The secretory immunoglobulin A response to
Mycobacterium
tuberculosis
in a childhood population
Resposta da imunoglobulina A secretória ao Mycobacterium tuberculosis
em população infantil
Carlos Fernández de Larrea
1, Jacobus Henry de Waard
2,
Francesca Giampietro
3and Zaida Araujo
3ABSTRACT
We report on the measurement of saliva anti-Purified Protein Derivative sIgA and 3 8 kDa antibodies from 1 2 7 c hildren, of whom 3 1 were strong tuberc ulosis suspec ts and 9 6 were healthy c ontac t c hildren. The results c onc erning the perc entage of c hildren with antib o dy reac tivity to PPD and 3 8 kDa antigens showed that, of these 2 antigens, 3 8 kDa induc ed higher reac tivity in patients positive and negative for the Tuberc ulin Skin Test ( 2 8 % and 1 6 .6 % , respec tively) in c omparison to c ontrols positive and negative for the TST ( 1 1 .7 % and 7 .1 % , respec tively) . There was a statistic ally signific ant differenc e between patients positive and c ontrols negative for the TST. In relation to the Purified Protein Derivative antigen, while 1 4 .2 % of patients positive for the TST showed antibody reac tivity to the PPD antigen, no patients negative for the TST had reac tivity to this antigen. The findings suggest that these two antigens seem be assoc iated with a different development of the muc osal defenc e mec hanisms mediated by sIgA against Myc obac terium tuberc ulosis.
Ke y- wo r ds: Tub e r c ulo sis. War ao . Se c r e to r y IgA. Tub e r c ulin sk in te st.
RESUMO
Fo r am do sado s antic o r po s sIgA anti-Purified Protein Derivative e 3 8 k Da da saliva de 1 2 7 c r ianç as, das quais 3 1 e r am de pac ientes altamente suspeito s de tuber c ulo se e 9 6 er am pr o venientes de c r ianç as saudáveis, que tiver am c o ntato c o m pac ientes. Os resultado s referentes à po rc entagem de c rianç as, reativas ao PPD e ao antígeno 3 8 kDa, mo straram que destes do is antígeno s, o 3 8 kDa induziu maio r r eatividade em pac ientes po sitivo s e negativo s ao Tub er c ulin Skin Test ( 2 8 % e 1 6 ,6 % , r espec tivamente) , e m c o mpar aç ão ao s c o ntr o le s po sitivo s e ne gativo s ao TST ( 1 1 ,7 % e 7 ,1 % , r e spe c tivame nte ) . Ho uve dife r e nç a e statistic ame nte signific ativa e ntr e pac ie nte s po sitivo s e c o ntr o le s ne gativo s ao Tub e r c ulin Sk in Te st. Em r e laç ão ao antíge no PPD, e nquanto 1 4 ,2 % de pac ie nte s po sitivo s ao TST mo str ar am antic o r po s r e ativo s ao antíge no Pur ifie d Pr o te in De r ivative , ne nhum pac ie nte ne gativo ao TST fo i r e ativo ao antíge no . Os ac hado s suge r e m que , apar e nte me nte , e ste s do is antíge no s e stão asso c iado s a de se nvo lvime nto distinto do s me c anismo s de de fe sa da muc o sa me diado s po r sIgA c o ntr a Myc o b ac te r ium tub e r c ulo sis.
Pa la vr a s- cha ve s: Tub e r c ulo se . War ao . IgA se c r e tó r ia. Te ste c utâne o da tub e r c ulina.
1 . Ho spital Var gas de Car ac as, Unive r sidad Ce ntr al de Ve ne zue la, Car ac as, Ve ne zue la. 2 . Lab o r ato r io de Tub e r c ulo sis, Instituto de B io me dic ina, Unive r sidad Ce ntr al de Ve ne zue la, Car ac as, Ve ne zue la. 3 . Lab o r ato r io de Inmuno lo gía de Enfe r me dade s Infe c c io sas, Instituto de B io me dic ina, Unive r sidad Ce ntr al de Ve ne zue la, Car ac as, Ve ne zue la.
The study was suppo r te d b y e l Fo ndo Nac io nal de Cie nc ia, Te c no lo gía e Inno vac ió n ( FONACIT) , S1 -2 0 0 0 0 0 0 6 6 7 .
Addr e ss to : Dr a. Zaida Ar auj o . Lab o r ato r io de Inmuno lo gía de Enfe r me dade s Infe c c io sas. Instituto de B io me dic ina. Apar tado 4 0 4 3 , Car ac as 1 0 1 0 A, Ve ne zue la. Te le fax: 5 8 2 1 2 5 6 4 -2 9 7 8 /4 1 4 2 4 8 -0 2 1 5 .
e -mail: zar auj o @ te lc e l. ne t. ve /zar auj o gar c ia@ yaho o . c o m Re c e b ido par a pub lic aç ão e m 2 2 /1 2 /2 0 0 5
Ac e ito e m 8 /9 /2 0 0 6
Myc o b ac te r ia, inc luding tho se that c ause tub e r c ulo sis
( T B ) , c r o s s m u c o s a l b a r r i e r s a n d e n te r m u c o s a l
lym pho e pithe lial site s, whic h inc lude o r o phar ynge al and
naso phar ynge al to nsils2 2. De ndr itic c e lls and mac r o phage s
in the se site s allo w fo r myc o b ac te r ial r e plic atio n, b e c ause o f
the permissive immuno lo gic al enviro ment in lympho epithelial
tissue s, whe r e b a c te r ia a ppe a r to a da pt the ir im m e dia te
e nvir o nme nt to favo r sur vival and may c ar r y o ut e sse ntial
immunoregulatory mec hanisms designed to minimize immune
patho lo gy o r the inappro priate ac tivatio n o f immune effec to rs.
Thus Myc o b ac te r ium tub e r c ulo sis c an e stab lish life - lo ng
c hronic infec tions in their hosts after an ac ute infec tion period
invo lving the a c tiva tio n o f b o th the inna te a nd a c q uir e d
Muc o sal sur fac e s r e pr e se nt a ve r y lar ge ar e a, and in the
ab se nc e o f spe c ific immune de fe nse me c hanisms we wo uld r apidly b e o ve r whe lme d b y b ac te r ial patho ge ns. Eve n in the
pr esenc e o f effec tive muc o sal immune mec hanisms, b ac ter ial
infe c tio ns o f the gastr o inte stinal, r e spir ato r y and ur o ge nital
muc o sae ar e suffic iently c o mmo n to r epr esent a maj o r glo b al
h e a lth p r o b le m4 1 2 1 7. Th us , e n te r ic , c h r o n ic a n d a c ute
r e spir ato r y tr ac t infe c tio ns ar e the thr e e le ading c ause s o f
illn e s s a n d de a th glo b a lly. Th e y a ffe c t m a in ly c h ildh o o d
populations in developing c ountries, suc h as Venezuela, where a c hr o nic r e spir ato r y infe c tio n lik e TB in so me indige no us
c o mmunitie s to wns, suc h as Mur ak o and Ko amuho , r e ac h a
pr e vale nc e o f ne ar ly 2 % within a c hildho o d po pulatio n2 0.
Ab o ut 6 0 % o f the to ta l im m uno glo b ulin pr o duc e d in
humans is IgA. Although IgA makes up only 1 0 -1 5 % of serum immuno glo b ulin, it is the pr edo minant immuno glo b ulin in
muc osal sec retions. There are two subc lasses of IgA in humans:
IgA1 and IgA2 , serum c ontains 8 0 -9 0 % IgA1 whereas muc osal
sec retions c ontain up to 6 0 % IgA2 . The assoc iation of IgA dimers with a sec retory c omponent molec ule fac ilitates transport of this
isotype into the lumen, where they c an interac t with antigens.
The oligomeric nature of IgA enhanc es its ability to interac t with
high avidity with vir use s and b ac te r ia that ar e pr e se nt in
sec retions1 2 3 7. IgA antibodies also bind well to Fc rec eptors on
neutrophils. In this regard, sinc e the identific ation of rec eptors
fo r I gA o n the s ur fa c e o f b lo o d le uk o c yte s a nd a lve o la r
mac rophages was reported, the role of sec retory IgA ( sIgA) in the defenc e of muc osal surfac es at the level of the respiratory
trac t has now expanded from the limited role of exogenous
mater ial sc avenger to a b r o ader pr o tec tive func tio n with a
potential protec tive role2 6. It has been reported that IgG is the
predominant immunoglobulin in the lower respiratory trac t,
followed by sIgA1 6. Most IgA defic ient individuals experienc e
r e s pir a to r y in fe c tio n s , m a la b s o r ptio n a n d a uto im m un e
disorders9 1 4.
Sec retory IgA was found to be signific antly higher in smear negative and c ulture positive c ases of TB c ompared with c ulture
negative c ases3 3. In addition, intranasal inoc ulation of mic e with
IgA against M. tuberc ulosis antigen diminished the tuberc ulosis
infec tion in the lungs2 8. Few studies have addressed the spec ific
muc osal immune response in c hildhood TB or rec ognized the
importanc e of sIgA in muc osal homeostasis in the respiratory
trac t. In this regard, the present researc h studied the levels of
anti-PPD and 3 8 kDa sIgA in a Warao c hild population with TB. Th e r e s ults m igh t pa r tia lly c o n tr ib ute to e xpla in in g th e
extraordinarily high prevalenc e of c hildren with ac tive TB present
in this population.
MATERIAL AND METHODS
I n a r e m o te a r e a o f a n in dige n o us po pula tio n fr o m
no r the aste r n Ve ne zue la, a study was c o nduc te d in 1 5 War ao
indige no us c o mmunitie s fr o m two Munic ipal Distr ic ts o f the
Delta Amac uro State ( Tuc upita and Antonio Díaz) . A total of 1 2 7 saliva samples were c ollec ted from c hildren of both genders,
aged 1 month to 1 5 years. The mean age of c ases was 8 .0 9 ± 3 .8 0
years old. Radiologic al studies suggested that 3 1 c hildren were strong TB suspects. The children were grouped as follows: Patient
Group, c hildren with probable ac tive TB before treatment ( n= 3 1 ,
2 5 positive and 6 negative for the TST) ; Control Group, healthy
c ontac t c ontrols ( n= 9 6 , 5 3 positive and 4 3 negative for the TST) . The latter gro up was evaluated and no -o ne was fo und with
c harac teristic signs suggesting TB . A sec ond c ontrol group of
4 0 c hildr e n fr o m Car ac as do nate d saliva sam ple s fo r the
determinatio n o f no rmal sIgA levels. Info rmed c o nsent was o btained fro m all partic ipants o r their legal representatives
( c hildren or parents, respec tively) , who signed a c onsent form agreement before blood and saliva samples were taken. The
approved c onsent of the Ethic al Commission of the Biomedic ine Institute was also obtained.
Dur ing the pr e se nt study spe c ific atte ntio n was give n to
Wa r a o c h ildr e n le s s th a n 1 5 ye a r s o ld with r e s pir a to r y
sym pto m s. I n this r e gar d, a sc he m e pr e vio usly r e po r te d b y
o ur r e se ar c h gr o up was use d2 0, whic h tak e s into ac c o unt
th e c lin ic a l a n d e p ide m io lo gic a l c r ite r ia th a t c h ildr e n
pr e se nte d: 1 ) c linic al and nutr itio nal c r ite r ia and po sitive
r e a c tivity to tub e r c ulin , a n d 2 ) c lin ic a l a n d n utr itio n a l
c r ite r ia, with ne gative tub e r c ulin and po sitive ho use ho ld c o n ta c t. Ch i l d r e n th a t we r e TB s u s p e c ts we r e fu r th e r
e valuate d with a c he st X- r ay.
Clinical, epidemiological and bacter iological cr iter ia for tuber culosis diagnosis. Sinc e 1 9 9 6 , the Regional Program of Tuberc ulosis of Delta Amac uro State and the Tuberc ulosis Laboratory of the Institute of Biomedic ine have ac tively diagnosed
tuberc ulosis c ases among the Warao c ommunities based on
respiratory symptoms c harac teristic of TB, the TST and smears
and/or c ultures, and presc ribed spec ific treatments.
Clinic a l a nd nutr itio na l c r ite r ia . A c o m ple te b asic c linic al and nutr itio nal e valuatio n was c ar r ie d o ut. The latte r
was b ase d o n an anthr o po m e tr ic e valuatio n, c o ntaine d in
the Tr ansve r sal Study o f Car ac as, Fundac r e de sa3. The c linic al
e va l u a ti o n i n c l u de d: r e c e n t we i gh t l o s s o r i n a de q u a te
pr o gr e ss o f we ight gain; pr o lo nge d fe b r ile syndr o m e ; night
swe ats; c o ughing o r whe e zing fo r m o r e than two we e k s;
lar ge painle ss ade no pathy, with o r witho ut fistulas; angular
de fo r m ity o f the spine ; inc r e ase d ar tic ular o r b o ne vo lum e ,
o r fistulas; ine xplic ab le ab do minal mass o r asc itis; b e havio r
o r s e n s o r y s ys te m a l te r a ti o n s ; a n y o th e r n e u r o l o gi c a l
m a n ife s ta tio n s ugge s tive o f tub e r c ulo us m e n in gitis ; a n d
r e gistr atio n o f the pr e se nc e o r ab se nc e o f B CG sc ar s.
Ra dio lo gica l cr ite r ia . Tho r ax r adio lo gy was pe r fo r me d o n all highly suspe c t c ase s ac c o r ding to standar d te c hnique s
in po st-ante r io r pr o j e c tio n. This to o k plac e in the r adio lo gy se r vic e o f the Ho spital Luis Razze tti, Tuc upita. Radio lo gic al
e valuatio n was pe r fo r me d b y two pne umo no lo gists.
Epidemiologic al c riteria.A c omplete basic epidemiologic al
evaluation was c arried out, whic h was based on the TST and
household c ontac ts, defined as c ontinuous c ontac t with an adult
patient with ac tive lung tuberc ulosis or who had rec ently rec eived
The tube r culin skin te st. TheTSTs we r e pe r fo r me d o n all the individuals o f this study using two tub e r c ulin units o f
p u r i fi e d p r o te i n d e r i va ti ve ( P P D ) o f Myc o b a c te r i u m
tub er c ulo sis, str ain RT-2 3 , fr o m the State ns Se r uminstitut in Co pe n h a ge n , De n m a r k . Te s tin g a n d r e a din g we r e do n e
ac c o r ding to inte r natio nal guide line s2; indur atio n o f ³ 1 0 mm
was use d as the c r ite r io n fo r infe c tio n with M. tub e r c ulo sis.
Ba c te r io lo gic a l c r ite r ia . Sinc e invasive pr o c e dur e s c anno t b e use d to tak e sample s in the se c o mmunitie s, a study
o f se c r e tio ns o f the phar ynx and atte mpts to o b tain sample s
o f sputum b y e xpe c to r atio n in o lde r c hildr e n was c ar r ie d o ut in all highly suspe c t c ase s. Sme ar s fr o m sputum we r e staine d
b y the Zie hl-Ne e lse n dir e c t me tho d. Fo r e ac h spe c ime n two
tub e s o f mo difie d Ogawa e gg me dium and Lo wë nste in-Je nse n
we r e ino c ulate d using the swab me tho d o f Kudo h and Kudo h,
fo r b o th sputum and o o zing se c r e tio ns1 9.
Tr e a tme nt o f tube r culo sis. Spe c ific tr e atme nts we r e initiate d fo llo wing the no r m s o f the Ve ne zue lan Natio nal
Pr o gr am o f Tub er c ulo sis Co ntr o l6 in all newly identified c ases
o f tub e r c ulo sis, whe r e r adio lo gic al e vide nc e sugge stive o f tub e r c ulo sis o r b ac te r io lo gic al c o nfir matio n b y b ac illo sc o py
o r c ultur e was fo und. Clinic al and nutr itio nal mo nito r ing in
all highly suspe c t patie nts was c ar r ie d o ut, to e valuate the
impr o ve me nt o f the se aspe c ts as the r ape utic e vide nc e , whic h allo we d fo r the c o r r o b o r atio n o f the diagno sis.
De te r mina tio n o f the a ntibo die s o f Myco ba cte r ium tube r culo sis a ntige ns. Anti-PPD sIgA:the detec tio n o f anti-PPD sIgA le ve ls was pe r fo r me d b y c aptur e immuno e nzymatic
assays ( ELISA) . The assay was de ve lo pe d and standar dize d in o ur labo rato ry fo r the detec tio n o f sIgA against PPD antigen.
Eac h individual assay inc lude d po sitive and ne gative se r a and
also b lank s to c o ntr o l no n-spe c ific b inding. Mic r o tite r plate s
( ThermoLabsystems) , Dynatec h Laboratories, Inc .) were c oated
with PPD (Statens Seruminstitut, Copenhagen) ( 1
µ
g/well inc a r b o n a te - b ic a r b o n a te b uffe r pH 9 . 6 ) o ve r n igh t a t 4 ° C. Exc e ss pr o te in b inding site s we r e b lo c k e d b y inc ub atio n with ho r se se r um in PB S ( 1 :3 0 ) at 3 7 ° C fo r 2 h, the n the plate s we r e washe d fo ur time s with PB S c o ntaining 0 .1 % Twe e n 2 0 . Optimal dilutio ns o f saliva sample s ( 1 :5 0 ) we r e adde d and
plate s we r e inc ub ate d fo r 2 h at 3 7 ° C and washe d fo ur time s;
then inc ubated fo r 1 ho ur at 3 7 ° C with the sec o ndary antibo dy fo r s I gA ( p e r o x i da s e - c o n j u ga te d m o n o c l o n a l a n ti b o dy
anti- alpha c hain I gA, Sigm a- Aldr ic h, USA, dilute d) . Afte r
washing, sub str ate so lutio n ( 3 0
µ
l o f 3 0 % H2O2 and 1 0 mg
o -phenylenediamine ( OPD) dihydro c hlo ride, (Sigma-Aldric h,
USA) in 2 5 ml c itr ate b uffe r, pH 5 ) was adde d and inc ub ate d
fo r 1 6 minute s at r o o m te mpe r atur e . Co lo r de ve lo pme nt was me asur e d in an ELISA r e ade r at 4 9 2 nm.
Anti-3 8 k Da sIgA: the le ve ls o f anti-3 8 k Da sIgA in saliva wer e deter mined b y a similar ELISA to that desc r ib ed fo r
anti-PPD sIgA. B riefly, mic ro titer plates ( Thermo Labsystems) were
c o ated o ver night at 4 ° C with 3 8 kDa antigen ( 1
µ
g/well o f eac hantige n in c ar b o nate -b ic ar b o nate b uffe r pH 9 .6 ) . The saliva
s a m p l e s we r e di l u te d 1 : 5 0 a n d p e r o x i da s e - c o n j u ga te d mo no c lo nal antib o dy anti-alpha c hain IgA ( Sigma-Aldr ic h, USA) was use d as the se c o ndar y antib o dy dilute d.
Sta tistica l a na lysis. The statistic al signific anc e o f the differenc es between the mean ± SD of the optic al density ( OD)
values of the patients and c ontrols was estimated by the Students “t” test. The evaluation of positive saliva was based on a positive
sc ore represented by levels greater than OD mean plus two
standar d deviatio ns o f saliva fr o m a healthy c o ntr o l gr o up
negative for the TST from Carac as in north-c entral Venezuela. The proportions of patients with positive results for the different
evaluations were c ompared by Fisher’s exac t test.
RESULTS
Se c r e to r y I gA s p e c ific le ve ls a c c o r d in g to th e tube r c ulin s kin te s t. The r e sults in r e latio n to the TST
sho we d thatin the TB patie nt gr o up, 2 5 we r e po sitive fo r the
tub e r c ulin sk in te st ( TST) and 6 ne gative fo r the TST; and in
the he althy c o ntac t c hildr e n, 5 3 we r e po sitive fo r the TST and 4 3 ne gative fo r the TST ( Tab le 1 ) .
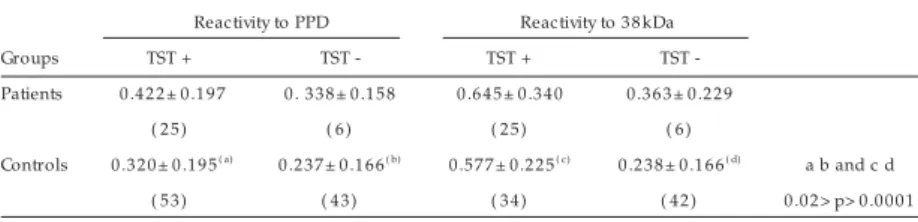
The mean ± SD of the optic al density ( OD) values of anti-PPD and anti-3 8 kDa sIgA levels of patient and c ontrol c hildren
are shown in Table 1 . In relation to the mean anti-PPD sIgA levels, in the patient group, there was no statistic ally signific ant
differenc e between patients positive and negative for the TST ( 0 .4 2 2 ± 0 .1 9 7 and 0 .3 3 8 ± 0 .1 5 8 , respec tively) . In the c ontrol
gr o up, th e m e a n a n ti- PPD s I gA le ve ls we r e s ign ific a n tly i n c r e a s e d i n th e c o n tr o l gr o u p p o s i ti ve fo r th e T S T
( 0 .3 2 0 ± 0 .1 9 5 ) , in c omparison to the c ontrol group negative for the TST ( 0 .2 3 7 ± 0 .1 6 6 ) , p< 0 .0 2 , ( Table 1 ) .
In r e latio n to the me an anti-3 8 k Da sIgA le ve ls, in the patient gro up, altho ugh patients po sitive fo r the TST presented
a h igh m e a n o f th e s e le ve ls , th e r e wa s n o s ta tis tic a lly
signific ant diffe r e nc e b e twe e n patie nts po sitive and ne gative
fo r the TST ( 0 .6 4 5 ± 0 .3 4 0 and 0 .3 6 3 ± 0 .2 2 9 , r e spe c tive ly) . In the c o ntr o l gr o up, the me an anti-3 8 k Da sIgA le ve ls we r e signific antly inc r e ase d in the c o ntr o l gr o up po sitive fo r the
Table 1 - Specific sIgA levels in patients and controls according to the response to the tuberculin skin test. Reactivity to PPD Reactivity to 3 8 kDa
Groups TST + TST - TST + TST
-Patients 0 .4 2 2 ± 0 .1 9 7 0 . 3 3 8 ± 0 .1 5 8 0 .6 4 5 ± 0 .3 4 0 0 .3 6 3 ± 0 .2 2 9
( 2 5 ) ( 6 ) ( 2 5 ) ( 6 )
Controls 0 .3 2 0 ± 0 .1 9 5( a) 0 .2 3 7 ± 0 .1 6 6( b) 0 .5 7 7 ± 0 .2 2 5( c) 0 .2 3 8 ± 0 .1 6 6( d) a b and c d
TST ( 0 . 5 7 7 ± 0 . 2 2 5 ) , in c o m par iso n to the c o ntr o l gr o up ne gative fo r the TST ( 0 .2 3 8 ± 0 .1 6 6 ) , p< 0 .0 0 0 1 ( Tab le 1 ) .
When the results are shown as percentage of children with antibodies to specific antigens according to the tuberculin skin test, it was found that regarding the sIgA specific response against PPD according to the TST, salivas from patients positive for the TST presented a significant percentage of patients with specific
sIgA ( 1 4 .2 %) in comparison to patients negative for the TST ( 0 %) . The Figure 1 sho ws that in the c ontrol group, there was no significant difference between controls positive and negative for the TST ( 3 .7 % and 4 .6 %, respectively) .
The pe r c e ntage s o f patie nts and c o ntr o ls with po sitive responses to 3 8 kDa antigen according to the TST are shown in Figure 2 . Regarding the sIgA specific response according to the TST, in patient group, there was statistically significant differences in patients positive for the TST that presented anti-3 8 kDa levels ( 2 8 %) in comparison to patients and controls negative for the TST ( 1 6 .6 % and 7 .1 %, respectively) , p< 0 .0 4 ( Figure 2 ) . Those
patients positive for the TST presented twice the anti-3 8 kDa sIgA levels in comparison to those that produced anti-PPD sIgA levels. There was no statistically significant differences in the percentage
of controls with specific anti-3 8 kDa sIgA response between children
positive and negative for the TST.
DISCUSSION
Sinc e in indige no us Wa r a o c o m m unitie s in a r e m o te
indigeno us po pulatio n fro m no rth-eastern Venezuela, invasive pr o c e dur e s c anno t b e use d to tak e sample s due to e thic al
c o nside r atio ns, the asse ssme nt o f TB amo ng a po pulatio n o f
c hildr en with an high pr evalenc e o f ac tive TB in adults o ffer ed
a n o ppo r tunity to study the de ve lo pm e nt o f the m uc o sa l defenc e mec hanisms mediated by sIgA against M. tuberc ulosis antige ns and to atte mpt to impr o ve diagno stic me tho ds, suc h
as the spe c ific sIgA te st.
The role of type-2 responses and humoral immunity in TB
infec tion is generally c onsidered to be marginal1 5 3 4. However,
bearing in mind that the identification of receptors for IgA on the
surface of blood leukocytes and alveolar macrophages that perform
a protective role in chronic respiratory infections, such as TB, has
been reported and that this provides a measure of the integrity of
the spec ific muc osal response to M. Tuberc ulosi1 6 2 2 2 5 3 2, the
measurement of specific sIgA was carried out. Concerning the
anti-PPD sIgA antibody response and the response to the TST, while
patients positive for the TST presented antibodies reactive to PPD antigen, no tuberc ulin negative patients presented antibodies
reactive to this antigen, so the latter correlates with a lack of the
cellular specific response in these children. The results show that
child patients produced M. tuberculosis-reactive sIgA antibodies during active infection; moreover, children in this patient group
failed to react to PPD, as has been suggested by other studies which
showed that during active TB, signs of immune depression were
related to the presenc e of a signific ant immune depression in
response to the TST and with antibody test unresponsiveness or
anergy, when PPD was used7. In addition, it has been reported that
in another approach, when a correlation was found between the
presence of TB disease and anti-PPD sIgA, 7 % of patients displayed
a selective sIgA deficiency3 5. the present findings suggest that an
absence of this specific sIgA immune defence in a percentage of
these children does occur, which might be associated with higher
susceptibility to TB and probably to other infections, particularly
acute respiratory tract infections that are frequently observed in
these childhood communities1 0. On the other hand, other factors
could be involved, such as nutritional status, type of feeding7 and
genetic aspects6 2 1 2 7, alternatively, proinflammatory factors, such as
cytokines ( for example, IL-6) , traditionally involved in the polyclonal
activation seen in TB, may play a role in sIgA elevation1 3 1 8. In this
regard, several studies have reported that the human airway epithelium constitutively produces IL-2 , TGF-beta, IL-6 and IL-1 0 ,
factors which are essential for B-cell clonal proliferation, IgA isotype
switc h and differentiation into IgA-produc ing plasma c ells5 1 1.
Additionally, it has been reported that a transient absence of salivary IgA in the first years of life was associated with an increased risk of
developing atopy, asthma or bronchial hyperreactivity later in life23 24;
whereas low levels of salivary IgA, partic ularly the IgA1 subc lass,
have b e e n asso c iate d with an inc r e ase d r isk o f r e spir ato r y
illne ss8.
In relation to the anti-3 8 kDa muc osal response, a signific ant perc entage of both tuberc ulin positive patients and c o ntr o ls, 1 6 TST+ TST-1 4 1 2 1 0 8 6 4 2 0
Patients Contr ols
SIgA antibodies to PPD P ercenta ge (%) M. Tuberculosis
Data r e pr e se nting the pe r c e ntage s o f patie nts ( n= 3 1 ) and c o ntr o ls ( n= 9 6 ) .
Figur e 1 - Anti- PPD sIgA a cco r ding to the tube r culin skin te st.
Data r e pr e se nting the pe r c e ntage s o f patie nts ( n= 3 1 ) and c o ntr o ls ( n= 9 6 ) . * The r e was statistic ally signific ant diffe r e nc e s in patie nts TST + that pr e se nte d anti- 3 8 k Da le ve ls in c o mpar iso n to patie nts and c o ntr o ls TST- , p< 0 . 0 4
Figur e 2 - Anti- 3 8 kDa sIgA a cco r ding to the tube r culin skin te st. TST+ TST-3 0 2 5 2 0 1 5 1 0 5 0
Patients Contr ols
and even a perc entage of tuberc ulin negative patients, produc ed
anti-3 8 kDa sIgA antibodies, whic h c ould be due to the fac t that the muc osal immune system in these c hildren is assoc iated with
an appropriate muc osal immune response that it is c apable of
mounting a better response to 3 8 kDa antigen than the PPD
antigen. The similar lower perc entage of tuberc ulin negative c ontrols with reac tivity to 3 8 kDa and PPD c ould be c onditioned
by a high prevalenc e of atypic al myc obac teria, whic h c an induc e
a c ross-reac ting antibody immune response. Although in the
pr e se nc e o f ac tive infe c tio n a c e r tain am o unt o f im m une depression related to PPD antibody test unresponsiveness or
anergy oc c urred, the sIgA antibodies to 3 8 kDa antigen were
produc ed both in patients positive and negative for the TST.
Bearing in mind that the use of ELISA for immunodiagnosis of TB has shown that the sensitivity of the tests remained limited in
the diagnosis of c hildhood TB2 9 3 0 3 1, and sinc e the immunologic al
ac tivity of 3 8 kDa antigen of M. tuberc ulosis has been reported
and used for the serodiagnosis of TB3 6, it seems important that a
c ombination inc luding anti-3 8 kDa sIgA provided improvement
in the diagnosis of this population, as previously reported by
our group1.
Fe w s tudie s h a ve a ddr e s s e d th e de pr e s s io n o f b o th
d e l a ye d - typ e h yp e r s e n s i ti vi ty, m a n i fe s t a s d e p r e s s e d tub e r c ulin s k in te s t r e a c tio n , a n d th e s I gA r e s p o n s e to
M. tub e r c ulo sis antige ns, the pr e se nt study pe r mitte d the s ugge s tio n th a t in th e Wa r a o c h ildh o o d po pula tio n wh e r e M. tub e r c ulo sis infe c tio n is pr e vale nt, the r e was a c le ar se par atio n o f the two sIgA spe c ific r e spo nse s. The se antige ns
se e m to b e asso c iate d with a distinc t de ve lo pme nt o f the
m uc o s a l de fe n c e m e c h a n is m s m e dia te d b y s I gA a ga in s t M. tuberc ulosis. The identific ation of these muc osal mec hanisms c o uld be mo re c learly defined in future studies, leading to
improved diagnosis of c hildhood TB and the design of targeted
muc osal vac c ines.
ACKNOWLEDGEMENTS
The autho r s ar e inde b te d to Mar k Gr e gso n fo r his c r itic al review o f the manusc ript and wo uld also like to thank Mic hael Ar auj o fo r his te c hnic al assistanc e .
REFERENCES
1 . Ar a uj o Z, Wa a r d J H, La r r e a CF, Ló pe z D, Fa n diñ o C, Ma ldo n a do A,
He r nánde z E, Oc aña Y, Or te ga R, Singh M, Otte nho ff To m HM, Ar e nd SM,
Co n vit J . Study o f th e R e s po n s e a ga in s t Myc o b a c te r ium tub e r c ulo s is
Antigens in War ao amer indian Childr en in Venezuela. Memó r ias do Instituto
Oswaldo Cr uz 9 9 : 5 1 7 - 5 2 4 , 2 0 0 4 .
2 . Ar nado ttir T, Rie de r HL, Tr é b uq A, Waale r H. Guide line s fo r c o nduc ting
tub e r c ulin sk in te st sur ve ys in high pr e vale nc e c o untr ie s. Tub e r c le and
Lung Dise ase 7 7 : 1 - 2 0 , 1 9 9 6 .
3 . B l a n c o M L, La n d a e t a M . M a n u a l d e Cr e c i m i e n t o y D e s a r r o l l o .
Fundac r e de sa. Car ac as, 1 9 9 1 .
4 . B o yaka PN, Lillar d Jr JW, Mc Ghee J. Inter leukin 1 2 and innate mo lec ules fo r
enhanc ed muc o sal immunity. Immuno lo gic Resear c h 2 0 : 2 0 7 -2 1 7 , 1 9 9 9 .
5 . B r ac iak TA, Gallic han WS, Gr aham FL, Ric har ds CD, Ramsay AJ , Ro se nthal
KL, Gauldie J. Re c o mb inant ade no vir us ve c to r s e xpr e ssing inte r le uk in-5
and- 6 spe c ific ally e nhanc e muc o sal immuno glo b ulin A r e spo nse s in the lung. Immuno lo gy 1 0 1 : 3 8 8 - 3 9 6 , 2 0 0 0 .
6 . Da vie s P, Gr a nge J . The ge ne tic s o f ho st r e sista nc e a nd susc e ptib ility
tub er c ulo sis. Annals o f New Yo r k Ac ademy o f Sc ienc es 9 5 3 : 1 5 1 -1 5 6 , 2 0 0 1 .
7 . Gatne r EM, Ande r so n R. An in vitr o asse ssme nt o f c e llular and humo r al
im m un e fun c tio n in pulm o n a r y tub e r c ulo s is : c o r r e c tio n o f de fe c tive
ne utr o phil mo tility b y asc o r b ate , le vamiso le , me to pr o lo l and pr o pano lo l. Clinic al and Expe r ime ntal Immuno lo gy 4 0 : 3 2 7 - 3 3 6 , 1 9 8 0 .
8 . Gle e so n M. Muc o sal im m unity and r e spir ato r y illne ss in e lite athle te s.
Inte r natio nal J o ur nal o f Spo r ts Me dic ine 2 1 3 3 - 4 3 , 2 0 0 0 .
9 . Gle e so n M, Cr ipps A, Clane y R. Mo difie r s o f the human muc o sal immune
syste m. Immuno lo gy and Ce ll B io lo gy 7 3 : 3 9 7 - 4 0 4 , 1 9 9 5 .
1 0 . Go nzále z N, De Cub e ddu L, Waar d J H, Fandiño C, Lar r e a CF, Ló pe z D, Maldo nado A, Oc aña Y, He r nánde z E, Or te ga R, Co nvit J , Puj o l FH, Casté s M, Ar auj o Z. Study o f the immune r e spo nse in War ao c hildr e n fr o m an ar e a with high pr e vale nc e o f tub e r c ulo sis. Inve stigac ió n Clínic a 4 4 : 3 0 3 -3 1 8 , 2 0 0 -3 .
1 1 . Go o dr ic h ME, Mc Ge e DW. Effe c t o f inte stinal e pithe lial c e ll c yto k ine s o n muc o sal B - c e ll IgA se c r e tio n: e nhanc ing e ffe c t o f e pithe lial- de r ive d IL- 6 b ut no t TGF- b e ta o n IgA+ B c e lls. Immuno lo gy Le tte r s 6 7 : 1 1 - 1 4 , 1 9 9 9 .
1 2 . Ho lm gr e n J , Rudin A. Muc o s a l I m m un ity a n d B a c te r ia l. I n : Muc o s a l Immuno lo gy. Se c o nd e ditio n, Chapte r 4 1 . Ac ade mic Pr e ss USA, p. 6 8 5 -6 9 0 , 1 9 9 9 .
1 3 . Huc kleb r idge F, Clo w A, Evans P. The r elatio nship b etween salivar y sec r eto r y immuno glo b ulin A and c o r tiso l: ne ur o e ndo c r ine r e spo nse to awak e ning and the diur nal c yc le . Inte r natio nal J o ur nal o f Psyc ho physio lo gy 3 1 : 6 9 -7 6 , 1 9 9 8 .
1 4 . J e m m o tt 3r d J B , B o r ys e n k o J Z, B o r ys e n k o M. Ac a de m ic s tr e s s , po we r
m o ti va ti o n , a n d d e c r e a s e i n s e c r e ti o n r a te o f s a l i va r y s e c r e to r y
immuno glo b ulin A. Lanc e t 1 : 1 4 0 0 - 1 4 0 2 , 1 9 8 3 .
1 5 . Kamat HA, Williamso n M, Ko ppik ar GV. Humo r al and c e ll me diate d immune r espo nses in patient with tub er c ulo sis meningitis. Indian Jo ur nal o f Medic al Sc ie nc e s 5 3 : 3 4 3 -3 4 8 , 1 9 9 9 .
1 6 . Kitz R, Ahr e ns P, Zie le n S. Immuno glo b ulin le ve ls in b r o nc ho alve o lar lavage fluid o f c h ildr e n with c h r o n ic c h e s t dis e a s e . Pe dia tr ic Pulm o n o lo gy 2 9 : 4 4 3 - 4 5 1 , 2 0 0 0 .
1 7 . Kiyo no H, Kwe o n MN, Hir o i T, Tak ahashi I. The muc o sal immune syste m: fr o m s pe c ia lize d im m un e de fe n s e to in fla m m a tio n a n d a lle r gy. Ac ta Odo nto lo gic a Sc andinavic a 5 9 : 1 4 5 -1 5 3 , 2 0 0 1 .
1 8 . Kr ame r DR, Suthe r land RM, B ao S, Husb and AJ . Cyto k ine me diate d e ffe c ts in muc o sal immunity. Immuno lo gy and Ce ll B io lo gy 7 3 : 3 8 9 - 3 9 6 , 1 9 9 5 .
1 9 . Kudo h S, Kudo h T. A simple tec hnique fo r c ultur ing tub er c le b ac illi. B ulletin o f the Wo r ld He alth Or ganizatio n 5 1 : 7 1 - 8 2 , 1 9 7 4 .
2 0 . Lar r e a CF, FandiñoC, Ló pe z D, de l No gal B , Ro dr ígue z N, Co nvit J , Ar auj o
Z, Waar d JH. Childho o d tub e r c ulo sis in the War ao po pulatio n in Ve ne zue la. Inve stigac ió n Clínic a 4 3 : 3 5 - 4 8 , 2 0 0 2 .
2 1 . Layr isse Z, He ine n HD, B alb as O, Gar c ía E, Sto ik o w Z. Uniq ue HLA- DR/DQ asso c iatio ns r e ve ale d b y family studie s in War ao ame r indians. Haplo type and ho mo zygo sity fr e q ue nc ie s. Human Immuno lo gy 2 3 : 4 5 - 5 7 , 1 9 8 8 .
2 2 . Lugto n I. Muc o sal-asso c iate d lympho id tissue s as site s fo r uptak e , c ar r iage a nd e xc r e tio n o f tub e r c le b a c illi a nd o the r pa tho ge nic m yc o b a c te r ia . Immuno lo gy and Ce ll B io lo gy 7 7 : 3 6 4 - 3 7 2 , 1 9 9 9 .
2 3 . Mar e e G, Cr ipps AW, Clanc y RL. Mo difie r s o f the human muc o sal immune syste m. Immuno lo gy and Ce ll B io lo gy 7 3 : 3 9 7 - 4 0 4 , 1 9 9 5 .
2 4 . Miletic ID, Sc hiffman SS, Miletic VD, Sattely-Miller EA. Salivar y IgA sec r etio n r ate in yo ung and elder y per so ns. Physio lo gy & B ehavio r 6 0 : 2 4 3 -2 4 8 , 1 9 9 6 .
2 5 . Nagao AT, Pilagallo MI, Pe r e ir a AB . Quantitatio n o f salivar y, ur inar y and fae c al sIgA in c hildr e n living in diffe r e nt c o nditio ns o f antige nic e xpo sur e . J o ur nal o f Tr o pic al Pe diatr ic s 3 9 : 2 7 8 - 2 8 3 , 1 9 9 3 .
2 7 . Ramo s M, Po stigo J M, Vilc he s C, Layr isse Z, Castr o J AL. Pr imar y str uc tur e o f a no ve l HLA- B 3 9 alle le ( B * 3 9 0 9 ) fr o m the War ao Indians o f Ve ne zue la. Fur the r e vide nc e fo r lo c al HLA- B dive r sific atio n in So uth Ame r ic a. Tissue Antige ns 4 6 : 4 0 1 - 4 0 4 , 1 9 9 5 .
2 8 . Re lj ic R, Clar k SO, Williams A, Fale r o - Díaz G, Singh M, Challac o mb e S, Mar sh PD, Ivanvi J. Intr anasal IFNgamma e xte nds passive IgA antib o dy pr o te c tio n o f m ic e against Myc o b ac te r ium tub e r c ulo sis lung infe c tio n. Clinic al Expe r ime ntal Immuno lo gy 1 4 3 : 4 6 7 - 4 7 3 , 2 0 0 6 .
2 9 . Sant’Anna CC, Fe r r e ir a MAS, Fo nse c a LS. Evaluatio n o f a se r o lo gic al me tho d ( ELI SA) fo r the diagno sis o f pulm o nar y tub e r c ulo sis in c hildr e n. The Inte r natio nal J o ur nal o f Tub e r c ulo sis and Lung Dise ase 3 : 7 4 4 -7 4 8 , 1 9 9 9 .
3 0 . Star k e J R. Childho o d tub e r c ulo sis: a diagno stic dile mma. Che st 1 0 4 : 3 2 9 -3 -3 0 , 1 9 9 -3 .
3 1 . Swaminathan S, Umade vi P, Shantha S, Radhak r ishnan A, Datta 0 . Se r o diagno sis o f tub e r c ulo sis in c hildr e n using two ELISA k its. Indian J o ur nal o f Pe diatr ic s 6 6 : 8 3 7 - 8 8 4 , 1 9 9 9 .
3 2 . Tamada T, Sasak i T. The r o le o f air way sub muc o sal glands in the air way m uc o s a l de fe n s e s ys te m . Nih o n Ko k yuk i Ga k k a i Za s s h i 3 9 : 1 5 7 - 1 6 5 , 2 0 0 1 .
3 3 . To mo da T, Tak ai A. Tub e r c le b ac illi and the de fe nc e fac to r s fo r infe c tio n in sputum and b r o nc ho alve o lar lavage fluid. Ke k k ak u 6 9 : 7 4 3 - 7 4 9 , 1 9 9 4 .
3 4 . Van Cr e ve l R, Otte nho ff THM, van de r Me e r J WM. I nnate im m unity to Myc o b ac te r ium tub e r c ulo sis. Clinic al Mic r o b io lo gy Re vie ws. 1 5 : 2 9 4 -3 0 9 , 2 0 0 2 .
3 5 . Watso n RR, Mc Mur r ay DN. The e ffe c ts o f malnutr itio n o n se c r e to r y and c e llular im m une pr o c e sse s. CRC Cr itic al Re vie ws in Fo o d Sc ie nc e and Nutr itio n 1 2 : 1 1 3 - 1 5 9 , 1 9 7 9
3 6 . Yo ung D, Ke nt L, Re e s A, Lamb J , Ivanyi, J . Immuno lo gic al ac tivity o f a 3 8 -k ilo dalto n pur ifie d fr o m Myc o b ac te r ium tub e r c ulo sis. Infe c tio n Immunity 5 4 : 1 7 7 - 1 8 3 , 1 9 8 6 .