a n tige n o f Le is h m a n ia c h a ga s i th a t pr e dic ts a c tive vis c e r a l
le ishmaniais. J o ur nal o f Infe c tio us Dise ase s 1 7 3 : 7 5 8 - 7 6 1 , 1 9 9 6 .
3 . B adar ó R, Jo ne s TC, Car valho EM, Sampaio D, Re e d SG, B ar r al A, Te ixe ir a
R, J o hnso n WD J r. Ne w pe r spe c tive s o n a sub c linic al fo r m o f visc e r al
le ishmaniasis. Jo ur nal o f Infe c tio us Dise ase s 1 5 4 : 1 0 0 3 -1 0 1 1 , 1 9 8 6 a.
4 . B adar ó R, Jo ne s TC, Lo r e nç o R, Ce r f J, Sampaio D, Car valho EM, Ro c ha H,
Te ixe ir a R, Jo hnso n Jr WD. A pr o spe c tive study o f visc e r al le ishmaniasis in
an e nde mic ar e a o f B r asil. Jo ur nal o f Infe c tio us Dise ase s 1 5 4 : 6 3 9 -6 4 9 ,
1 9 8 6 b .
5 . B ur ns J M, Shr e ffle r WG, B e nso n DR, Gha lib HW, B a da r ó R, Re e d SG.
Mo le c ular c har ac te r izatio n o f a k ine sin- r e late d antige n o f Le ishm ania
c hagasi that de te c ts spe c ific antib o dy in Afr ic an and Ame r ic an visc e r al
le ishmaniasis. Pr o c e e dings o f the Natio nal Ac ade my o f Sc ie nc e s o f the
Unite d State s o f Ame r ic a 9 0 : 7 7 5 - 7 7 9 , 1 9 9 3 .
6 . Caldas AJ M, Silva, DRC, Pe r e ir a CCR, Nune s, PMS, Silva B P, Silva AAM,
B ar r al A, Co sta JML. Infe c ç ão po r Le ishmania ( Le ishmania) c hagasi e m
c r ianç as de uma ár e a e ndê mic a de le ishmanio se visc e r al ame r ic ana na
Ilha de São Luis-MA, B r asil. Re vista da So c ie dade B r asile ir a de Me dic ina
Tr o pic al 3 4 : 4 4 5 -4 5 1 , 2 0 0 1 .
7 . Ca m a r go ME, R e b o n a to C. Cr o s s - r e a c tivity in fluo r e s c e n c e te s ts fo r
Tr ypano so ma and Le ishmania antib o die s. A single inhib itio n pr o c e dur e to
e nsur e spe c ific r e sults. The Ame r ic an Jo ur nal o f Tr o pic al Me dic ine and
Hygie ne 1 8 : 5 0 0 -5 0 5 , 1 9 6 9 .
8 . Ca n ç a do J R. Lo n g te r m e va lua tio n o f e tio lo gic a l tr e a tm e n t o f Ch a ga s
dise ase with B e nzanidazo le . Re vista do Instituto de Me dic ina Tr o pic al de
São Paulo 1 : 2 9 -3 7 , 2 0 0 2 .
9 . Ce r f B J , J o ne s TC, B adar ó R, Sam paio D, Te ixe ir a R, J o hnso n J r WD.
Malnutr itio n as a r isk fac to r fo r se ve r e visc e r al le ishmaniasis. J o ur nal o f
Infe c tio us Dise ase s 1 5 6 : 1 0 3 0 -1 0 3 3 , 1 9 8 7 .
1 0 . Co sta CH, Go me s RB , Silva MR, Gar c e z LM, Ramo s PK, Santo s RS, Shaw J J ,
David J r, Maguir e J H. Co mpe te nc e o f the human ho st as a r e se r vo ir fo r
Le ishmania c hagasi. Jo ur nal o f Infe c tio us Dise ase s 1 8 2 : 9 9 7 -1 0 0 0 , 2 0 0 0 .
1 1 . Co sta CH, Stewar t JM, Go mes RB B , Gar c ez LM, Ramo s PK, B o zza M, Sato skar
Asympto matic human c ar r ier s o f Leishmania c hagasi. The Americ an Jo urnal o f Tr o pic al Me dic ine and Hygie ne 6 6 : 3 3 4 - 3 3 7 , 2 0 0 2 .
1 2 . Co sta J M, Dur nad R, De niau M, Rivo lle t D, Izr i M, Ho uin R, Vidaud M,
B r e tagne S. PCR Enzyme - link e d immuno so r b e nt assay fo r Diagno sis o f Le ishmaniasis in human Immuno de fic ie nc y Vir us-infe c te d Patie nts. Jo ur nal o f Clinic al Mic r o b io lo gy 3 4 : 1 8 3 1 - 1 8 3 3 , 1 9 9 6 .
1 3 . Cunha S, Fr e ir e , M, Eulálio C, Cr istó vão J , Ne tto E, J o hnso n J r WD, Re e d SG, B adar ó R. Visc e r al le ishmaniasis in a ne w e c o lo gic al nic he ne ar a maj o r me tr o po litan ar e a o f B r azil. Tr ansac tio ns o f the Ro yal So c ie ty o f Tr o pic al Me dic ine and Hygie ne 8 9 : 1 5 5 - 1 5 8 , 1 9 9 5 .
1 4 . D’Olive ir a J r A, Co s ta , SRM, B a r b o s a AB , Or ge MLGO, Ca r va lh o EM. Asym pto m atic Le ishm ania c hagasi infe c tio n in r e lative s and ne ighb o r s o f patie nts with visc e r al le ishmaniasis. Me mó r ias do Instituto Oswaldo Cr uz 9 2 : 1 5 -2 0 , 1 9 9 7 .
1 5 . De gr ave W, Fe r nande s O, Campb e ll D, B o zza M, Lo pe s UG. Use o f mo le c ular pr o b e s and PCR fo r de te c tio n and typing o f Le ishmania- a mini- r e vie w. Me mó r ias do Instituto Oswaldo Cr uz 8 9 : 4 6 3 - 4 6 9 , 1 9 9 4 .
1 6 . Evans TG, Te ixe ir a MJ, Mc Auliffe IT, Vasc o nc e lo s I, Vasc o nc e lo s AW, So usa
AA, Lim a J W, Pe a r s o n RD. Epide m io lo gy o f Vis c e r a l Le is h m a n ia s is in No r the ast B r azil. Jo ur nal o f Infe c tio us Dise ase s 1 6 6 : 1 1 2 4 -1 1 3 2 , 1 9 9 2 .
1 7 . Gama MEA, Co sta J ML, Go me s CMC, Co r b e tt CEP. Sub c linic al fo r m o f the Am e r ic an Visc e r al Le ishm aniasis. Me m ó r ias do Instituto Oswaldo Cr uz 9 9 : 8 8 9 -8 9 3 , 2 0 0 4 .
1 8 . Je r o nimo SMB , Te ixe ir a MJ, So usa AQ, Thie lk ing P, Pe ar so n RD Evans TG. Na tu r a l h i s to r y o f Le i s h m a n i a ( Le i s h m a n i a ) c h a ga s i i n fe c ti o n i n No r th e a s te r n B r a zil: Lo n g- te r m fo llo w- up. Clin ic a l I n fe c tio us Dis e a s e 3 0 : 6 0 8 -6 0 9 , 2 0 0 0 .
1 9 . Kwo k S, Higuc hi R. Avo iding false po sitive s with PCR. Natur e 3 3 9 : 2 3 7 -2 3 8 , 1 9 8 9 .
2 0 . Le Fic ho ux Y, Quar anta JF, Aufeuvr e JP, Lelievr e A, Mar ty P, Suffia I, Ro usseau D , Ku b a r J . O c c u r r e n c e o f Le i s h m a n i a i n fa n tu m p a r a s i te m i a i n asympto matic b lo o d do no r s living in an ar e a o f e nde mic ity in so uthe r n Fr anc e . Jo ur nal o f Cinic al Mic r o b io lo gy 3 7 : 1 9 5 3 -1 9 5 7 , 1 9 9 9 .
2 1 . Mar tin-Sanc he z J, Pine da JA, Mo r illas-Mar q ue z F, Gar c ia-Gar c ia JA, Ac e do C, Mac ias J. Detec tio n o f Leishmania infantum kineto plast DNA in peripheral b lo o d fr o m asympto matic individuals at r isk fo r par e nte r ally tr ansmitte d infe c tio ns: r e latio nship b e twe e n po lyme r ase c hain r e ac tio n r e sults and o ther Leishmania infec tio n markers. Americ an Jo urnal o f Tro pic al Medic ine and Hygie ne 7 0 : 5 4 5 -5 4 8 , 2 0 0 4 .
2 2 . Mo r e no EC, Me lo MN, Ge nar o O, Lamb e r tuc c i J R, Se r ufo J C, Andr ade ASR, Antune s CMF, Car ne ir o M. Risk fac to r s fo r Le ishmania c hagasi infe c tio n in an ur b an ár e a o f Minas Ge r ais State . Re vista da So c ie dade B r asile ir a de Me dic ina Tr o pic al 3 8 : 4 5 6 -4 6 3 , 2 0 0 5
2 3 . Nuzum E, White Iii F, Thakur R, Dietze R, Wages J, Grogl M, Berman J. Diagnosis of Symptomatic Visc eral Leishmaniasis by Use of the Polymerase Chain Reac tion on Patient B lood. Journal of Infec tious Diseases 1 7 1 :7 5 1 -7 5 4 , 1 9 9 5 .
2 4 . Ote r o ACS, Silva VO, Luz KG, Palatnik M, Pir me z C, Fe r nande s O, Palatinik -de -So uza CB . Sho r t r e po r t: o c c ur r e nc e o f Le ishmania do no vani DNA in do nate d b lo o d fr o m se r o r e ac tive B r azilian b lo o d do no r s. The Ame r ic an
Jo ur nal o f Tr o pic al Me dic ine and Hygie ne 6 2 : 1 2 8 -1 3 1 , 2 0 0 0 .
2 5 . Pampiglio ne S, Manso n- B ahr PEC, Giuingi F, Giunti G, Par e nti A, Cane str i Tr o tti G. Studie s o n Me dite r r ane an le ishmaniasis 2 Asympto matic c ase s o f Vis c e r a l le is h m a n ia s is . Tr a n s a c tio n s o f th e Ro ya l So c ie ty o f Tr o pic a l Me dic ine and Hygie ne 6 8 : 4 4 7 - 4 5 3 , 1 9 7 4 .
2 6 . Piar r o ux R, Gamb ar e lli F, Dumo n H, Fo nte s M, Dunan S, Mar y C, To ga B , Qu i l i c i M. Co m p a r i s o n o f P CR wi th d i r e c t e x a m i n a ti o n s o f b o n e mar r o w aspir atio n, mye lo c ultur e , and se r o lo gy fo r diagno sis o f visc e r al l e i s h m a n i a s i s i n i m m u n o c o m p r o m i s e d p a ti e n s . J o u r n a l o f Cl i n i c a l Mic r o b io lo gy 3 2 : 7 4 6 - 7 4 9 , 1 9 9 4 .
2 7 . Riera C, Fisa R, Udina M, Gállego M, Portus M. Detec tion of Leishmania infantum c ryptic infec tion in asymptomatic blood donors living in an endemic area ( Eivissa, B alearic Islands, Spain) by different diagnostic methods. Transac tions of the Royal Soc iety of Tropic al Medic ine and Hygiene 9 8 :1 0 2 -1 1 0 ,2 0 0 4 .
2 8 . Sac k e tt DL, Hayne s RB , Guyatt GH, Tugwe ll P. Clinic al Epide mio lo gy: a b asic sc ie nc e fo r c linic al me dic ine . Little , B r o wn and Co mpany, B o sto n, 1 9 9 1 .
2 9 . Santo s FR, Pe na SDJ, Epple n JT. Ge ne tic and po pulatio n study o f a Y-link e d te tr a nuc le o tide r e pe a t DNA po lym o r phism with a sim ple no n- iso to pic te c hniq ue . Human Ge ne tic s 9 0 : 6 5 5 - 6 5 6 , 1 9 9 3 .
3 0 . Shaw J J , Vo lle r A. The de te c tio n o f c ir c ulating antib o dy to k ala- azar b y m e a n s o f im m un o fluo r e s c e n t te c h n iq ue s . Tr a n s a c tio n s o f th e R o ya l So c ie ty o f Tr o pic al Me dic ine and Hygie ne 5 8 : 3 4 9 - 3 5 2 , 1 9 6 4 .
3 1 . S i l va E S , Go n ti j o CMF, P a c h e c o R S , Fi u za VOP, B r a zi l R . Vi s c e r a l Le ishm a nia sis in the Me tr o po lita n Re gio n o f B e lo Ho r izo nte , Sta te o f Minas Gerais, B razil. Memórias do Instituto Oswaldo Cruz 9 6 :2 8 5 -2 9 1 , 2 0 0 1 .
3 2 . Silva ES, Go ntij o CMF, Pir me z C, Fe r nande s O, B r azil RP. Sho r t r e po r t: de te c tio n o f Le ishm a nia DNA b y po lym e r a se c ha in r e a c tio n o n b lo o d sample s fr o m do gs with visc e r al le ishmaniasis. The Ame r ic an J o ur nal o f Tr o pic al Me dic ine and Hygie ne 6 5 : 8 9 6 - 8 9 8 , 2 0 0 1 .
3 3 . Sundar S, Re e d S, Singh VP, Kumar PCK, Mur r ay HW. Rapid ac c ur ate fie ld diagno sis o f Indian visc e r al le ishmaniasis. The Lanc e t 3 5 1 :5 6 3 -5 6 5 , 1 9 9 8 .
3 4 . Vi e i r a J B F, Co e l h o GE. Le i s h m a n i o s e Vi s c e r a l o u Ca l a za r : As p e c to s epidemio ló gic o s e de c o ntr o le. Revista da So c iedade B r asileir a de Medic ina Tr o pic al 3 1 : 8 5 -9 2 , 1 9 9 8 .