w w w . r b o . o r g . b r
Original
Article
Muscle
injury:
current
perspectives
and
trends
in
Brazil
夽
,
夽夽
Diego
Costa
Astur
∗,
João
Vitor
Novaretti,
Renato
Kalil
Uehbe,
Gustavo
Gonc¸alves
Arliani,
Eduardo
Ramalho
Moraes,
Alberto
de
Castro
Pochini,
Benno
Ejnisman,
Moises
Cohen
PaulistaMedicalSchool,FederalUniversityofSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received3October2013 Accepted31October2013 Availableonline27October2014
Keywords:
Muscleinjury Perspectives Treatment Management Epidemiology
a
b
s
t
r
a
c
t
Objective:Toevaluatethemanagement,proceduresandperspectivesofsportsphysicians andorthopedistsinBrazilwithregardtodiagnosingandtreatingmuscleinjuries.
Methods:Aquestionnaire containing20questionsrelatingtothetopic ofmuscleinjury wasappliedtosportsphysiciansandorthopedistsduringtheSecondBrazilianCongress ofArthroscopyandSportsTraumatology,in2013.
Results:Completelyansweredquestionnaireswerereceivedfrom168sportsphysiciansand orthopedists.DoctorsfromallregionsofBrazilwithameanof11yearsofexperienceof treatingmuscleinjurieswereinterviewed.Lowerlimbswereaffectedin97%ofthecases, par-ticularlythequadriceps,adductorandsuraltriceps.Theinjuryoccurredduringtheeccentric phasein62%oftheinterviews;39%underwentultrasoundexaminationand37%magnetic resonanceimaging(MRI)fortheinjurytobediagnosed.Medication,restandcryotherapy duringtheacutephase(87.5%)andmedication,restandphysiotherapyduringtreatmentof theinjury(56%)weretheprevalentoptions.Thecriteriaforreturningtosportswerevery subjectiveanddisparateamongtheoptionspresented,andmostoftheintervieweeshad alreadyusedsometherapythatwasadjuvanttotraditionalmethods.
Conclusion: Thenumberofmuscleinjuriestreatedperyearwasgreaterthan30, indepen-dent ofwhether inthe publicor privatesector.These injuriesoccurred mainly atthe muscle–tendonjunction,inthelowerlimbsandduringtheeccentricphaseofmuscle con-traction.Ultrasoundwastheexaminationmostperformed,whileMRIwasconsideredideal. Formostoftheinterviewees,thepreferredtreatmentinvolvedrest,medicationand physio-therapy.Inaddition,52%believedthatplatelet-richplasmawasanefficienttreatmentand 42%saidthattheyhadalreadyusedit.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:AsturDC,NovarettiJV,UehbeRK,ArlianiGG,MoraesER,deCastroPochiniA,EjnismanB,CohenM.Lesão muscular:perspectivasetendênciasatuaisnoBrasil.RevBrasOrtop.2014;49:573–580.
夽夽
WorkdevelopedattheSportsTraumatologyCenter,DepartmentofOrthopedicsandTraumatology,PaulistaMedicalSchool,Federal UniversityofSãoPaulo(Unifesp),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](D.C.Astur).
http://dx.doi.org/10.1016/j.rboe.2013.10.003
Lesão
muscular:
perspectivas
e
tendências
atuais
no
Brasil
Palavras-chave:
Lesãomuscular Perspectivas Tratamento Conduta Epidemiologia
r
e
s
u
m
o
Objetivo: Avaliarascondutas,osprocedimentoseasperspectivasdomédicodoesportee ortopedistadoBrasilnodiagnósticoenotratamentodelesõesmusculares.
Métodos:Questionáriocom20questõesrelacionadasaotemalesãomusculares.Foiaplicado emmédicosdoesporteeortopedistasduranteoIICongressoBrasileirodeArtroscopiae TraumatologiadoEsporte,em2013.
Resultados: Responderamcompletamenteoquestionário168médicosdoesportee ortope-distas.ForamentrevistadosmédicosdetodasasregiõesdoBrasil,commédiade11anosde experiêncianotratamentodalesãomuscular.Membrosinferioressãoacometidosem97% doscasos,principalmentequadríceps,adutoretrícepssural.Alesãoocorrenafase excên-tricapara62%dosentrevistados,39%fazemultrassom(USG)e37%ressonânciamagnética (RM)paradiagnósticodalesão.Medicac¸ão,repousoecrioterapianafaseaguda(87,5%)e medicac¸ão,repousoefisioterapiaduranteotratamentodalesão(56%)sãoasopc¸ões preva-lentes.Oscritériosderetornoaoesporteforambastantesubjetivosedísparesentreas opc¸õesapresentadaseamaioriadosentrevistadosjáusoualgumaterapiaadjuvanteàs tradicionais.
Conclusão: Onúmerode lesõesmuscularestratadasanualmente ésuperiora 30, inde-pendentemente de se no setor público ou privado. Ocorre principalmente na junc¸ão miotendínea,nosmembrosinferioresenafaseexcêntricadacontrac¸ãomuscular.OUSG éoexamemaisfeitoeaRMoconsideradoideal.Paraamaioriadosentrevistadoso trata-mentodeescolhaenvolverepouso,medicac¸ãoefisioterapia.Alémdisso,52%acreditamna eficiênciadoplasmaricoemplaquetas(PRP)e42%referemjátê-lousado.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Overrecent decades, the number ofpeople taking part in sportsactivitiesaroundtheworldhasprogressivelyincreased. Alargepartofthisincreasehasoccurredbecauseofthe exten-sivedisseminationbythemediaofthebenefitstohealththat result from regularly practicing exercise. Exercise provides improvementofqualityoflifeandreductionofthe riskof havingmanydiseases.1–3
However, it is known that the benefits from practicing sportsstandincontrasttotheincreaseinthenumberof osteo-muscularinjuries.4Almost10millionsports-relatedinjuries
occureveryyearintheUnitedStates.5Mostofthemarenot
very severe, but theyare painfuland oftenincapacitating, sincetheytakepeopleawayfromtheirphysicaland profes-sionalactivities.6
Muscleinjuriesarethecommonestoftheseandaccountfor 10–55%ofallsportsinjuries.Theyconsistmainlyofbruises, sprains and lacerations.7 Injuries due to sprains generally
affectsuperficialandtwo-jointmuscles(rectusfemoris,knee flexorsandgastrocnemius)andtheyoccurduringthe eccen-tricphaseofcontraction.8Thecausesaremultifactorialand
there are somerisk factors,such as age, previous muscle injuriesinthesameregion,ethnicity,overloading,force imbal-anceandalterationofthecapacitytostretchthemusclegroup inquestion.9
However,littlehaschangedoverrecentdecadesregarding the way in which muscle injuries are understood and treated. Theaimof thepresent study was toevaluatethe
conceptualizations,diagnosticmethods,treatmentmethods andperspectivesofspecialistphysiciansthroughapplyinga questionnaireamongthem,onmuscleinjuriesinBrazil.From theseresults,itwillbepossibletodelimitnationaltrendson thislittlestudiedtopicandguidesubsequentnewresearchin thisfield.
Methods
Thiswasadescriptivestudywithapplicationofa question-naire toasampleformed mainlybysports physiciansand orthopedists.Thisquestionnairewascomposedof20closed questionsandwasdrawnupbythepresentauthorsinasimple andobjectivemanner.Itcoveredthemaintopicofthesubject ofmuscleinjuries(Appendix1).
Thequestionnairewasappliedtophysicianswhoroutinely treatmuscleinjurieswhowereattendingtheSecondBrazilian CongressofSportsArthroscopyandTraumatology(SBRATE), whichtookplaceinFortalezain2013.
Thus,168questionnaireswerefilledout underguidance from oneoftheresearchersforclarificationsofanydoubts thatmayhavearisen.
From the data obtained through the questionnaires that were filled out, descriptive statistics were calculated on the variables involved, in order to characterize the sample.
Table1–Geographicaldistributionofthestudy participants.
Numberof physicians
North 9(5%)
Northeast 44(27%) Center-West 18(10%) Southeast 79(47%)
South 18(10%)
Total 168
Results
Therewere168completedquestionnaires,filledoutby physi-ciansfrom20statesinallthefiveregionsofBrazil(Table1): 118wereorthopedists,43wereorthopedistsandsports physi-cians,fivewere sportsphysiciansand twowere fromother specialties.
Themeanlengthoftimeforwhichtheprofessionals inter-viewed had been activeintreating muscle injurieswas 11 years.Mostoftheintervieweesdealtwithmuscleinjuriesin bothpublicandprivateservicesandsawmorethan30cases
peryear(Table2).
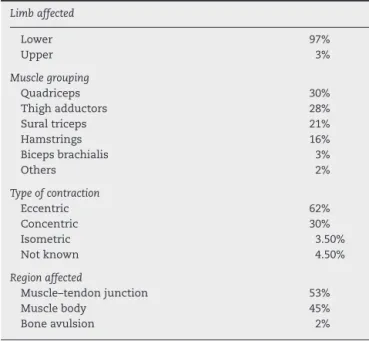
Mostoftheinjuriescitedoccurredinthelowerlimbs(97%): 30%inthequadriceps,28%inthethighadductorsand21% inthesuraltriceps.Theseinjuriesmostcommonlyoccurred duringtheeccentricphaseofmovement(incasesseenby62% oftheinterviewees)andmostlyaffectedthemuscle–tendon junction(53%)andthemusclebody(45%)(Table3).
Theexaminationmostoftenperformedbythephysicians interviewed,inordertoaidinthediagnosis,wasultrasound (39%),butthemajorityofthem(84%)consideredthat mag-neticresonanceimagingwasthebestexaminationformaking diagnoses(Table4).Throughtheimagingexamination,itwas possibletoclassifytheinjuriesusingthemethodpreferredby themajorityoftheinterviewees(73%):themethodthatdivides injuriesintothreegradesaccordingtothenumberoffibers injured.Ontheotherhand,24%oftheintervieweespreferred toclassifyinjuriesonlywithadescription ofthe anatomi-calregioninjured.Moreover,48%consideredchronicmuscle injuriestobethosethathadbeenpresentedformorethansix weeks,35%formorethanthreeweeksand15%formorethan 3months.
The treatment of choice in the acute phase of the injury for most of the interviewees was a combination of rest,cryotherapyandmedication.Regardingtheoptionsfor
Table2–Numberofmuscleinjurycasestreatedwithin thepublicandprivatesystemseveryyear.
Muscleinjurycases treated/year Public service Private service Publicand private
<10 4(27%) 9(13%) 11(15%) 10–20 5(33%) 13(19%) 10(13%) 20–30 2(13%) 10(15%) 25(33%) >30 4(27%) 35(52%) 29(39%)
Total 15 67 75
Table3–Maincharacteristicsofthemuscleinjuries:site affectedandtypeofcontractionattimeofinjury.
Limbaffected
Lower 97%
Upper 3%
Musclegrouping
Quadriceps 30% Thighadductors 28% Suraltriceps 21% Hamstrings 16% Bicepsbrachialis 3%
Others 2%
Typeofcontraction
Eccentric 62%
Concentric 30% Isometric 3.50% Notknown 4.50%
Regionaffected
Muscle–tendonjunction 53% Musclebody 45% Boneavulsion 2%
Table4–Comparisonbetweentheexaminationmost performedandtheoneconsideredidealfordiagnosing muscleinjuries.
Examination performed
Ideal examination
USG 65(39%) 23(14%) MRI 62(37%) 142(84%) USG+MRI 29(17%) 0 Notused 12(7%) 3(2%)
USG,ultrasound;MRI,magneticresonanceimaging.
medications,themajority(35%)prescribedanti-inflammatory drugs alone, followed by analgesics (25%) and an associa-tion of anti-inflammatory drugs and analgesics (12%). For mostoftheinterviews(56%),the treatmentaftertheacute phasewascomposedofmedication,restandphysiotherapy. Inthiscase,themedicationmostprescribedwasanalgesics
(Tables5and6).
Table5–Mainmedicationsusedfortreatingmuscle injuriesatthetimeoftheinjury(acute)andduringthe treatmentperiod(post-injury).
Treatment Acute Post-injury
NSAID 59(35%) 39(23%) AG 42(25%) 74(44%) NSAID+AG 20(12%) 7(4%) NSAID+AG+RX 20(12%) 6(3.5%) NSAID+RX 18(10.5%) 9(5.5%) AG+RX 5(3%) 9(5.5%) RX 3(2%) 15(9%) Other 1(0.5%) 9(5.5%)
Table6–Therapeuticoptionsfortreatingmuscleinjuriesatthetimeoftheinjuryandaftertheinjury.
Treatment Acute Treatment Post-injury
Medication+rest+cryo 147(87.5%) Medication+rest+physio 95(56%) Medication+rest 10(6%) Physio+rest 28(17%) Cryo+rest 7(4%) Physio 25(15%) Medication 0 Medication+rest 15(9%)
Cryo 0 Medication 0
Other 4(2.5%) Other 5(3%)
Cryo,cryotherapy;Physio,physiotherapy.
ForinjuriesclassifiedasgradeI,themeanlengthoftime awayfromsportsactivitieswas13days;gradeII,28days;and gradeIII,48days.Themaincriteriausedfordeterminingthe returntosportwerecomparisonofmusclestrengthalonein theinjuredlimbwiththecontralaterallimbandcombination evaluationofthepainscaleandmusclestrengthinrelationto thecontralaterallimb,alongwiththepatient’sowndegreeof confidence(Table7).
Theintervieweeswerealsoaskedaboutotherpossible ther-apiescitedintheliteraturethat couldbeusedfortreating muscleinjuries: 52%believed that treatmentwith platelet-richplasma(PRP)wasefficient,butonly42%hadalreadyused
Table7–Criteriausedforthereturntosport,for patientstreatedformuscleinjury.
Criteriaforreturntosport Number
FMcontralateral 24(14%) Pain+contralateral
MS+confidence
23(13.5%)
Pain+contralateralMS 22(13%) Alloptions 19(11%)
Pain 16(9.5%)
Otheroptions 14(8.5%) Confidence 13(7.5%) Pain+confidence 12(7%) Imagingexamination 5(3%) Pain+imagingexamination 5(3%) ContralateralMS+confidence 5(3%) Pain+contralateral
MS+imagingexamination
3(2%)
MS+imaging
examination+confidence
2(1%)
MS+imagingexamination 1(0.5%) Pain+imaging
examination+confidence
1(0.5%)
Pain+MS+circumferenceof injuredlimb
1(0.5%)
Pain+confidence+circumference ofinjuredlimb
1(0.5%)
MS+imaging
examination+circumference ofinjuredlimb
1(0.5%)
Circumferenceofinjuredlimb 0
ContralateralMSreferstocomparisonofmusclestrengthbetween theinjuredanduninjuredsides;painisevaluatedbymeansofa visualanalogscale;confidenceisasubjectivemeasurement; imag-ingexaminationrelatestofollow-upoftheevolutionoftheinjury; circumferenceoftheinjuredlimbreferstoevolutioncomprising hypotrophycausedbytheinjury.
Table8–Interviewees’opinionsregardingtheefficiency ofnewtherapiespresentedintheliterature,fortreating muscleinjuries,andwhethertheyhadhadthe
opportunitytousetherespectivetherapeuticoptions.
Therapy Efficiency Used
PRP 88(52%) 70(42%) Shockwaves 45(27%) 45(27%) Genetherapy 11(6.5%) 0 Localinfiltration 7(4%) 36(21%) Others 20(12%) 18(11%) Noopinion 24(14%) 40(24%)
PRP,platelet-richplasma.
thistherapeuticmethod,while14%didnotbelieveinanyof themethodspresentedand24%hadneverusedanyofthese therapeuticmethods(Table8).
Discussion
Muscle injury is the commonest type of musculoskeletal injury.Itmayrepresentupto50%ofallorthopediccomplaints. Inmostcases,the patientiscapableofreturningto activi-tiesatthesamelevelasbeforetheinjury,withoutfunctional deficits.10,11Nonetheless,littleisknownabouttheseinjuries.
Thereisnoconsensusonthebestwayofdefiningtheir sever-ity, the mostappropriatetreatment and the mostefficient formofrehabilitation.
Thepresentstudyevaluatedthemaintopicsinvolvedin muscleinjuriesandinvestigatedthemamongapopulationof highlyspecializedphysicianswhowereaccustomedtodealing withthispathologicalcondition.
Thesequestionswereputto168sportsphysiciansand/or orthopedistsfrom allregionsofBrazilwhosemeanlevelof experienceoftreatingmuscleinjurieswas11years.
example,inkickingmovements:quadriceps,thighadductors andsuraltriceps.
Intheliterature,muscleinjurieshavebeencorrelatedwith eccentriccontraction.12–15 62%oftheintervieweesalsotook
theviewthatthemajorityoftheinjuriesoccurredduringthis phaseofthecontraction,whichshouldserveasinformation forcorrectphysicalpreparationandinjurypreventionamong athletespracticingavarietyofphysicalactivities.
Althoughmany classificationshavebeendescribed with theaimofbetterunderstandingofthetypesofmuscleinjury, webelievethatthereisstillnoconsensusaboutthebestway ofdifferentiatingbetweenthem.16 Thedifficultyinmaking
sampleshomogenous makescomparisonbetweendifferent injuriesverycomplex.Classificationsmayrelatetoanatomy, theregioninwhichthemusclefibersareaffectedorthetime elapsedsincetheinjury,amongmanyothers.Inthepresent study,themajorityoftheparticipantschosetodefinethetype ofinjuryaccordingtothenumberoffibersinjuredandthey dividedtheseinjuriesintothreetypes:gradesI,IIandIII. How-ever,eventhoughthisclassificationdependsonanimaging examination,itisstillvery subjectiveand resultsfrom the opinionofthephysicianwhomakestheassessment.Evenso, thisistheclassificationthatbestledtheprofessionalstothe typeoftreatmentandthelengthoftimeforwhichthe ath-letewillbeawayfromhissport.Itwasseenthatthehigher thegradeofthe injurywas, the longerthe timeforwhich thestudyparticipantschosetokeeptheathletesfromtheir activitieswas.Indiscussingthetimerequiredfordefiningan injuryasacuteorchronic,therewasalsoaverywiderange ofopinions. Intheliterature,therehasbeen little scientifi-callybasedescriptionofwhatconstitutesachronicinjury.16
Inthepresentstudy,48%believedthattheseareinjuriesthat occurredmorethansixweeksago,35%morethanthreeweeks agoand15%morethanthreemonthsago.
Inrelationtothediagnosticmethod,therewas concord-ancewiththeliteratureregardingthenotionthatmagnetic resonance imaging would be the ideal examination,17
althoughthemajorityoftheinterviewees usedultrasound. Thiscanbeexplainedbythedifferenceincostsbetweenthe examinations,althoughthismaynolongerbetheruleinother countries,wherethecostsofmagneticresonanceimagingare notashighasitisinBrazil.
Thetreatment formuscle injuries iswithout doubt the mostcontroversialitem. Althoughthe sametreatment has beenusedformorethan40years,sometherapieshavebeen described andhave started tobeusedinour setting,even thoughinsomesituationstherehasbeenlittlebasisforthis intheliterature.Intheacutephase,thegreatmajorityofthe interviewees mainly used analgesicand anti-inflammatory medications,inassociationwithrestandcryotherapy.
Thesubsequenttreatment,whichinmostcasesisguided bythetypeofinjury,wascomposedofphysiotherapy,restand medication,according to56%oftheinterviewees.Thishas beentheconventionaltriooftreatmentsformuscleinjuries formanyyears.Overthistimeperiod,muchhasbeen said aboutadjuvanttherapiesthatmightacceleratemuscle heal-ing and provide an earlier return to sport. We asked the participants whetherthey consideredthat treatmentswith PRP,shockwaves,localinfiltrationandgenetherapywere effi-cient. Mostofthem believed that PRP treatment would be efficient,followedbyshockwaves,genetherapyand infiltra-tion. However,whenasked whetherthey wereusing these therapies,smallernumbersofparticipantsaffirmedthis:42% hadalreadyusedPRP,27%shockwavesand21%infiltration. Noneofthemmentionedusinggenetherapy.
For the returntosports practice,the maincriteriaused bytheparticipantswerecomparisonofmusclestrengthwith the contralateral side,comparisonof thecombined results fromthevisualanalogpainscaleandmusclestrengthwith thecontralateralsideandthepatient’sconfidence.Thegreat challengeintreatingmuscleinjuriesprobablyrelatestothe exacttimeatwhichinjuredpatientscanreturntotheirsports activities ata highperformancelevel. Today,many criteria are used to measure this capacity to return, but in most casesthesemethodsarestillsubjective,withlittlescientific evidence.
Althoughthiswaspurelyadescriptivestudy,withalow levelofevidence,ithasgreatimportanceinthatitanalyzed thewayinwhichspecialistsdealwithinjuriesthatareso com-monyetsolittlestudiedwithregardtothemainaspectsofthis pathologicalcondition.
Conclusion
Thenumber ofmuscleinjurycasestreated everyyear was greater than 30, independent of whether this was in the publicorprivatesector.Theinjuriesoccurredmainlyatthe muscle–tendonjunction, inthe lowerlimbsandduringthe eccentric phase ofmuscle contraction.Ultrasoundwas the examinationmostused,whilemagneticresonanceimaging wasconsideredtobeideal.Thepreferredtreatmentinvolved rest,medication andphysiotherapy,forthe majorityofthe interviewees.Moreover,52%ofthephysiciansbelieved that PRPwasefficientand42%saidthattheyhadusedit.
Conflicts
of
interest
Appendix
1.
Questionnaire
applied
during
a
congress,
to
ask
professionals
within
this
field
about
r
e
f
e
r
e
n
c
e
s
1. SilvaOC.Aqualidadedevidaligadaàpráticaregularde
atividadesfísicas.EFDeportes.2010:150.
2. ProgramaNacionaldePromoc¸ãodaAtividadeFísicaAgita
Brasil.Atividadefísicaesuacontribuic¸ãoparaaqualidadede
vida.RevSaúdePúbl.2002;36(2):254–6.
3. HaskellWL,LeeIM,PateRR,PowellKE,BlairSN,FranklinBA,
etal.Physicalactivityandpublichealth:updated
recommendationforadultsfromtheAmericanCollegeof
SportsMedicineandtheAmericanHeartAssociation.Off
JAmCollSportsMed.2007:1423–34.
4. MaffuliN,LongoUG,GougouliasN,CaineD,DenaroV.Sport
injuries:areviewofoutcomes.BrMedBull.2011;97:47–80.
5. NichollJP,ColemanP,WilliamsBT.Theepidemiologyof
sportsandexerciserelatedinjuryintheUnitedKingdom.
BrJSportsMed.1995;29(4):232–8.
6. GalerBS,RowbothamM,PeranderJ,DeversA,FriedmanE.
Topicaldiclofenacpatchrelievesminorsportsinjurypain:
resultsofamulticentercontrolledclinicaltrial.JPainSymp
Manage.2000;19(4):287–94.
7.JärvinenTA,JärvinenTL,KääriäinenM,AärimaaV,Vaittinen
S,KalimoH,etal.Muscleinjuries:optimizingrecovery.Best
PractResClinRheumatol.2007;21(2):317–31.
8.LindqvistKS,TimpkaT,BjurulfP.Injuriesduringleisure
physicalactivityinaSwedishmunicipality.ScandJSocMed.
1996;24(4):282–92.
9.OparDA,WilliamsMD,ShieldAJ.Hamstringstraininjuries:
factorsthatleadtoinjuryandre-injury.SportsMed.
2012;42(3):209–26.
10.FernandesTL,PedrinelliA,HernandezAJ.Lesãomuscular–
Fisiopatologia,diagnóstico,tratamentoeapresentac¸ão
clínica.RevBrasOrtop.2011;46(3):247–55.
11.JärvinenTAH,JärvinenTLN,KääriäinenM,KalimoH,Järvinen
M.Muscleinjuries.Biologyandtreatment.AmJSportsMed.
2005;33(5):745–64.
12.ChoiSJ,LimJY,NibaldiEG,PhillipsEM,FronteraWR,Fielding
RA,etal.Eccentriccontraction-inducedinjurytotypeI,IIa,
andIIa/IIxmusclefibersofelderlyadults.Age(Dordr).
13.LieberRL,FridénJ.Mechanismsofmuscleinjuryafter
eccentriccontraction.JSciMedSport.1999;2(3):
253–65.
14.PullMR,RansonC.Eccentricmuscleactions:implicationsfor
injurypreventionandrehabilitation.PhysTherSport.
2007;8(sI):88–97.
15.AllenDG.Eccentricmuscledamage:mechanismsofearly
reductionofforce.ActaPhysScand.2001;171(s1):
311–9.
16.Mueller-WohlfahrtHW,HaenselL,MithoeferK,EkstrandJ,
EnglishB,McNallyS,etal.Terminologyandclassificationof
muscleinjuriesinsport:theMunichconsensusstatement.Br
JSportsMed.2013;47(6):342–50.
17.DiasEP,MarchioriE,CoutinhoJuniorAC,DominguesRC,
DominguesRC.Avaliac¸ãoporressonânciamagnéticadas
injúriasmuscularestraumáticas.RadiolBras.