THE JAMAICAN
HYPERTENSIVE:
CHARACTERISTICS
OF BLACK
PATIENTS
AT THE UNIVERSITY
HOSPITAL
OF THE WEST INDIES’
Gerald A. C. Grel12
Hypertension is the most common chronic disease of adults in the Caribbean, affecting some 22% of the population. This article reports the results of a prospective study of 286 hospitalized black hypertensive subjects that was designed to help elucidate prevailing features of the disease in this region,
Introduction
Hypertension is the most common chronic dis- ease of adults in the Caribbean today, affecting some 22% of this population (I); as a result, it contributes directly and indirectly to the leading causes of death in most of the English-speaking islands (2).
While many epidemiologic surveys (3, 4, 5) have defined the prevalence of this disease in the community, there are very few studies that document the clinical problems associated with hypertension in Jamaica. This article provides some basic data about the clinical characteristics of the black hypertensive Jamaican and supplies information useful for comparison with popula- tions from other parts of the world.
Black hypertensives in Africa and the Carib- bean and those in the United States and United Kingdom exhibit some interesting similarities; but with increasing “Westernization,” changes in the pattern of the disease can be expected. Comparative studies will help to separate those differences that may properly be attributed to ethnic factors from those which are largely de- termined by environmental variables.
‘This article will also be published in Spanish in the
Boletin de la Ojicina Sanitaria Panamericana, 1985. ‘Senior Lecturer in Medicine and Director, Hypertension Research Clinic, University of the West Indies Department of Medicine, Mona Campus, Kingston 7, Jamaica.
Materials and Methods
Jamaica, with a population of 2,085,000, is situated at the northwest end of the Greater An- tilles chain of islands which were formerly British colonies. The University Hospital of the West Indies (UHWI), with a bed capacity of 506, is located in Kingston, the capital of Jamaica; and while admissions are predominantly from within that island, referrals are accepted from all of the 14 territories that contribute to the University of the West Indies, a regional institu- tion. Some 16,097 patients were admitted in 1981, 2,158 to the medical wards with a bed complement of 100 and an average length of stay of 10 days.
Data were collected from all male and female hypertensives admitted consecutively to the medical wards at the UHWI during the two-year period extending from 1 January 1980 through 3 1 December 198 1. Patients satisfying the criteria for inclusion in the study were those (1) who were confirmed to be hypertensive on previous hospitalization at the UHWI with recorded sys- tolic and diastolic blood pressures in excess of 160195 mmHg, or (2) who were known hyper- tensives requiring antihypertensive therapy at some time prior to admission, or (3) who had to be placed on antihypertensive medication during the hospital stay under study, or (4) whose sys- tolic and diastolic blood pressures recorded during the current period of hospitalization exceeded
160/95 mmHg on at least three successive read- Age, Sex, and Social Characteristics of the
ings. Black Study Subjects
All subjects studied were interviewed indi- vidually in the wards, and a questionnaire was completed relating details of each patient’s his- tory, clinical presentation, complications, tests, and management. Each case was reviewed again at the time of discharge from the hospital. In the event that the patient was unconscious or unable to speak, the interview was conducted with a relative or friend, or with the patient’s spouse.
The black study population included 149 males and 137 females. The age distribution of these subjects, by sex, is shown in Figure 1. As may be seen, most of the subjects were over 25 years old, with the 55-64 age group being the largest of the ten-year age groups covered. In all, some 72% of the males and 70% of the females were between 45 and 74 years old.
The following blood tests were performed for each patient: hemoglobin, packed cell volume, creatinine, urea, electrolytes, blood glucose, cholesterol, and uric acid. In addition, as part of the study all subjects had their urine tested for albumin on admission, all had a chest X-ray, and all had a routine 12-lead electrocardiogram (ECG). If deemed necessary, other diagnostic procedures such as intravenous pyelograms were requested.
No significant difference was found between the average admission blood pressure of males versus females. The mean admission systolic and diastolic blood pressures for the whole sample of 286 subjects (mmHg&SD) was 176.8232.9 and 110.9k21.2, respectively.
The data obtained from the study subjects were recorded on especially designed forms pro- duced after discussion with statisticians and computer programmers at the University of the West Indies Computer Center, where analysis of the data was carried out. The statistical work performed included Student’s “t” test and X2 testing.
On the basis of the United Kingdom Registrar General’s classification (see Table l), less than 18% of the patients were in social classes I and II, while over 37% were in social classes IV and V. Myocardial infarction was seen twice as frequently in classes I and II as in classes IV and V.
Regarding parity, 15.5% of the female patients
Figure 1. Distribution of the 286 black hyperten- sive patients, by sex and ten-year age group.
MALE FEMALE
Results
The Population Profile
There were 313 patients who satisfied the criteria for hypertension as defined in this study. There were also four dominant racial groups involved, 286 subjects being black (of African origin), five East Indian, four Chinese, and three white. The racial background of 15 subjects was undetermined. Data relating to black patients were analyzed further in an effort to more pre- cisely define the characteristics of the disease among this group.
6574
5!x4
4554
3544
2534
< 25
1 1 I I i 1 1 I
30 20 10 0 10 20 30
Grell 0 THE JAMAICAN HYPERTENSIVE 267
Table 1. The 286 black hypertensive patients grouped according to the U.K. Registrar General’s social class classification and by sex.
Social
class Occupational group
Males Females Total
NO. (%I NO. (%) NO. W) I Professional
II Intermediate occupations III Skilled occupations IV Partly skilled V Unskilled
Unemployed Unknown
Total
24 16.1 8 5.8 32 16 10.7 3 2.2 19 3.5 23.5 25 18.2 60 49 32.9 19 13.9 68 15 10.1 25 18.2 40 2 1.3 27 19.7 29 8 5.4 30 21.9 38 149 100 137 100 286
11.2 6.6 21.0 23.8 14.0 10.1 13.3 100
were nulliparous, while 26.4% had had more than four pregnancies. (An earlier study had sug- gested that both nulliparous Jamaican females and those who experienced toxemia of pregnan- cy were likely to have a higher prevalence of hypertension-o).
Cigarette smoking was more common among males (61.5% of whom were smokers) than among females ( 17.4% of whom were smokers). Males who drank alcohol also outnumbered female drinkers by a ratio of 5.3 to 1. Smoking was significantly associated (pcO.05) with ECG evidence of left ventricular hypertrophy (LVH), as was heavy alcohol consumption.
Overall, 39.6% of the males and 44.5% of
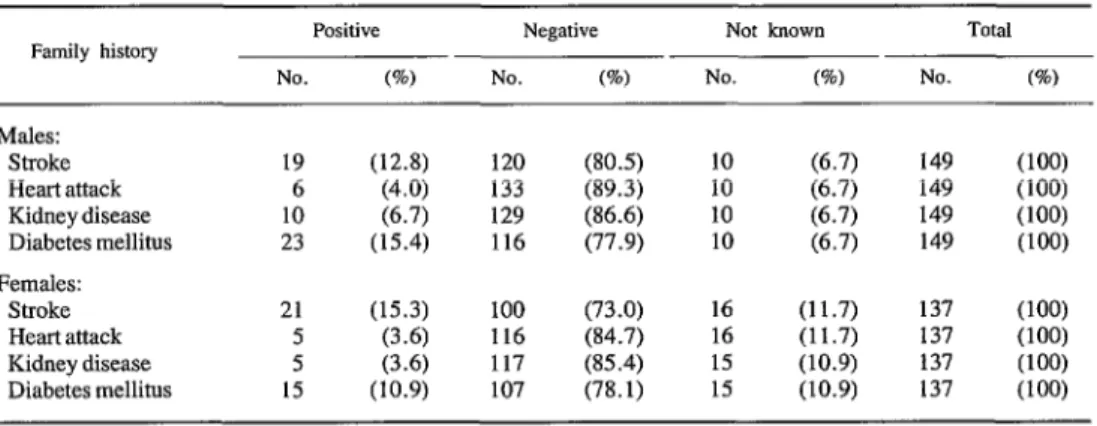
the females were found to have a positive family history of hypertension. The overall prevalence for males and females combined was 41.7%, as compared to the 68.5% documented by a Veter- an’s Administration study in the United States (7). As Table 2 shows, lesser percentages of the patients were found to have a family history of stroke, heart attack, kidney disease, or diabetes mellitus .
Etiology, Presenting Features, and Complications
Of the 286 patients investigated, 90.2% had essential hypertension, 9.1% showed evidence
Table 2. The black study subjects found to have a family history of diseases associated with hypertension (stroke, heart attack, kidney disease, and diabetes mellitus), by sex.
Family history Positive Negative Not known Total NO. (%) NO. (%) NO. (a) NO. (%) Males:
Stroke Heart attack Kidney disease Diabetes mellitus Females:
Stroke Heart attack Kidney disease Diabetes mellitus
of underlying renal disease, 0.3% (one patient) had a pheochromocytoma, and 0.3% (one pa- tient) had Corm’s syndrome (right adrenal aldos- terone producing adenoma) .
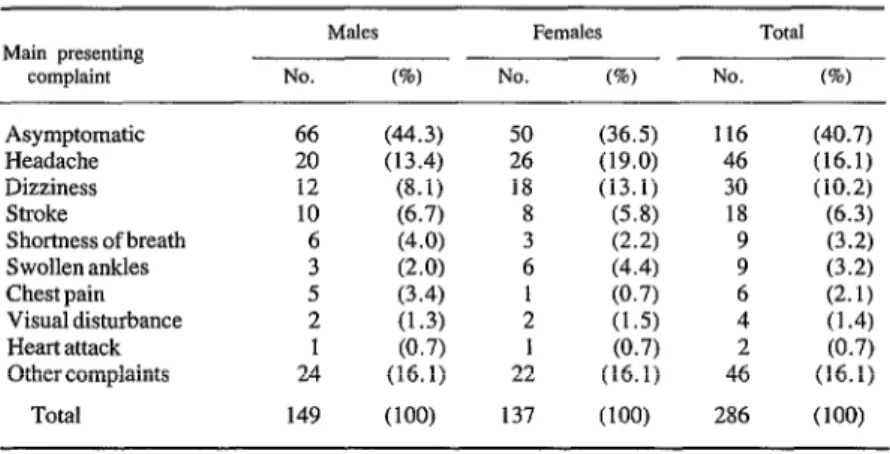
On initial presentation (at the time hyperten- sion was diagnosed) 40.7% of the subjects were asymptomatic; most had complaints such as headache, dizziness, and shortness of breath that were not specific for hypertension (Table 3).
As shown in Table 4, the most frequent com-
plications seen at the time of hospitalization in- cluded cardiomegaly (in 62.9%), renal impair- ment (in 48.6%), cardiac failure (in 35.3%), and cerebrovascular accident (in 27.3%). Myocar- dial infarction was diagnosed in 16.4% of the patients. Although ECGs showed that T wave inversions were not uncommon (being found in 42.3% of the subjects), these T wave abnormali- ties were largely related to left ventricular “strain” rather than ischemia.
TabIe 3. The main presenting complaint of the study subjects at the time of diagnosis, by sex.
Main presenting
complaint
Males Females Total NO. (%I NO. 0%) NO. (%I Asymptomatic 66 (44.3) 50 (36.5) 116 (40.7) Headache 20 (13.4) 26 (19.0) 46 (16.1) Dizziness 12 (8.1) 18 (13.1) 30 (10.2) Stroke 10 (6.7) 8 (5.8) 18 (6.3) Shortness of breath 6 (4.0) 3 (2.2) 9 (3.2) Swollen ankles 3 (2.0) 6 (4.4) 9 (3.2) Chest pain 5 (3.4) : (0.7) 6 (2.1)
Visual disturbance 2 (1.3) (1.5) 4 (1.4) Heart attack 1 (0.7) (0.7)
Othercomplaints 24 (16.1) 2:
(16.1)
4: (0.7) (16.1) Total 149 (100) 137 (100) 286 (100)
Table 4. The prevalence of complications involving likely target organ damage that were assessed at the time of the subject’s admission to the hospital. The data shown are for all 149 male and 137 female study subjects. In cases where multiple complications were found
in the patient, all the complications found have been included. Complication Males FeIlldeS Total
NO. (%I NO. (%) NO. (%I Cardiac enlargement
(on X-ray)
Left ventricular hypertrophy (on ECG)
Renal impairment” T wave changes (on ECG)b Cardiac failure
Cerebrovascular accident Myocardial infarction Angina1 chest pains Hypertensive encephalopathy Limb ischemia or gangrene
98 (65.8) 85 (57.0) 78 (52.3) 67 (45.0) 45 (30.2) 37 (24.8) 26 (17.4) 24 (16.1)
9 (6.0)
5 (3.4)
82 (59.9) 49 (35.8) 61 (44.5) 54 (39.4) 56 (40.9) 41 (29.9) 21 (15.3) 15 (10.9) 7 (5.1) 4 (2.9)
180 (62.9) 134 (46.9) 139 (48.6) 121 (42.3) 101 (35.3) 78 (27.2) 47 (16.4) 39 (13.6)
16 (5.6)
9 (3.2) aFor purposes of this study, renal impairment was considered to exist in subjects with creatinine levels above 150 pmol per liter.
Grell 0 THE JAMAICAN HYPERTENSIVE 269
Changes associated with hypertensive re- tinopathy were present in 67.7% of those whose fundi were carefully examined (Table 5), and 14.7% were found to have accelerated (III) or malignant (IV) retinopathy.
Malignant hypertension with papilloedema was detected by fundoscopy in 10 males and eight females representing 6.3% of the popula- tion studied. In this group, headache and visual
disturbance were the most common clinical com- plaints. The majority of the 18 were recently diagnosed as being hypertensive, only 39% having a previous history of the disease; the patients also tended to be younger than the other study subjects, and 83.3% had severe renal impair- ment.
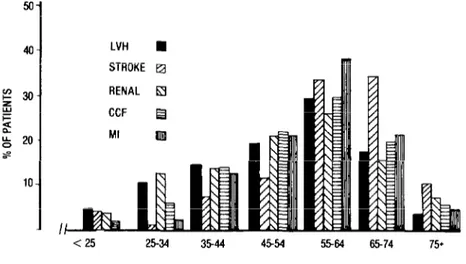
In general, the prevalence of complications was age-related (Figure 2), although renal im-
Table 5. Keith-Wagener-Barker (K-W-B) fnndoscopic changes observed
in the 286 study subjects, by sex.
K-W-B grade Males FelllabS Total NO. (%) NO. (%) NO. (%) Normal 28 (18.8) 32 (23.4) 60 (21.1)
I 22 (14.8) 2: (5.1) 29 (10.2) II 26 (17.4) (19.0) 52 (17.9) III 13 (8.7) 11 (8.0) 24 (8.4)
IV 10 (6.7) (5.8) 18 (6.3
Not coded” 50 (33.6) 5: (38.7) 103 (36.1) Total 149 (100) 137 (100) 286 (100) “In the uncoded cases the fundi were not examined, or the patient was too uncooperative for proper evaluation, or the presence of cataracts prevented proper evaluation.
Figure 2. Observed complications, by sex and ten-year age group, among the 286 study subjects. LVH = left ventricular hypertrophy, STROKE = cerebrovascular
accident, RENAL = renal impairment, CCF = cardiac failure, and MI = myocardial infarction.
50
1
40- LVH n STROKE 0
- I
pairment (as indicated by creatinine levels above 150 pm01 per liter) was relatively more common in patients between 25 and 34 years of age. Proteinuria was found to be a useful simple in- dicator of severe renal dysfunction, inasmuch as 42.8% of the patients with proteinuria had creatinine levels above 250 pmol per liter (as compared to only 6.7% of the patients without proteinuria), and there was a progressive in- crease in the prevalence of severe renal impair- ment in patients with proteinuria graded 0 to 3 + using Ames Uristixm.
Myocardial infarction was significantly (p<O.O5) more common in patients with dias- tolic blood pressures of less than 100 mmHg and was the most important single cause of death in the mild hypertensives. Impairment of renal func- tion was most common in patients with severe hypertension and was present in 45.5% of the patients with diastolic pressures of 120 mmHg and above.
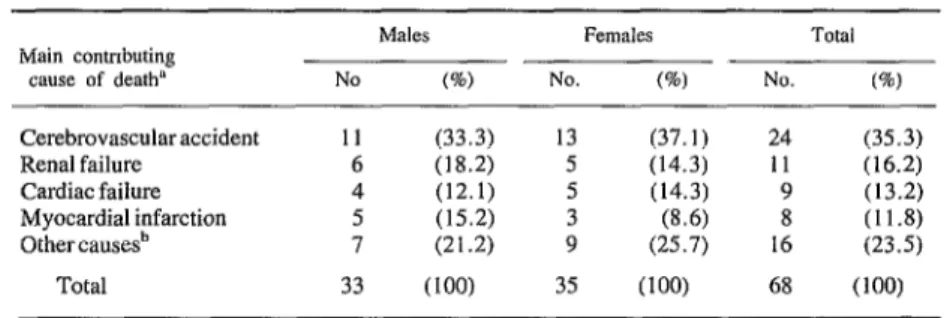
There were 68 hypertensive patients who died in the hospital during the two-year period of this study (Table 6). In contrast to the prevailing situation in Europe and North America, how- ever, myocardial infarction was less common as a terminal event than cardiac failure, renal failure, or cerebrovascular accidents.
A comparison of the prevalence of four com- mon coronary risk factors among our study sub- jects and among a sample of the general hospital
outpatient clinic population suggested a rela- tively high prevalence of cigarette smokers and patients with diabetes mellitus among the hyper- tensive study subjects (Table 7).
Discussion and Conclusions
Jamaica and the Caribbean offer an important opportunity to study black hypertensives in an environment where they occupy all levels of the existing social hierarchy.
Overall, only nine of the hypertensive patients admitted during the two-year period under re-
Table 7. The prevalence of four common risk factors (associated with coronary heart disease) in the 286 hyper- tensive study subjects as compared to the prevalence of these same risk factors in 246 patients attending a general
medical outpatient clinic at the university hospital. The latter sample was composed of outpatients seen consecutively over a three-month period at one of the
hospital’s general medical outpatient clinics.
Risk factor
% of hospitalwed hypertenswe
patExIts
(n = 286)
% of general outpatient clinic patients
(n = 246) Alcohol consumption 49.1 49.6 Cigarette smoking 45.0 11.8 Obesity= 28.2 31.7 Diabetes mellitus 36.1 15.0
‘A weight over 20% above the “ideal” body weight, as defined by the Metropolitan Life Insurance Company Table of Desirable Weight.
Table 6. The main causes of deaths of the 68 study subjects dying in the hospital in 1980-1981.
Main contnbuting cause of death=
M&S Females Total
No (%) NO. (%) NO. (90) Cerebrovascularaccident 11 (33.3) 13 (37.1) 24 (35.3) Renal failure 6 (18.2) 5 (14.3) 11 (16.2) Cardiac failure 4 (12.1) 5 (14.3) 9 (13.2) Myocardial infarction 5 (15.2) 3 (8.6) (11.8) Other cause& 7 (21.2) 9 (25.7)
1:
(23.5) Total 33 (100) 35 (100) 68 (loo) “Several complications may have been present terminally. The one listed here was the one found to be the main contributing cause of death. Postmortems were done in 26 of these 68 cases.
Grell 0 THEJAMAICANHYPERTENSIVE 271
view were under 25 years old. The clinical prob- lems associated with hypertension assumed sig- nificance mainly in persons over 34 years old (88.1% of the hypertensives were age 35 or more), with the peak prevalences occurring among males in the 55-64 year age group and among females in the 55-64 and 65-74 year age groups.
As in most countries, the majority of the study subjects seen in Jamaica had essential hyperten- sion; but it has been found that while renal dis- ease is the most common cause of secondary hypertension, renovascular disease is uncom- mon in Jamaicans (8) and also in other black populations (9).
Previously reported experience in Jamaica (IO) also indicates that low renin hype,rtension is not overrepresented, as has been reported for blacks elsewhere (II). A profile of the Jamaican hypertensive population has shown that 24% of those studied had high renin levels, 45% had normal renin levels, and 31% had low renin hypertension (IO).
While Akinkugbe (12) has commented on the relatively infrequent occurrence of hypertensive retinopathy in the African, in our study fundo- scopy was normal in only 21.1% of the hospital- ized patients, and 14.7% had grade III and IV changes. This high prevalence of hypertensive retinopathy in Jamaica is consistent with data of McDonough et al. (13) from the Evans County study that showed hypertensive blacks to have a higher prevalence of hypertensive retinal changes at each level of blood pressure than did whites. Fundoscopic grading was found to be particularly useful in indicating the prevalence and degree of underlying renal disease. Breslin et al. (14) found that ophthalmoscopic grading was positively correlated with the severity of diastolic hypertension as well as with the inci- dence of azotemia, proteinuria, inversion of the T wave on ECG, cardiomegaly on X-ray, and ten-year mortality.
Impairment of renal function was a common finding in Jamaican hypertensives, occurring in 52.3% of the males and 44.5% of the females in our study population; renal failure accounted for 16.2% of the deaths in that population.
Hypertension also contributes the largest quota of patients to the chronic hemodialysis program (6.6% of our study subjects were dialyzed). In this regard, it has been suggested that black pa- tients may have an increased susceptibility to the effects of hypertension. For instance, in one biracial analysis of patients with renal failure, it was noted that blacks seemed to develop renal failure at a lower systolic blood pressure than whites (15).
In South Africa, cardiac failure has been cited as the most common complication seen in black hypertensives (16, 17, 18). In Jamaica, cardiac failure was present in 35.3% of the admitted hypertensive patients and was the cause of death in 13.2% of those who died during the two-year study period.
Adelstein (19) has shown that the proportional mortality from ischemic heart disease was lower among people of African ancestry than among people of British or Asian ancestry. Beever’s group (20) has shown that West Indians in Bir- mingham, England, had relatively few heart at- tacks compared to whites, although they had a higher incidence of hypertension and proportion- ately more strokes.
Today, stroke (cerebrovascular accidents) and heart diseases are the most common causes of death in the islands of the West Indies (2). Stroke is the most common cause of death in hyperten- sives (see Table 5), and hypertension is now the most important single contributor to mortality in the Caribbean (21).
were present in 29.2% of Jamaican study sub- jects with systolic pressures above 160 mmHg,
while such changes were noted in only 1.6% of those with systolic pressures below 120 mmHg. Ashcroft attributed these changes to hyperten- sion per se, rather than interpreting them as im- plying the presence of coronary heart disease. The complications associated with hyperten- sion are influenced by the presence of associated risk factors such as cigarette smoking, alcohol consumption, obesity, and diabetes mellitus. In particular, these risk factors increase the preva-
lence of coronary heart disease. And, although the incidence of coronary heart disease is rela- tively low in the West Indies, there is evidence to suggest that this incidence has increased in recent years (23). Further studies are thus re- quired to determine those influences that may alter the natural history of hypertension, as man- ifested in blacks, in order to contribute to an understanding of the basic factors associated with racial differences reported from clinical and epidemiologic research.
ACKNOWLEDGMENTS
My research nurses, Marlene Anderson, Phyllis Gibbs, and Rosemarie Douglas, were meticulous in helping to collect data. Mr. Roy Bailey deserves special thanks for allowing me the use of his facilities at the University of the West Indies Computer Center.
SUMMARY
Hypertension is the most common chronic disease of adults in the Caribbean, affecting some 22% of the population. For the purpose of learning more about prevailing patterns of hypertension in black residents of the area, a prospective survey was conducted of all black hypertensives admitted to the medical wards of the University Hospital of the West Indies in Kingston, Jamaica, during 1980 and 1981.
In all, 149 males and 137 females meeting the sur- vey’s criteria for hypertension were included in the study. Of these 286 patients, 90.2% had essential hypertension, 9.1% showed evidence of underlying renal disease, 0.3% (one patient) had pheochromocy- toma, and 0.3% (one patient) hadconn’s syndrome.
The most frequent complications seen at the time of hospitalization included cardiomegaly (in 62.9% of the subjects), renal impairment (in 48.6%), cardiac failure (in 35.3%), and cerebrovascular accident (in
27.3%). Myocardial infarction was diagnosed in 16.4% of the patients. Changes associated with hyper- tensive retinopathy were present in 67.7% of the study subjects whose fundi were carefully examined, and 14.7% were found to have accelerated (III) and malig- nant (IV) retinopathy. Malignant hypertension was seen in 6.3% of the subjects.
Grell 0 THE JAMAICAN HYPERTENSIVE 273
REFERENCES
(I) Grell, G.A.C. Hypertension: A challenge for the providers of health care in the Caribbean. West Indian Med J 30:105-106, 1981.
(2) Grell, G.A.C. Epidemiology of Hypertension in the Caribbean. In: Proceedings of the Meeting and Papers of the Expert Committee on Chronic Diseases (in the English-Speaking Caribbean), Part II. Pan American Health Organization/World Health Organi- zation, Barbados, 6-7 January 1983.
(3). Antia, A. U., R. Maxwell, A. Gough, and 0. Ayeni. Arterial blood pressures in Jamaican chil- dren ofnegrodescent. WestIndianMedJ29:110-116,
1980.
(4) Ashcroft, M. T., and P. Des& Blood pressure and mortality in a rural Jamaican community. Lancet 1:1167-1170, 1978.
(5) Miall, W. E., and A. L. Cochrane. The distri- bution of arterial pressure in Wales and Jamaica. Path01 Microbial 24:690-697, 1961.
(6) Miall, W. E., E. H. Kass, J. Ling, and K. L. Stuart. Factors influencing arterial pressure in the general population in Jamaica, Br Med J 2:497-506, 1962.
(7) Veterans Administration, United States. Veter- ans Administration Cooperative Study Group on anti- hypertensive agents-effects of treatment on morbidi- ty in hypertension: I. Results in patients with diastolic blood pressure averaging 115 through 129 mmHg. JAMA 202: 116-122, 1967.
(8) Grell, G.A.C. Clinical aspects of hypertension in Jamaica. West Indian Med J 27:231-237, 1978.
(9) Keith, T. A. Renovascular hypertension in black patients. Hypertension 4438-443, 1982.
(IO) Grell, G.A.C., T. Forrester, and H. M. Robinson. Renin levels in hypertensive patients in Jamaica. West Zndian Med J 30:30-33, 1981.
(II) Sever, P. S., D. Gordon, W. S. Peart, and P. Beighton. Blood pressure and its correlates in urban and tribal Africa. Lancet 2:60-64, 1980.
(12) Akinkugbe, 0. 0. The Rarity of Severe Hypertensive Retinopathy in the African. In: 0.0.
Akinkugbe. High Blood Pressure in the African. Churchill Livingston, London, 1972, pp. 90-96.
(13) McDonough, J. R., G. E. Garrison, and C. G. Hames. Blood pressure and hypertensive disease among negroes and whites. Ann intern Med 61:208, 1964.
(14) Breslin, D. J., R. W. Gifford, J. F. Fairbairn, and T. P. Keams. Prognostic importance of ophthal- moscopic findings in essential hypertension. JAMA 195:335-338, 1966.
(15) Goss, L. Z., R.M.F. Rosa, W. M. O’Brien, C. R. Ayers, and J. E. Wood. Predicting death from renal failure in primary hypertension. Arch Intern Med 124:160-164, 1969.
(16) Seedat, Y. K., and J. Reddy. A study of 1,000 South African non-white hypertensive patients. S Afr Med J 48:X16-820, 1974.
(17) Seedat, Y. K., and N. Pillary. Myocardial infarction in the African hypertensive patient. Am Heart J 94:388-390, 1977.
(18) Seedat, Y. K. Race, environment and blood pressure: The South African experience. Jour;aZ of Hypertension 1:7-12, 1983.
(19) Adelstein, A. M. Current vital statistics: Methods and interpretation. Br Med J 2:983-987, 1978.
(20) Cruickshank, J. K., D. G. Beevers, V. L. Osboume, R. A. Haynes, J.C.R. Corlett, and S. Selby. Heart attack, stroke, diabetes, and hyperten- sion in West Indians, Asians, and whites in Birming- ham, England. Br Med J 2X1:1108, 1980.
(21) Grell, G.A.C. Hypertension in the West In- dies. Postgrad Med J 59:5-10, 1983.
(22) Ashcroft, M. T. Prevalence of hypertension and associated electrocardiographic abnormalities in Jamaica and West Africa. West Indian Med J 26:24- 33, 1977.
(23) Ashcroft, M. T., and K. L. Stuart. Acute myocardial infarction in the University Hospital, Jamaica, 1968-1970. West Zndian Med J 22:60-66,