w w w . r b o . o r g . b r
Original
Article
Partial
rotator
cuff
injury
in
athletes:
bursal
or
articular?
夽
Cassiano
Diniz
Carvalho
∗,
Carina
Cohen,
Paulo
Santoro
Belangero,
Eduardo
Antônio
Figueiredo,
Gustavo
Cará
Monteiro,
Alberto
de
Castro
Pochini,
Carlos
Vicente
Andreoli,
Benno
Ejnisman
CentrodeTraumatologiadoEsporte(CETE),DepartmentofOrthopedicsandTraumatology,UniversidadeFederaldeSãoPaulo,SãoPaulo, SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24October2013 Accepted7July2014 Availableonline2July2015
Keywords:
Rotatorcuff/injuries Bursitis
Sports
Resistancetraining
a
b
s
t
r
a
c
t
Apainfulshoulderisaverycommoncomplaintamongathletes,especiallyinthecaseof thoseinsportsinvolvingthrowing.Partiallesionsoftherotatorcuffmaybeverypainfuland causesignificantfunctionallimitationtoathletes’sportspractice.Theincidenceofpartial lesionsofthecuffisvariable(13–37%).Itisdifficulttomaketheclinicalandradiological diagnosis,andthisconditionshouldbeborneinmindinthecasesofallathleteswhopresent symptomsofrotatorcuffsyndrome,includinginpatientswhoarediagnosedonlywith tendinopathy.
Objective:Toevaluatetheepidemiologicalbehaviorofpartiallesionsoftherotatorcuffin bothamateurandprofessionalathletesindifferenttypesofsports.
Methods:Weevaluated 720medicalfiles onathletesattendedattheshoulderserviceof theDisciplineofSportsMedicineattheSportsTraumatologyCenter,FederalUniversity ofSãoPaulo.Themajorityofthemweremen(65%).Amongallthepatients,83ofthem werediagnosedwithpartiallesionsoftherotatorcuff,bymeansofultrasonographyor magneticresonance,orinsomecasesusingboth.Weappliedthebinomialtesttocompare theproportionsfound.
Result:It wasobservedthatintra-articularlesionspredominated(67.6%)andthatthese occurredmorefrequentlyin athletesinsportsinvolvingthrowing(66%). Bursallesions occurredin32.4%oftheathletes,predominantlyinthosewhodidmusclebuilding(75%).
Conclusion:Intra-articularlesionsaremorefrequentthanbursal lesionsandthey occur predominantlyinathletesinsportsinvolvingthrowing,whilebursallesionsweremore prevalentinathleteswhodidmusclebuilding.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedinHospitalSãoPaulo,UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](C.D.Carvalho).
http://dx.doi.org/10.1016/j.rboe.2015.06.009
Lesão
parcial
do
manguito
rotador
no
atleta
bursal
ou
articular?
Palavras-chave:
Bainharotadora/lesões Bursite
Esportes
Treinamentoderesistência
r
e
s
u
m
o
Oombrodolorosoéumaqueixamuitocomumentreosatletas,especialmentenocaso dosarremessadores.Aslesõesparciaisdomanguitorotadorpodemsermuitodolorosas ecausarlimitac¸ãofuncionalimportantenapraticaesportivadoatleta.Aincidênciadas lesõesparciaisdomanguitoévariável(13%a37%).Odiagnósticoclínicoeradiológicoé difíciledeveserconsideradoemtodoatletaqueapresentesintomatologiadasíndromedo manguitorotador,inclusivenospacientesdiagnosticadosapenascomtendinopatia.
Objetivo: Avaliarocomportamentoepidemiológicodaslesõesparciaisdomanguitorotador nosatletastantoamadorescomoprofissionaisdediferentesmodalidadesesportivas.
Métodos: Avaliamos720prontuáriosdeatletasatendidosnoservic¸odeombrodadisciplina demedicinaesportivanoCentrodeTraumatologiadoEsportedaUniversidadeFederalde SãoPaulo,amaioria(65%)homens.Dentretodos,83pacientesforamdiagnosticadoscom lesãoparcialdomanguitorotadorpormeiodaultrassonografiaouressonânciamagnética eemalgunscasosporambas.Aplicamosotestebinomialparacompararasproporc¸ões encontradas.
Resultado: Verificou-seumpredomíniodaslesõesintra-articulares(67,6%)equeessas ocor-reramcommaiorfrequêncianosarremessadores(66%).Jácomrelac¸ãoàslesõesbursais, essasocorreramem32,4%dosatletasepredominamnosdemusculac¸ão(75%).
Conclusão:Aslesõesintra-articularessãomaisfrequentesemrelac¸õesàsbursaise predom-inamnosatletasarremessadores,enquantoqueaslesõesbursaisforammaisprevalentes nosatletasdemusculac¸ão.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Painfulshouldersareaverycommoncomplaintamong ath-letes,especiallyinthecaseofthoseinvolvedinball-throwing sports.Partialtears ofthe rotator cuffmaybeverypainful andcausesignificantfunctionallimitationinathletes’sports practice.1,2
Theclinicalandradiologicaldiagnosisofpartialtearsis dif-ficulttomake.Somestudieshavesuggestedthatpartialtears maybemorepainfulthatcompletetears,3–5althoughclinical
examinationsandthepainpresentedarepoorindicatorsof thesizeofthelesion6andalsoarenohelpindifferentiating
betweenpartialandcompletetears.7
Partialtearsoftherotatorcuffshouldbeconsideredasa diagnosisforanypatientwhohasbeenidentifiedin preoper-ativeexaminationsaspresentingtendinopathyoftherotator cuff,or forany patient withcomplete tears,sincethere is evidencethatasignificantnumberofuntreatedpartialtears evolvetolargerorcompletetears.8
Theincidenceofpartialtearsrangesfrom13%to37%.9–13
Fukuda4 reportedthatpartialtearsoccurredin13%oftheir
patients.Ofthese,18%werebursal,55%werewithinthe ten-don and 27% were inside the joint, on the tendon of the supraspinatus.
Rotator cuffinjuries inathletes have been described in severalstudiesintheliteraturerecently.4,6,7,12,14,15 However,
theathletesmoststudiedhavebeenthoseinvolvedin ball-throwing sports. The present study observed a pattern of partialtearsoftherotatorcuffbothintheseathletesandin thosepracticingmuscle-building.Wedidnotfindanystudies
intheliteratureaddressingtheseinjuriesinthelattertypeof sport.
Typically, rotator cuff injuries among athletes involved inball-throwingsportsoccur inthearticularportionofthe tendon and at the junction between the tendons of the supraspinatusandinfraspinatus.4,6,7,12,14,15
Therearebasicallytwotheoriesregardingtheetiologyof partialtears:theextrinsicandtheintrinsictheory.
Theextrinsictheory16,17 describesabrasion betweenthe
rotatorcuffandanabnormalacromion,inwhichtheimpact would result ina bursal lesion. For intra-articular lesions, anothertypeofimpacthasbeendescribed:internalimpact. Inthis,thesupraspinatusimpactsagainsttheglenoid, espe-ciallywhentheseathletesadoptathrowingpositionabove headlevel.18,19
Ontheotherhand,theintrinsictheoryisbasedoninternal degenerationofthetendon.Inhistologicalstudies,this degen-erationismoreprominentonthejointsideofthetendonof theintactsupraspinatus.20
Otherfactorshavebeendescribed,suchastrauma, repet-itivemovements,instabilityandaninsidiousstartassociated withdegenerativeage-relatedalterations.21–26
Objective
Material
and
method
Thisstudy consistedofaninitialevaluationof720medical filesfromtheshoulderoutpatientclinicforathletesofthe Dis-ciplineofSportsMedicineofUNIFESP.Outofthetotalnumber ofpatients,252(35%)werewomenand468(65%)weremen, withameanageof28.3years.Amongthesepatients,34%were competitiveathletesand66%wererecreational.
Wedivided the athletes into two groups: sports involv-ingball-throwing(volleyball,tennisandhandball)andsports relating to muscle-building, such as body-building, base-trainingandgymtraining.Therewere44athletesinthefirst groupand39inthesecond.
Theinclusion criterion was thatthe patients should be athletes who were evaluated atour serviceand diagnosed withpartialrotatorcufftears.Patientswithotherdiagnoses, thosewhodidnotpracticesportsroutinely,thosepresenting completetearsoftherotatorcuffandthosewithassociated glenohumeral pathological conditions such as arthrosis or infectionwereexcluded.
Dataweregatheredusingaformthatsoughtclinicaldata suchaspainandlengthofevolutionofthecondition,sex,type ofsportandprevioustreatment.TheprovocativetestsofNeer andHawkins–KennedyandtheJobetestwerealsoconducted aspartofthephysicalexamination.
Thediagnosis was confirmed either byultrasonography orbymagneticresonanceimaging(MRI).Insomecases,the patientunderwentbothoftheseexaminations.
Allthepatientssignedafreeandinformedconsent state-ment prior to participation in this study. The study had previously been submitted to our institution’s ethics com-mittee for researchon human beings, for assessmentand approval.
Thedatawereevaluatedandprocessedbymeansofthe binomialtestforcomparisonbetweentwoproportions.The Bioestat5.0 softwarewasused.27 Weusedthe significance
referencevalueof5%(p<0.05).
Results
Amongthe720athletesevaluated,83(11.5%)werediagnosed withpartialtearsoftherotatorcuff.Thediagnosisofrotator cuffinjurywasconfirmedbymeansofultrasonographyin74% ofthecasesandbymeansofMRIin87%ofthecases.
Thesports-relatedinjurymechanismwasoftraumatic ori-ginin35.3%oftheathletesstudiedandwasassociatedwith repetitivemovementin64.7%.
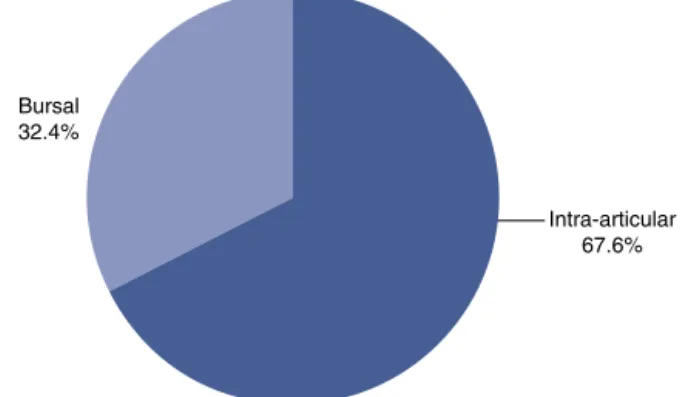
Wefoundanincidenceofintra-articularlesionsof67.6%. Ofthese,66%wereinathletesinvolvedinball-throwingsports. Ontheotherhand,theincidenceofbursallesionswas32.4% and75%oftheseoccurredinathleteswhopracticed muscle-building(Figs.1–3).
Fromapplyingthebinomialtestbetweentheproportions found,weobservedthattherewasastatisticallysignificant relationship betweenthe intra-articular and bursallesions (p=0.0001).Theintra-articular lesionswere moreprevalent thanthebursallesions.
Bursal 32.4%
Intra-articular 67.6%
Fig.1–Distributionofthepartialrotatorcufftearsamong theathletes.
Bursal
Body-builders 75%
Fig.2–Prevalenceofbursallesions.
Intra-articular
Ball-throwers 66%
Volleyball Handball Tennis Muscle-building 40
35
30
25
15 20
10
5
0
Fig.4–Distributionaccordingtotypeofsport.
Amongtheintra-articularlesions,statisticalsignificance was observed regarding the prevalence of the injuries foundamongthe athletes involved inball-throwing sports (p=0.0007).Bursallesionswereprevalentamongpractitioners ofmuscle-building(p=0.0004).
Thesportsmostfrequentlyaffectedwerevolleyball, hand-ball, tennis and muscle-building, with 18, 15, 11 and 39 athletesaffected,respectively(Fig.4).
Thirty-fourpatients(40%)weresymptomaticand refrac-tory to conservative treatment. These patients underwent arthroscopy. The other patients achieved remission of the symptomsthroughconservativetreatmentalone.
Discussion
Partialtearsoftherotatorcuffinsportshavebeengreatly stud-ied.BoththeBrazilianandtheworldwideliteraturearevastin relationtotheseinjuriesinathletesinvolvedinball-throwing sports.Nevertheless,shoulder injuriesinathletesare mul-tifactorialandpresentsomepatternsthatdifferfromthose ofthegeneralpopulation,whichneedtobenoted.Moreover, weareunawareofanystudiesaddressingthistypeofinjury amongmuscle-builders.
Weobservedinthisstudythattherewasgreaterincidence ofintra-articularlesions,oftheorderofapproximatelytwo toone,whichisin linewithcurrent literature,which sug-geststhatjointlesionsareatleasttwiceasfrequentasbursal lesions1,12,21,28–33andthatthemajorityofpartialtearsinvolve
thetendonofthesuprasupinatus.22,33,34
Thispredominanceofintra-articularlesionscanperhaps beexplainedbythebursalandintra-articularcharacteristics ofthetendon,whicharedifferent.Thebursallayeris com-posedprimarily oftendon bands with greater capacity for stretchingand,therefore,greaterresistancetotearing.Onthe otherhand,thejointfaceiscomposedonacomplexof ten-dons,capsulesandligaments.Ithasthecharacteristicofpoor distensibilityandgreaterpredispositiontotearing.14
Inthepresentstudy,40%ofthepatientsdiagnosedwith partialrotatorcufftearscontinuedtoshowsymptomsafter conservative treatment. This proportion was much higher thanwhatcanbefoundintheliterature,asrepresentedbythe systematicreviewbyReillyetal.,35inwhichitwasestimated
that 5–10% of painful shoulders presented symptomatic
partialrotatorcufftears.Weconsideredthatthisimportant differenceoccurredbecausewewereevaluatingapopulation ofathletesratherthanthegeneralpopulation.Anotherfactor mightalsohavebeenthedifferentagegroupsofthetwo stud-ies:inthemeta-analysis,theagesrangedfrom43to54years, whileinourstudythemeanagewas28.3years.
Insomesituations,theclinicalandradiologicaldiagnoses maybedifficulttomake,giventhattheclinical–radiological correlationmaybelow.Theliteraturesuggeststhatthepain maybemoresignificantinpartialtears3–5 andthatno
pat-tern ofpain canbe establishedfordifferentiatingbetween partial tears and tearing that affects the entire thickness ofthe tendon.7 The goldstandard forthe diagnosis would
reallyarthroscopyperformedduringtheoperation.However, accordingtomorerecentstudies,arthro-MRIisindicatedas thebestradiologicalexaminationforthis.36Itissuperiorto
conventionalMRIandultrasonographyandpresents sensitiv-ityof86%andspecificityof96%.However,its interobserver accuracyforclassifyingtearsbothaspartialorcompleteand inrelationtothedegreeofpartialtearingispoor,asobserved byKuhnetal.37andSpenceretal.,38respectively.
Withintheworldofsports,aseriesofassociatedfactors has meant that these injuries have acquired some par-ticular characteristics, such that diagnosing these injuries becomesmoredifficult.Insomeway,thismakesthemdiverge fromtheepidemiologicalpatternsofthegeneralpopulation. Fromthisperspective,shoulderpaininathletesinvolvedin ball-throwing sports has been correlated with a varietyof conditionsordysfunctions,suchas:subacromialimpact,17,38
anteriorglenohumeralinstability,39,40internalimpact,17,40–47
contracture of the posterior capsule,43,48,49 medial
rota-tiondeficit,43,48,49humeralretroversion,50dysfunctionofthe
trunk,scapulaandshouldermusculature51and
biomechani-caldisorders.21
Inindividualsinvolvedinball-throwingsportsandathletes whousetheirupperlimbsinpositionsaboveheadlevel,the internalimpactseemstobethemaincauseoftheirshoulder pain.52Inthestageofpreparingforthethrow,thereis
abduc-tion ofthe humerusatbetween 60◦ and 70◦, atmaximum
externalrotation.Inthisposition,arthroscopicandMRI exam-inationshaveshownthatthejointfaceoftheposteriorportion ofthetendonofthesupraspinatusandthesuperiorportion ofthetendonoftheinfraspinatushasanimpactagainstthe posterosuperior borderofthe glenoid and its labrum.7,40–47
Thissuggeststhatthereisabiomechanicalexplanationfor thepredominanceofintra-articularlesions.
Althoughthe relationshipestablishedabove isplausible andsomestudiespointinthisdirection,otherauthorssuchas Walch,41JobeandSidles46andMcFarlandetal.44havebelieved
thatthisimpactbetweentheglenoidandthetendonmightbe physiological.
Fromthisperspective,weobserveddifferentpatternsinthe twogroupsstudied(athletesinvolvedinthrowingsportsand muscle-builders).Intra-articularlesionspredominatedinthe athletesinvolvedinthrowingsports(66%)andbursallesions amongtheweight-lifters(75%).
lowervascularizationofthejointportion,greatermoduleof elasticityandconcentrationofeccentricforcesonasurface thatislessfavorabletothecurveofmaximumtension52,53
favorsjointinjuriesintherotatorcuff.Extensionofthelesion tolayersthataremoreinternaltotherotatorcuffisnotably recognizedamongathletesinvolvedinthrowingsportswith internalimpact.17,54However,weareunawareofanystudies
intheliteratureaddressingtherelationshipoftheseinjuries with individuals undertaking muscle-building in gyms, as observedinthisstudy.
Alsoinrelationtosomecharacteristicsoftheinjury,itis knownthattheinabilityofthetendontobecomecuredcanbe partiallyattributedtothepoorvascularsupplyinthetendon ofthesupraspinatus.55,56,57Ithasalsobeenobservedthatthe
vascularsupplyisgreateronthebursalsideofthetendon.55,58
Ontheotherhand,invivostudieshavedemonstratedthat there is an increase in blood flow at the borders of com-pletetears.59 Moreover,therewashypervascularizationina
smallsampleofpartialtears.60Histologicalstudieshavealso
suggestedthattheincreasesinvascularizationareinversely proportionaltothesizeofthelesion.61
Conclusion
In or study, the athletes were divided into two types: ball-throwers,encompassingvolleyball,handballandtennis players;andpractitionersofmuscle-building,who couldbe doing this as a recreational or competitive activity, within body-building or base-training. We conclude that partial bursal lesions occur more frequently among individuals practicingmuscle-building,whileintra-articularlesions pre-dominated among the athletes involved in ball-throwing sports.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. EllmanH.Diagnosisandtreatmentofincompleterotatorcuff
tears.ClinOrthopRelatRes.1990;(254):64–74.
2. Gonzalez-LomasG,KippeMA,BrownGD.Insitutranstendon
repairoutperformstearcompletionandrepairforpartial
articular-sidedsupraspinatustendontears.JShoulderElb
Surg.2008;17(5):722–8.
3. StraussEJ,SalataMJ,KercherJ,BarkerJU,McGillK,BachBRJr,
etal.Thearthroscopicmanagementofpartial-thickness
rotatorcufftears:asystematicreviewoftheliterature
arthroscopy.Arthroscopy.2011;27(4):568–80.
4. FukudaH.Partial-thicknessrotatorcufftears:amodernview
onCodman’sclassic.JShoulderElbSurg.2000;9(2):163–8.
5. GschwendN,Ivosevic-RadovanovicD,PatteD.Rotatorcuff
tearrelationshipbetweenclinicalandanatomopathological
findings.ArchOrthopTraumaSurg.1988;107(1):7–15.
6. BryantL,ShnierR,BryantC,MurrellGA.Acomparisonof
clinicalestimation,ultrasonography,magneticresonance
imaging,andarthroscopyindeterminingthesizeofrotator
cufftears.JShoulderElbSurg.2002;11(3):219–24.
7.BrownlowH,SmithC,CornerT,NeenD,PenningtonR.Pain
andstiffnessinpartial-thicknessrotatorcufftears.AmJ
Orthop.2009;38(7):338–40.
8.SmithCD,CornerT,MorganD,DrewS.Partialthickness
rotatorcufftears:whatdoweknow?ShoulderElb.
2010;2(2):77–82.
9.LöhrJF,UhthoffHK.Epidemiologyandpathophysiologyof
rotatorcufftears.Orthopade.2007;36(9):788–95.
10.DepalmaA.Surgeryoftheshoulder.Philadelphia:J.B.
Lippincott;1950.
11.FukudaH,MikasaM,YamanakaK.Incompletethickness
rotatorcufftearsdiagnosedbysubacromialbursography.Clin
OrthopRelatRes.1987;(223):51–8.
12.PayneLZ,AltchekDW,CraigEV,WarrenRF.Arthroscopic
treatmentofpartialrotatorcufftearsinyoungathletes.A
preliminaryreport.AmJSportsMed.1997;25(3):299–305.
13.UhthoffHK,SanoH.Pathologyoffailureoftherotatorcuff
tendon.OrthopClinNorthAm.1997;28(1):31–41.
14.BiglianiLU,MorrisonDS,AprilEW.Themorphologyofthe
acromionanditsrelationshiptotherotatorcufftears.Orthop
Trans.1986;10:228.
15.NeerCS2nd.Anterioracromioplastyforthechronic
impingementsyndromeintheshoulder:apreliminary
report.JBoneJointSurgAm.1972;54(1):41–50.
16.JobeCM.Superiorglenoidimpingement.OrthopClinNorth
Am.1997;28(2):137–43.
17.WalchG,BoileauP,NoelE,DonellST.Impingementofthe
deepsurfaceofthesupraspinatustendononthe
posterosuperiorglenoidrim:anarthroscopicstudy.J
ShoulderElbSurg.1992;1(5):238–45.
18.SanoH,IshiiH,TrudelG,UhthoffHK.Histologicevidenceof
degenerationattheinsertionof3rotatorcufftendons:a
comparativestudywithhumancadavericshoulders.J
ShoulderElbSurg.1999;8(6):574–9.
19.DeutschA.Arthroscopicrepairofpartial-thicknesstearsof
therotatorcuff.JShoulderElbSurg.2007;16(2):193–201.
20.GartsmanGM,MilneJC.Articularsurfacepartial-thickness
rotatorcufftears.JShoulderElbSurg.1995;4(6):409–15.
21.AndrewsJR,BroussardTS,CarsonWG.Arthroscopyofthe
shoulderinthemanagementofpartialtearsoftherotator
cuff:apreliminaryreport.Arthroscopy.1985;1(2):117–22.
22.JobeFW,KvitneRS,GiangarraCE.Shoulderpaininthe
overhandorthrowingathlete.Therelationshipofanterior
instabilityandrotatorcuffimpingement.OrthopRev.
1989;18(9):963–75.
23.JobeFW,PinkM.Classificationandtreatmentofshoulder
dysfunctionintheoverheadathlete.JOrthopSportsPhys
Ther.1993;18(2):427–32.
24.LyonsTR,SavoieFH3rd,FieldLD.Arthroscopicrepairof
partial-thicknesstearsoftherotatorcuff.Arthroscopy.
2001;17(2):219–23.
25.OzakiJ,FujimotoS,NakagawaY,MasuharaK,TamaiS.Tears
oftherotatorcuffoftheshoulderassociatedwith
pathologicalchangesintheacromion.Astudyincadavera.J
BoneJointSurgAm.1988;70(8):1224–30.
26.CordascoFA,BackerM,CraigEV,KleinD,WarrenRF.The
partial-thicknessrotatorcufftear:isacromioplastywithout
repairsufficient?AmJSportsMed.2002;30(2):257–60.
27.AyresM,AyresMJr,AyresDL,SantosAS.Bioestat5.0.
Aplicac¸õesestatísticasnasáreasdasciênciasbiológicase
médicas.Belém,Brasília:SociedadeCivildeMamiraúa/CNPq;
2007.
28.GartsmanGM.Arthroscopictreatmentofrotatorcuffdisease.
JShoulderElbSurg.1995;4(3):228–41.
29.ItoiE,TabataS.Incompleterotatorcufftears.Resultsof
operativetreatment.ClinOrthopRelatRes.1992;(284):128–35.
30.OlsewskiJM,DepewAD.Arthroscopicsubacromial
decompressionandrotatorcuffdebridementforstageIIand
31.WeberSC.Arthroscopicdebridementandacromioplasty
versusmini-openrepairinthetreatmentofsignificant
partial-thicknessrotatorcufftears.Arthroscopy.
1999;15(2):126–31.
32.McConvilleOR,IannottiJP.Partial-thicknesstearsofthe
rotatorcuff:evaluationandmanagement.JAmAcadOrthop
Surg.1999;7(1):32–43.
33.FukudaH,HamadaK,YamanakaK.Pathologyand
pathogenesisofbursal-siderotatorcufftearsviewedfrom
en-blochistologicsections.ClinOrthop.1990;(254):75–80.
34.ReillyP,MacleodI,MacfarlaneR,WindleyJ,EmeryRJ.Dead
menandradiologistsdon’tlie:areviewofcadavericand
radiologicalstudiesofrotatorcufftearprevalence.AnnRColl
SurgEngl.2006;88(2):116–21.
35.DeJesusJO,ParkerL,FrangosAJ,NazarianLN.Accuracyof
MRI,MRarthrography,andultrasoundinthediagnosisof
rotatorcufftears:ameta-analysis.AmJRoentgenol.
2009;192(6):1701–7.
36.KuhnJE,DunnWR,MaB,WrightRW,JonesG,SpencerEE,
etal.Interobserveragreementintheclassificationofrotator
cufftears.AmJSportsMed.2007;35(3):437–41.
37.SpencerEJr,DunnW,WrightR,WolfBR,SpindlerKP,McCarty
E,etal.Interobserveragreementintheclassificationof
rotatorcufftearsusingmagneticresonanceimaging.AmJ
SportsMed.2008;36:99–103.
38.NeerCS2nd.Impingementlesions.ClinOrthop.
1983;173:70–7.
39.MontgomeryWH3rd,JobeFW.Functionaloutcomesin
athletesaftermodifiedanteriorcapsulolabralreconstruction.
AmJSportsMed.1994;22(3):352–8.
40.DavidsonPA,ElAttracheNS,JobeCM.Rotatorcuffand
posterior–superiorglenoidlabruminjuryassociatedwith
increasedglenohumeralmotion:anewsiteofimpingement.J
ShoulderElbSurg.1995;4(5):384–90.
41.WalchG.Posterosuperiorglenoidimpingement.In:Rotator
cuffdisorders;1996.p.193–8.
42.JobeCM.Currentconcepts:superiorglenoidimpingement.
ClinOrthopRelatRes.1996;(330):98–107.
43.BarberFA,MorganCD,BurkhartSS,JobeCM.Labrumbíceps
cuffdysfunctioninthethrowingathlete.Arthroscopy.
1999;15(8):852–7.
44.McFarlandEG,HsuYC,NeiraC.Internalimpingementofthe
shoulder:aclinicalandarthroscopicanalysis.JShoulderElb
Surg.1999;8(5):458–60.
45.JobeFW,TiboneJE,PerryJ,MoynesD.AEMGanalysisofthe
shoulderinthrowingandpitching:asecondreport.AmJ
SportsMed.1983;11(1):3–5.
46.JobeCM,SidlesM.Evidenceforasuperiorglenoid
impingementupontherotatorcuff.JShoulderElbSurg.
1993;2Suppl.:S19.
47.JobeCM.Posteriorsuperiorglenoidimpingement.JShoulder
ElbSurg.1995;11(5):530–6.
48.BurkhartSS,MorganCD.Thepeel-backmechanism:itsrole
inproducingandextendingposteriortypeIISLAPlesionsand
itseffectonSLAPrepairrehabilitation.Arthroscopy.
1998;14(6):637–40.
49.MorganCD.SLAPlesionsinthrowingathletes.In:Presented
attheAmericanAcademyofOrthopaedicSurgeonsmeeting.
2000,February.
50.WalchG,LevigneC.Treatmentofdeepsurface
partial-thicknesstearsofthesupraspinatousinpatients
under30yearsofage.In:Thecuff.Paris,France:Elsevier;
1997.p.243–4.
51.KiblerBW.Currentconcepts:theroleofthescapularin
athleticshoulderfunction.AmJSportsMed.
1998;26(2):325–37.
52.TiboneJE,ElrodB,JobeFW,KerlanRK,CarterVS,ShieldsCLJr,
etal.Surgicaltreatmentoftearsoftherotatorcuffin
athletes.JBoneJointSurgAm.1986;68(6):887–91.
53.RoyeR,GranaWA,YatesCK.Arthroscopicsubacromial
decompression:two-to-seven-yearfollow-up.Arthroscopy.
1995;11(3):301–6.
54.ConwayJE.Arthroscopicrepairofpartial-thicknessrotator
cufftearsandSLAPlesionsinprofessionalbaseballplayers.
OrthopClinNorthAm.2001;32(3):443–56.
55.LohrJF,UhthoffHK.Themicrovascularpatternofthe
supraspinatustendon.ClinOrthopRelatRes.1990;(254):
35–8.
56.RathbunJB,MacnabI.Themicrovascularpatternofthe
rotatorcuff.JBoneJointSurgBr.1970;52(3):
540–53.
57.RothmanRH,ParkeWW.Thevascularanatomyoftherotator
cuff.ClinOrthopRelatRes.1965;41:176–86.
58.CodmanEA,AkersonIB.Thepathologyassociatedwith
ruptureofthesupraspinatustendon.AnnSurg.
1931;93(1):348–59.
59.LevyO,RelwaniJ,ZamanT,EvenT,VenkateswaranB,
CopelandS.Measurementofbloodflowintherotatorcuff
usinglaserDopplerflowmetry.JBoneJointSurgBr.
2008;90(7):893–8.
60.SwinontkowskiM,IannottiJP,HermannH,EsterhaiJ.
Intraoperativeassessmentofrotatorcuffvascularityusing
laserdopplerflowmetry.In:PostM,MorreyBF,HawkinsRJ,
editors.Surgeryoftheshoulder.StLouis,MO:Mosby-Year
Book;1990.p.202–12.
61.MatthewsTJ,HandGC,ReesJL,AthanasouNA,CarrAJ.
Pathologyofthetornrotatorcufftendon.Reductionin
potentialforrepairastearsizeincreases.JBoneJointSurgBr.