w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Prevalence
of
fibromyalgia
in
patients
treated
at
the
bariatric
surgery
outpatient
clinic
of
Hospital
de
Clínicas
do
Paraná
-
Curitiba
Deborah
Negrão
Gonc¸alo
Dias
a,∗,
Márcia
Alessandra
Arantes
Marques
a,
Solange
C.
Bettini
b,
Eduardo
dos
Santos
Paiva
a,c,daUniversidadeFederaldoParaná(UFPR),HospitaldeClínicas,Servic¸odeReumatologia,Curitiba,PR,Brazil
bUniversidadeFederaldoParaná(UFPR),HospitaldeClínicas,UnidadedeCirurgiaBariátrica,Curitiba,PR,Brazil
cUniversidadeFederaldoParaná(UFPR),DisciplinadeReumatologia,Curitiba,PR,Brazil
dUniversidadeFederaldoParaná(UFPR),HospitaldeClínicas,DepartamentodeClínicaMédica,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received9June2016 Accepted5January2017 Availableonline22March2017
Keywords: Fibromyalgia Obesity Depression
a
b
s
t
r
a
c
t
Introduction:Fibromyalgia(FM)isachronicpainsyndromecharacterizedbygeneralizedpain. Itisknownthatobesepatientshavemoreskeletalmusclepainandphysicaldysfunction thannormalweightpatients.Therefore,itisimportantthattheearlydiagnosisofFMbe attainedinobesepatients.
Objective:TodeterminetheprevalenceofFMinagroupofobesepatientswithindicationof bariatricsurgery.
Materialsandmethods: ThepatientswererecruitedfromtheBariatricSurgeryoutpatient clinicofHospitaldeClínicasofUFPR(HC-UFPR)beforebeingsubmittedtosurgery.Patient assessmentconsistedinverifyingthepresenceorabsenceofFMusingthe1990and2011 ACRcriteria,aswellasthepresenceofcomorbidities.
Results:98patientswereevaluated,ofwhich84werefemales.Themeanagewas42.07years andtheBMIwas45.39.TheprevalenceofFMwas34%(n=29)accordingtothe1990criteria and45%(n=38)accordingtothe2011criteria.Therewasnodifferenceinage,BMI,Epworth scoreandprevalenceofotherdiseasesamongpatientswhometornotthe1990criteria.Only depressionwasmorecommoninpatientswithFM.(24.14%vs.5.45%).Thesamefindings wereseeninpatientsthatmetthe2011criteria.
Conclusions: TheprevalenceofFMinpatientswithmorbidobesityisextremelyhigh. How-ever,BMIdoesnotdifferinpatientswithorwithoutFM.Thepresenceofdepressionmaybe ariskfactorforthedevelopmentofFMinthesepatients.
©2017PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](D.N.Dias). http://dx.doi.org/10.1016/j.rbre.2017.02.005
Prevalência
de
fibromialgia
em
pacientes
acompanhados
no
ambulatório
de
cirurgia
bariátrica
do
Hospital
de
Clínicas
do
Paraná
-
Curitiba
Palavras-chave: Fibromialgia Obesidade Depressão
r
e
s
u
m
o
Introduc¸ão: Fibromialgia(FM)éumasíndromededorcrônicacaracterizadapordor gener-alizada.Sabe-sequepacientesobesostêmmaisdormúsculoesqueléticaedisfunc¸ãofísica doquepacientesdepesonormal.Portanto,éimportantequeodiagnósticoprecocedaFM sejafeitoempacientesobesos.
Objetivo: DeterminaraprevalênciadeFMemumgrupodepacientesobesoscomindicac¸ão decirurgiabariátrica.
Materiaisemétodos: OspacientesforamcaptadosdoambulatóriodeCirurgiaBariátricado HospitaldeClínicasdaUFPR(HC-UFPR),antesdeseremsubmetidosàcirurgia.Aavaliac¸ão dospacientesconsistiaemconstatarapresenc¸aouausênciadeFMGpeloscritériosACR 1990e2011etambémapresenc¸adecomorbidades.
Resultados: Foramavaliados98pacientes,84mulheres.Aidademédiafoide42,07anoseo IMCde45,39.AprevalênciadeFMfoide34%(n=29)peloscritériosde1990ede45%(n=38) pelosde2011.Nãohouvediferenc¸aemidade,IMC,escaladeEpwortheprevalênciadeoutras doenc¸asentrepacientesquepreenchiamounãooscritériosde1990.Apenasdepressãofoi maiscomumnaspacientescomFM(24,14%vs.5,45%).Osmesmosachadosforamvistos naspacientesquepreenchiamoscritériosde2011.
Conclusões:AprevalênciadeFMempacientescomobesidademórbidaéextremamentealta. PorémoIMCnãodiferenospacientescomousemFM.Apresenc¸adedepressãopodeser umfatorderiscoparaodesenvolvimentodeFMnessespacientes.
©2017PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Fibromyalgia(FM)isachronicpainsyndromecharacterized
by widespread pain, muscle pain at palpation, and other
associatedsymptoms,suchasfatigue,morningstiffness, non-restorativesleepandcognitivesymptoms.1
In 1990, the American College of Rheumatology (ACR)
developedFMclassificationcriteriabasedonthepresenceof widespreadpain,pluspainuponpalpationinatleast11of18 predefinedpoints(tenderpoints).Widespreadpainisdefined asaxialpain,paininbothsidesofthebody,aswellasinthe upperandlowersegments.In2010,theACRdeveloped prelim-inarydiagnosticcriteriaforFM.Inthisnewsetofcriteria,the WidespreadPainIndex(WPI)scoreisused,plusthe Symp-tomSeverityScore (SSS).Patients withWPI≥7and SSS≥5 orWPIof3–6and SSS≥9are diagnosedwithfibromyalgia. Inthisnewcriterion thescoreoftenderpoints isnot con-sidered,andtheyweremodifiedin2011foramorepractical use.2,3
Itisknownthatobesepatientshavemoreskeletalmuscle painandphysicaldysfunctionthannormalweightpatients and thatobesity isassociatedwithcertain rheumatic
con-ditions, such as knee osteoarthritis (OA), carpal tunnel
syndromeandlowbackpain.4
There are possible mechanisms by which fibromyalgia
andobesity interrelate.PatientswithFMare overweightor
obese in most studies, and these conditions can worsen
the painful clinical picture. This may be due to several
factors,including obstructive sleep apneasyndrome, other sleepdisorders,depression,thyroiddysfunctionandcytokine profile.5
Additionally, thereisastudy withpatientssubmittedto bariatric surgery, who,afterweightlossshowed significant improvementorevenresolutionofFM.6
Knowingthatthereisanassociationbetweenthese con-ditions,itisimportanttoattainanearlydiagnosisofFMin obesepatients,toachieveanadequatetreatmentandquality oflifeimprovementofthesepatients.Thisstudyaimsto ver-ifythepresenceoffibromyalgiainapopulationtreatedina bariatricsurgeryoutpatientclinic,beforethesurgical proce-dure.TheprevalenceofFMwasverifiedthroughtheuseofthe 1990criteriaandthe2010criteriamodifiedbyWolfe.
Materials
and
methods
Studydesign
Cross-sectional study on the prevalence offibromyalgia in obesepatientswithindicationforbariatricsurgery.
Patients
Thepatientswererecruitedfrom theBariatricSurgery out-patient clinic of Hospital de Clínicas of UFPR (HC-UFPR).
One hundred patients were evaluated from 03/19/2012 to
12/09/2013andallprovidedthewritteninformedconsentform (ICF).
Patients were evaluated regarding age, gender, weight, height,BMI,andpresenceofcomorbiditiesthroughmedical recordanalysis.Theevaluationofcomorbiditieswasalso car-riedoutthroughaquestionnaireandbydirectlyaskingthe patientwhatotherdiseaseswerepresentandwhat medica-tionswereused.
FMdiagnosis
Patient evaluation consisted in verifying the presence or absenceofFMaccordingtoboththe1990andthemodified 2010ACRcriteria.Patientswereaskedaboutthepresenceof widespreadpainandinaffirmativecases,howlongthepain hadbeenpresent.Allpatientswereevaluatedforthepresence oftenderpoints.Iftherewere11ormorethan18positive ten-derpoints,thepatientwasclassifiedwithFMaccordingtothe 1990criteria.
WealsoevaluatedtheWidespreadPainIndex(WPI),which canrangefrom0to19dependingonthenumberofpainful areas,aswell as the SymptomSeverity Score (SSS),which evaluatesfatigue, repairing sleep and cognitive symptoms. Foreachoftheseitemsthedegreeofseveritycanvaryfrom 0to 3, where 0=it is nota problem; 1=slight, occasional; 2=moderate, present almost always; 3=severe, persistent,
major problems. Somatic symptoms were also evaluated,
but inasimplified way. Thepatientwas questionedabout
headaches, abdominal pain and depression, which were
scored from 0 to 3, with 0=none of the three problems;
1=onesymptom;2=twosymptomsand3=threesymptoms. ThefinalSSSrangesfrom0to12.ThesumoftheWidespread PainIndex(WPI)withtheSymptomSeverityScore(SSS) gen-eratesanewindextoevaluateFM, calledfibromyalgianess scale,whichwouldbethediseaseintensitydimension.
ByusingtheWPItogetherwiththeSSS,onehastheitems usedtoevaluatethediagnosis ofFMthroughthe2010ACR criteria.PatientsarediagnosedwithFMwhentheWPIis≥7 associatedwithSSS≥5.Whenpainisnotthemostaffected domaininthesyndrome,thediagnosisisalsopossible,since thenumberofgeneralsymptomsisgreater,thatis,withaWPI of3–6associatedwithSSS≥9thepatientisalsodiagnosed withFM.Inadditiontothescores,inordertocompletethe diagnosticcriteria,thepatientmusthavehadthecondition forthelastthreemonthsand nootherclinicalpicturethat justifiesthewidespreadpain.
TheFM-specificquestionnaire,FibromyalgiaImpact Ques-tionnaire(FIQ),whichhasbeenvalidatedforPortuguese,was alsoappliedtoallpatients.7,8Thisitemanalyzesthefrequency atwhichpatientscanperformcertaintasks,howmanydays theyfelt wellinthepreviousweek,work absenteeismand, usingscalesrangingfrom 0to10,assessespain, tiredness, depression,non-repairingsleep,amongothers.TheFIQranges
from 0to 100 and the higher the number, the greater the
impactoffibromyalgia.
Sleepevaluation
InadditiontothecriteriaforFM,weevaluatedtheEpworth scaleasasubstituteforsleepassessment.Thepatientanswers aboutthechanceofnappingwhileperformingcertaintasks accordingto ascale of0–3,0=would neverdoze, 1=slight
chance of dozing, 2=moderate chance of dozing, 3=high chanceofdozing.Incaseswherethepatientreaches10points or more,thechanceofhavingsleep disordersand/or sleep apneaisgreater.Thespecificdiagnosisofsleepdisordersin patientswithascore≥10pointsgoesbeyondtheobjectiveof thisstudy.
Statisticalanalysis
ThestatisticalanalysiswascarriedoutusingthesoftwareJMP 7.0(SAS,USA).Forcomparisonofmeans,thestudent’sttest
wasusedforparametric dataand Wilcoxon–Mannfor
non-parametricdata.Forthecorrelations,Pearson’stestwasused forparametricdataandSpearman’stestfornon-parametric data.Thechi-squaretestwasusedforproportions.
Results
One hundred patients were consecutively assessed and
completed the questionnaires; however, twopatients were
excluded, as it was not possible to review their medical
records.Thefinalanalysisconsistedof98patients,84(85.7%)
womenand14(14.3%)men.
As forthe initialassessedcharacteristics, BMIand age, there was no statistical difference betweenobese patients
withandwithoutfibromyalgia.Themeanageofwomenwas
42.07yearsandthemeanBMIwas45.39.
Whenanalyzingthesubgroupofwomen(n=84)usingthe 1990criteria,29patientshadFM(34%CI25–45),while accord-ing tothe2010criteria, 38patientshad FM(45%CI35–55); 26patientshadFMbybothcriteria(26.2%).
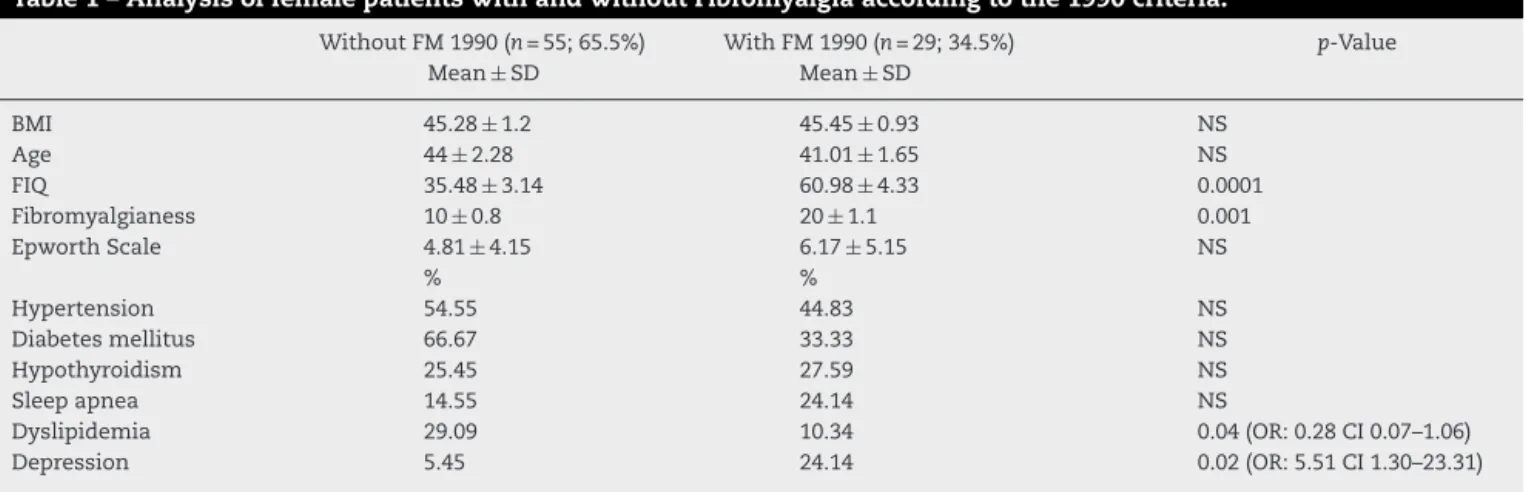
Ofthe 29 patientswho met the 1990criteria, onlynine (31.03%)hadadiagnosispriortothisstudy.Therewasno dif-ferenceinage,BMI,Epworthscore,andprevalenceofother diseasesinpatientsthatmetthe1990criteria.Only depres-sionwasmorecommoninpatientswithFM(24.14%vs.5.45%) (Table1).SignificantlyhighervaluesoftheFIQand
fibromyl-gianess index were observed in female patients with FM
incomparisontothosewithnoFM,confirmingthe useful-nessofthesemethodsintheevaluationofpatientswithFM (35.48±3.14 vs. 60.98±4.33 forFIQand 10±0.8vs. 20±1.1 forfibromyalgianessinpatientswithoutandwithFM, respec-tively).
Thesamefindingswereseeninpatientswhometthe2011 criteria(Table2).RegardingthediagnosisofFMbythe2011 criteria,only13.16%ofthepatientshadbeenpreviously diag-nosed.
Table3showsthecorrelationanalysisseparately, depend-ing on the criterion used for diagnosis. In the group that metthe1990criteria,BMIdidnotcorrelatewithFM-related indexes,suchasthenumber oftenderpoints, theFIQ,and thefibromyalgianessindex.Whentheageofthepatientswith FMwasanalyzed,therewasapositivecorrelationwiththe WPI(r=0.30,p=0.05)andthefibromyalgianessindex(r=0.35, p=0.03). These correlations were similar regardless of the criteriausedforFMdiagnosis.
Table1–AnalysisoffemalepatientswithandwithoutFibromyalgiaaccordingtothe1990criteria.
WithoutFM1990(n=55;65.5%) WithFM1990(n=29;34.5%) p-Value
Mean±SD Mean±SD
BMI 45.28±1.2 45.45±0.93 NS
Age 44±2.28 41.01±1.65 NS
FIQ 35.48±3.14 60.98±4.33 0.0001
Fibromyalgianess 10±0.8 20±1.1 0.001
EpworthScale 4.81±4.15 6.17±5.15 NS
% %
Hypertension 54.55 44.83 NS
Diabetesmellitus 66.67 33.33 NS
Hypothyroidism 25.45 27.59 NS
Sleepapnea 14.55 24.14 NS
Dyslipidemia 29.09 10.34 0.04(OR:0.28CI0.07–1.06)
Depression 5.45 24.14 0.02(OR:5.51CI1.30–23.31)
BMI,bodymassindex(kg/m2);FIQ,FibromyalgiaImpactQuestionnaire;SD,standarddeviation.
Table2–Analysisoffemalepatientswithandwithoutfibromyalgiaaccordingtothe2011criteria.
WithoutFM2011(n=46.55%) WithFM2011(n=38.45%) p-Value
Mean±SD Mean±SD
BMI 40.76±12.16 43.65±12.44 NS
Age 44.27±7.1 46.75±6.5 NS
FIQ 26.31±17.06 66.05±16.53 <0.0001
Fibromyalgianess 8.5±4.9 20.02±4.65 <0.0001
% %
Hypertension 54.35 55.26 NS
Diabetesmellitus 32.61 39.47 NS
Hypothyroidism 28.26 23.68 NS
Sleepapnea 13.04 23.68 NS
Dyslipidemia 30.43 13.16 0.05(OR:0.34IC:0.11–1.07)
Depression 6.52 18.42 0.09(OR:3.32IC:0.77–13.51)
BMI,bodymassindex(kg/m2);FIQ,FibromyalgiaImpactQuestionnaire;SD,standarddeviation.
Table3–Analysisofcorrelationsbetweenstudyvariables,onlyinfemalepatients.
BMI Age FIQ Fibromyalgianess WPI
Tenderpoints 1990 § § § § 0.31(p=0.08)
2011 § § § 0.37(p0.013) 0.48(p=0.001)
WPI 1990 § 0.37(p0.04) § § na
2011 § 0.3(p0.04) § § na
SSS 1990 § Na 0.78(p<0.0001) na na
2011 § Na 0.6(p<0.001) na na
Fibromyalgianess 1990 § 0.33(p0.06) 0.59(p0.004) – na 2011 § 0.36(p0.0017) 0.33(p0.03) – na
FIQ 1990 § § – – na
2011 § § – – na
Apnea 1990a § § 0.36(p0.08) na na
2011b § § § na na
BMI,bodymassindex(kg/m2);FIQ,FibromyalgiaImpactQuestionnaire;p,pvalue;§,nocorrelation;na,notassessed. a Only24patientsassessed.
b Only36patientsassessed.
criteria.Accordingtothe1990criteria,thesecorrelationswere stronger.WefoundanassociationbetweenFIQandEpworth indexonlyinpatientswhometthe1990criteria.
Thefibromyalgianessindexalsoshowedacorrelationwith thetenderpoints,butonlyinthepatientswhometthe2011 criteria.Thetenderpoints,inturn,showedacorrelationwith theWPIinbothcriteria.
Table4–Analysisofcorrelationsbetweenstudyvariablesinpatientswhometbothcriteria(1990and2011).
BMI Age FIQ Fibromyalgianess WPI
Tenderpoints § § § 0.37(p=0.059) 0.48(p=0.014)
WPI § 0.38(p=0.05) § na –
SSS § § 0.65(p=0.0003) na §
Fibromyalgianess § 0.41(p=0.04) 0.39(p=0.05) – na
FIQ § § – 0.39(p=0.045) §
Apnea § § § § §
BMI,bodymassindex(kg/m2);FIQ,FibromyalgiaImpactQuestionnaire;p,pvalue;§,nocorrelation;na,notassessed.
Ofthe14meninthisstudy,sevenhadFM(50%),threeof themaccordingtothe1990criteriaandfourbythe2011 crite-ria.Thecharacteristicsbetweenmenandwomendidnotvary inthisstudyregardlessofthecriteriausedfordiagnosis.
Discussion
TheprevalenceofFMinBrazilisestimatedat2.5%.9Itismore
commoninwomen,affectingapproximately3.4%ofwomen
and0.5%ofmen.10
Thereisaclearassociationbetweenfibromyalgiaand obe-sity, but the mechanisms ofsuch association are not well established yet. One cannot affirm whether obesity is the causeortheconsequenceoffibromyalgia,orifthetwo
dis-easeshavesimilarpathophysiologicalmechanisms. Among
the mechanisms proposed to explain this association are
impaired physical activity, cognitive and sleep disorders, depressionandotherpsychiatriccomorbidities,thyroidand neuroendocrineaxisdysfunctionandendogenousopioid sys-temdisorder.5
Inthepopulationwithfibromyalgia,theprevalenceof
obe-sity and overweight is approximately 32–50% and 21–35%
respectively.5,11–13Incontrast,inapopulationofobese individ-uals,theprevalenceofFMisnotaswelldocumented,ranging from5.15%to27.7%.6,14WefoundaprevalenceofFMbetween 34and45%,dependingonthecriteriaused,thus,wellabove whathasbeenreportedintheliterature.14
WefoundnoassociationbetweenFMandBMI,regardless ofthecriteriaused.However,duetotheassociationbetween FMandobesity,weexpectedpatientswithFMtohaveahigher BMI,whichwasnotconfirmedinthisstudy.Thesedataare compatiblewiththosebyArreghinietal.,2014,whichtothe
best of our knowledgeis the onlypublished study with a
similarstudydesignandthattestedthishypothesis.However, inthereportbyCorderoetal.,2014,whichevaluatedobesity inpatientswithFM, therewas aweakcorrelation between BMIand tenderpoints. Additionally, studies that assessed FMbeforeandafterweightloss showthatweightloss has animpactonpainindexes.Therefore,thefactthatwefound
noassociation between weightand FMmay bedue tothe
studydesign,aswestarted withagroupofobesepatients, notpatientswithFM.
Regardingthecomorbidities,wefoundahigherprevalence ofdepressionamongpatientswithFM,again,regardlessofthe criteriausedforevaluation.Theassociationbetween depres-sionandFMiswelldocumented.9,15 MostFMpatientsalso havedepression,withacumulativelifetimeprevalence
ran-ging from 62%to86% ofpatients.Someofthe hypotheses
explaining this strong association include depression as a reactiontochronicpainanddysfunctionorbothbeingpart ofthesamespectrumwithinaffectivedisorderswithcentral (CNS)andperipheralnervoussystem(PNS)disorders. Depres-sionlowersthepainthresholdandworsensphysicalinactivity, worseningfunctionallimitationandimpairingqualityoflife. Therefore,whendepressionisassociatedwithFM,theirjoint treatmentisimportant,sometimeswithpsychiatriccare.16
There was adifference between the FIQand
fibromyal-gianessindexes,withhighervaluesamongFMpatientsthan thosewithoutFM,usingbothcriteria.Thisconfirmsthe neg-ativeimpactthediseasehasonpatients’ dailylives,witha decreasedpain thresholdandgreater functionallimitation. Thisdrawsattention tothecomplexityofthetreatmentof patientswithFMandobesity.Ifontheonehandweightloss
can contributemuch topain control,FM causes theobese
patienttohavemoredepression,less motivationand resis-tancetophysicalactivity.Thus,obesitymanagementbecomes adifferentchallengethanthatinobesepatientswithoutFM. Forthesecases,themultidisciplinaryapproachwithpatient educationshouldincludediscussionsregardingthe associa-tionbetweenobesityandfibromyalgia.
wecannotexplainthefactthatthisassociationisonlypresent inpatientsthatmeetthe2011criteria.Initially,itmayseem strangetohavefoundthisassociationbetweentenderpoints andfibromyalgianessandWPIalsoinpatientsmeetingthe 2011criteria,asthesearenotpartofthiscriterion.However, itshouldbenotedthatallpatientswereevaluatedaccording tobothcriteria,sopatientswhoonlyhadthediagnosisbythe 2011criteriahadtheassessmentoftenderpointsavailable, makingtheanalysispossible.
TheincidenceofmenwithFMfoundinthisstudyiswell above that reported inthe literature. Wolfeet al.reported
0.5%ofaffected men, whereas in oursample wehad 50%
ofmenwithfibromyalgia.Moreover,clinicalexperiencealso reinforcesthattheincidenceofFMisnotashighinmen.This
ispossiblyduetothesmall number ofmeninthe sample
(n=14).
Thisstudyaimedtofindtheprevalenceofpatientswith FMinapublicbariatricsurgeryoutpatientclinic.Most stud-iesontheassociationbetweenfibromyalgiaandobesityhave been carriedout ingroups ofpatientswith FMand notin obesepatients,asinthepresentstudy.Studiesstartingwith obesepatientsarescarceintheliterature,6,14butourfindings showedahigherprevalencethanthepreviouslyreportedone. Thisstudyhassomelimitations.Thesamplenumberisnot largeenoughtoallowgeneralizations.Astherearefewstudies withthesamedesign,itisstillnotpossibletoevaluatethe meaningofallourfindings.
In conclusion, this study showed a high prevalence of
FM in obese patients with indication for bariatric surgery. RegardingtheassociationbetweenFMandobesity,depression wasshowntobeanimportantfactor.FMbringsanadditional impacttothequalityoflifeofobesepatients,makingtheir treatmentanextrachallenge,whichcertainlydeservesa mul-tidisciplinaryapproach.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. KimCH,LuedtkeCA,VincentA,ThompsonJM,OhTH. Associationofbodymassindexwithsymptomseverityand qualityoflifeinpatientswithfibromyalgia.ArthritisCareRes (Hoboken).2012;64:222–8.
2.WolfeF,ClauwDJ,FitzcharlesMA,GoldenbergDL,KatzRS, MeaseP,etal.TheAmericanCollegeofRheumatology preliminarydiagnosticcriteriaforfibromyalgiaand measurementofsymptomseverity.ArthritisCareRes (Hoboken).2010;62:600–10.
3.WolfeF,ClauwDJ,FitzcharlesMA,GoldenbergDL,HäuserW, KatzRS,etal.Fibromyalgiacriteriaandseverityscalesfor clinicalandepidemiologicalstudies:amodificationofthe ACRPreliminaryDiagnosticCriteriaforFibromyalgia.J Rheumatol.2011;38:1113–22.
4.OkifujiA,HareBD.Theassociationbetweenchronicpainand obesity.JPainRes.2015;8:399–408.
5.UrsiniF,NatyS,GrembialeRD.Fibromyalgiaandobesity:the hiddenlink.RheumatolInt.2011;31:1403–8.
6.SaberAA,BorosMJ,ManclT,ElgamalMH,SongS, WisadrattanapongT.TheeffectoflaparoscopicRoux-en-Y gastricbypassonfibromyalgia.ObesSurg.2008;18:652–5. 7.BurckhardtCS,ClarkSR,BennettRM.Thefibromyalgia
impactquestionnaire:developmentandvalidation.J Rheumatol.1991;18:728–33.
8.MarquesA,SantosA,Assumpc¸ãoA,MatsutaniL,LageL, PereiraC.ValidationoftheBrazilianversionofthe
FibromyalgiaImpactQuestionnaire(FIQ).RevBrasReumatol. 2006;46:24–31.
9.RezendeMC,PaivaES,HelfensteinMJr,RanzolinA,Martinez JE,ProvenzaJR,etal.EpiFibro–umbancodedadosnacional sobreasíndromedafibromialgia–análiseinicialde500 mulheres.RevBrasReumatol.2013;53:382–7.
10.WolfeF,RossK,AndersonJ,RussellIJ,HebertL.The prevalenceandcharacteristicsoffibromyalgiainthegeneral population.ArthritisRheum.1995;38:19–28.
11.SennaMK,SallamRAR,AshourHS,ElarmanM.Effectof weightreductiononthequalityoflifeinobesepatientswith fibromyalgiasyndrome:arandomizedcontrolledtrial.Clin Rheumatol.2012;31:1591–7.
12.CorderoMD,Alcocer-GómezE,Cano-GarcíaFJ,
Sánchez-DomínguezB,Fernández-RiejoP,FernándezAMM, etal.Clinicalsymptomsinfibromyalgiapatientsare associatedtooverweightandlipidprofile.RheumatolInt. 2014;34:419–22.
13.DeAraújoTA,MotaMC,CrispimCA.Obesityandsleepiness inwomenwithfibromyalgia.RheumatolInt.2015;35:281–7. 14.ArreghiniM,ManzoniGM,CatelnuovoG,SantovitoC,
CapodaglioP.Impactoffibromyalgiaonfunctioninginobese patientsundergoingcomprehensiverehabilitation.PLOS ONE.2014;9:e91392.
15.SennaMK,AhmadHS,FathiW.Depressioninobesepatients withprimaryfibromyalgia:themediatingroleofpoorsleep andeatingdisorderfeatures.ClinRheumatol.2013;32: 369–75.