SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Review
Article
Outcome
assessment
in
the
treatment
of
rotator
cuff
tear:
what
is
utilized
in
Brazil?
夽
Jorge
Henrique
Assunc¸ão
∗,
Eduardo
Angeli
Malavolta,
Vitor
Rodrigues
Domingues,
Mauro
Emilio
Conforto
Gracitelli,
Arnaldo
Amado
Ferreira
Neto
UniversidadedeSãoPaulo,FaculdadedeMedicina,HospitaldasClínicas,InstitutodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received16June2016 Accepted26July2016
Availableonline1September2017
Keywords: Shoulder
Evaluationofresultsoftherapeutic interventions
Rotatorcuff
a
b
s
t
r
a
c
t
Thisreviewevaluatedtheoutcomesusedinclinicalstudiesinvolvingrotatorcufftear pub-lishedinthelastdecadeinthetwoleadingBrazilianorthopedicjournals.Aliteraturereview wasperformed usingthe journals RevistaBrasileira de OrtopediaandActaOrtopédica Brasileira.Itincludedalloriginalclinicalarticlesdescribingatleastoneoutcomemeasured beforeorafteranyclinicalorsurgicalinterventionrelatedtorotatorcufftear,published between2006and2015.Theauthorsevaluatedrangeofmotion,musclestrength,patient satisfaction,andtendonintegrityandfunctionaloutcomesscores.Therewere25clinical studiespublishedaboutrotatorcuffinthetwoprincipalBrazilianorthopedicjournalsinthe lastdecade,20caseseries(80%),onecase–control(4%),andfourcohorts(16%).Objective measuressuchasmusclestrength,patientsatisfaction,andevaluationoftendonintegrity werelittleused.Rangeofmotionmeasurementswereperformedin52%ofthearticles. Evaluationsofmusclestrengthandpatientsatisfactionwerereportedby28%and16%of thestudies,respectively.Only28%ofthearticlesevaluatedtendonintegrityaftersurgery. Ofthese,16%didsobymagneticresonanceimagingand12%byultrasonography.Themost usedscalewastheUCLA,presentin92%ofthearticles,whiletheConstant–Murleyappeared in20%.Scalesdeemedreliable,withhighinternalconsistencyandgoodresponsiveness, wererarelyused.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
PaperdevelopedatUniversidadedeSãoPaulo,FaculdadedeMedicina,HospitaldasClínicas,InstitutodeOrtopediaeTraumatologia, GrupodeOmbroeCotovelo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](J.H.Assunc¸ão).
http://dx.doi.org/10.1016/j.rboe.2017.08.013
Avaliac¸ão
dos
desfechos
no
tratamento
da
rotura
do
manguito
rotador:
o
que
usamos
no
Brasil?
Palavras-chave: Ombro
Avaliac¸ãoderesultadode intervenc¸õesterapêuticas Manguitorotador
r
e
s
u
m
o
Avaliamososdesfechosusadosnosestudosclínicosqueenvolvemroturadomanguito rota-dorpublicadosnaúltimadécadanosdoisprincipaisperiódicosortopédicosbrasileiros.Foi feitaumarevisãodaliteraturanosperiódicosRevistaBrasileiradeOrtopediaeActaOrtopédica Brasileira.Foramincluídos todosos artigosclínicos originaisquedescreviam aomenos umamedidadedesfechoantesouapósalgumaintervenc¸ãoclínicaoucirúrgicareferente aomanguitorotadorpublicadosentre2006e2015.Osdesfechosavaliadosforamarcode movimento,forc¸amuscular,satisfac¸ão,integridadetendíneaeescalasclínicas.Foram publi-cados25estudosclínicossobremanguitorotadornosdoisprincipaisperiódicosortopédicos brasileirosnaúltimadécada,20sériesdecasos(80%),umestudotipocaso-controle(4%) equatrocoortes(16%).Medidasobjetivascomoforc¸amuscular,satisfac¸ãodopacientee avaliac¸ãodaintegridadetendíneaforampoucoempregadas.Asmedidasdoarcode movi-mentoforamdescritasem52%dosartigos.Aavaliac¸ãodaforc¸amusculareasatisfac¸ão dopaciente foramdescritas em28% e16%dos estudos,respectivamente. Apenas28% dosartigosavaliaramaintegridadetendíneaapósacirurgia.Desses,16%ofizeramcom aressonânciamagnéticae12%comaultrassonografia.AescalamaisusadafoiadaUCLA, presenteem92%dosartigos,enquantoadeConstant-Murleyfoiusadaem20%.Escalas consideradasconfiáveis,comgrandeconsistênciainternaeboaresponsividade,raramente foramusadas.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Shoulderpainhasahighprevalenceinthepopulation,ranging from7to26%.1Rotatorcuffconditions,themaincauseofpain
intheshouldergirdle,affect20%ofthegeneralpopulationand upto50%ofpatientsover80years.2
Standardizedclinicalassessmentisessentialtodetermine theefficacyofatreatmentandalsotocomparetheresultsof differentstudies;itiscrucialinclinicalresearch.3,4Methods
forevaluatingtheresultsoforthopedictreatmenthavebeen modifiedinrecentyears.5,6 Previously, measurementswere
based on physicalexamination, byexamining joint mobil-ityandmusclestrength.However,questionnairesorclinical scaleshavebeendevelopedthathaveimprovedtheevaluation ofresults.7,8 However,thereisawidevariationinthe
mea-surementtools.9Morethan40scalesaredescribedtoassess
shoulderpainandfunction.10Inaddition,themeasurement
oftherangeofmotionandstrength,andthedescriptionofthe imagingfindingsalsodonothaveaconsensus.9
Makhnietal.9recentlypublishedareviewinvolvingthesix
leadinginternationalorthopedicjournals,anddescribedthe toolsusedtoassessoutcomeinrotatorcuffdisorders.Wedo nothaveasurveyshowingthemaintypesofclinical evalu-ationinBrazil.Mostinstruments havebeendevelopedand evaluatedintheEnglishlanguage.10Fortheseinstrumentsto
beusedinBrazil,translation,culturaladaptation,aswellas teststhatevaluatemeasurementpropertiesofthese instru-ments,suchasinternalconsistency,reproducibility,validity andresponsivenessarerecommended.5
Theobjective ofthisstudy wastoevaluatetheoutcome usedinclinical studiesinvolvingtherotator cuffpublished
in the last decade in the two main Brazilian orthopedic journals.
Methods
Design
A literaturereviewwas performedin thetwo main Brazil-ianorthopedicjournals,RevistaBrasileiradeOrtopedia(RBO) and Acta Ortopédica Brasileira. The period covered was one decade (January 2006 to December 2015). This study was approved bythe local Ethics Committeewith number 1197.
Searchstrategy
Thesearchstrategyinitiallyincludedthereadingofalltitles ofthearticlesbyoneoftheauthors(JHA),usingthejournals’ tableofcontents.Incasesofdoubtwiththereadingofthetitle, theabstractwasevaluated.Thisway,allarticlesthatdidnot involvetheshoulderjointwereexcluded.Thentheabstracts werereadbythreeauthors(JHA,EAMandVRD)and,if neces-sary,thefulltext,todetermineifthearticlefittheselection criteria.Incaseofdisagreementintheselectionofaparticular articleamongthethreeauthors,whetherincludingitornot wasdefinedbyconsensus.
Selectioncriteria
one outcome measure before or aftera certain clinical or surgical intervention for the rotator cuff were included. Casereports, description ofsurgical technique, articles on diagnostic methods accuracy, anatomical studies, articles involvinganimalsorcadavers,basicscienceorreviewswere excluded.
Outcomes
Dataregardingthestudytitle,yearandvolumeofthe publi-cation,casuistry,minimumfollow-up,regularfollow-upand levelofevidencewere tabulated.Inaddition, the following outcomeswereassessed:
Rangeofmotion
Theevaluationoftherangeofmotionwasinvestigated:frontal flexion,elevation,abduction,lateralrotation(withthearmat thesideofthebodyorabduction)andmedialrotation(with thehandtowardthebackorwiththearminabduction).The measureinanyoftheaforementionedpositionswaslisted. Datawereonlyconsideredifquantitativelydescribedinthe resultssection.Thepositionofthepatient(supine,sittingor inaorthostaticposition)andtheuse ofagoniometerwere alsoevaluated.
Musclestrength
Thepositioninwhichstrength wasevaluatedwasstudied: frontalflexion,elevation,abduction,lateralrotation(withthe armatthesideofthebodyorabduction)andmedialrotation (withthe handtoward thebackor withthearmin abduc-tion).Themeasureinanyofthepositionswaslisted.Data wereonlyconsideredifquantitativelydescribedintheresults section.Thepositionofthe patient (supine, sitting orin a orthostaticposition)andtheuseofdynamometerwerealso evaluated.Manual evaluationdata(graduationfrom0to5) werecomputed.Dataonasubdomainofaclinicalscalewere alsoreported.
Tendonintegrity
The imaging method used (magnetic resonance with or withoutcontrast,computedtomographywithorwithout con-trast orultrasonography) was evaluated. Radiographs were notanalyzed.Theperiodicityand timinginwhichthetest was performed were reported. The use of some integrity assessmentscales,orcategoricalevaluationinrupturedand intact tendons has been described. We also describe the presenceorabsence ofdata relatedtothe acquisition and analysis of imaging tests: device used, evaluators, images obtained.
Satisfaction
Any data regarding patient satisfaction was studied. This included questions regarding treatment satisfaction or whether thepatient wouldrecommend the procedureto a thirdpartyor if theywould havesurgeryagain. Data on a subdomainofaclinicalscalewerealsoreported.
Evaluationscalesandquestionnaires
Thefunctionalscalesandtheevaluationquestionnairesused bytheauthorswereevaluated.Wealsoreportedstudiesthat usedvisualanaloguescale(VAS)forpainorfunction.
Statisticalanalysis
Datawereexposedinadescriptiveway,bymeansofabsolute numbersandpercentage.
Results
Intheperiodevaluated,712originalarticleswerepublished in the Brazilian Journal of Orthopedics and 588 in Acta OrtopédicaBrasileira,or1300publications.Amongthese,84 (6.7%ofthetotal)wereclinicalarticlesonshoulderdiseases; 25publications(1.9%ofthetotal)11–35 evaluatedtheclinical
results of treatment ofrotator cuff tears (Table 1); twenty studies(80%)werecaseseries(levelofevidenceIV),one(4%) case–controlstudy(levelofevidenceIII)andfour(16%)cohorts (levelofevidenceII).Norandomizedstudywaspublishedin theperiod.Westudied1651shoulders,66.1±50.3shoulders perstudy.Eightarticles(32%)hadfollow-uptimeofpatients greater thantwoyears andonlytwo(8%) followedupwith standardizedassessment time.The mean ofthe evaluated outcomewas2.2±1.1(Fig.1).
Rangeofmotion
Among the studies evaluated, 12 (48%) did not report the measurementoftherangeofmotioninanypositioninthe postoperative period. Nine articles (36%) presentedmedial rotation,11(44%)evaluatedthelateralrotation,samenumber foundofpublicationsthatevaluatedthepatients’elevation. Threepublications(12%)evaluatedonlyonepositionofthe rangeofmotion,one(4%)evaluatedtwopositionsandnine (36%)presentedthemeasurementsoftherangeofmotionin threepositions(Fig.2).Themethodologyappliedinthe mea-surementoftherangeofmotionwasreportedinseven(28%) articles,theothersdidnotreporttheuseofgoniometer,the measurementtechniqueorthepatientposition.
Musclestrength
Musclestrengthafterrotatorcuffrepairwasreportedinseven studies(28%).Inthreestudies(12%)itwaspresentedasa sub-domainofafunctionalscale,andintwoarticles(8%)itwas reportedcategoricallywiththeuseofthecontralateralside asareference.Twostudies(8%)usedquantitative measure-mentofmusclestrengthusingadynamometerandreported the patient’s position (orthostatic).Six studies(24%) evalu-atedonlyonepositionmovement(elevationorabduction),one study15evaluatedtheelevationandlateralrotation.
Tendonintegrity
Table1–Publicationsontreatmentofrotatorcufftearsbetween2006and2015.
Author(s) Title Journal Year Volume
(number)
Pages
Pecoraetal. Prognosticfactorsfortheclinicaloutcomefollowingrotator cuffrepair
ActaOrtopédica Brasileira
2015 23(3) 146–149
Portoetal. Evaluationofpatientsundergoingrotatorcuffsuturewiththe modifiedMason-Allentechnique
ActaOrtopédica Brasileira
2013 21(3) 167–169
Ramosetal. Resultsofarthroscopictreatmentofrotatorcufftears ActaOrtopédica Brasileira
2010 18(1) 15–18
Checchiaetal. Isolatedtearofthesubscapulartendon ActaOrtopédica Brasileira
2009 17(1) 26–30
Veadoetal. Rotatorcufftearinpatientsover65years:evaluationof function,integrityandstrength
RevistaBrasileirade Ortopedia
2015 50(3) 318–323
Miyazakietal. Evaluationofresultsofarthroscopicsurgicaltreatmentof rotatorcufftearsinpatients≥65years
RevistaBrasileirade Ortopedia
2015 50(3) 305–311
Godinhoetal. Long-termfunctionalevaluationofvideoarthroscopic treatmentofpartialtearsoftherotatorcuff
RevistaBrasileirade Ortopedia
2015 50(2) 200–205
Godinhoetal. Resultofarthroscopicsurgicaltreatmentofretearsofthe shoulderrotatorcuff
RevistaBrasileirade Ortopedia
2015 50(1) 89–93
Almeidaetal. Comparativeanalysisofarthroscopicsutureoflargeand extensivetearsoftherotatorcuffrelatedtothelevelof osteopenia
RevistaBrasileirade Ortopedia
2015 50(1) 83–88
Miyazakietal. Functionalevaluationofarthroscopicrepairoftherotatorcuff tearsinpseudoparalysispatients
RevistaBrasileirade Ortopedia
2014 49(2) 178–182
Ikemotoetal. Evaluationoftheclinical-functionalresultsoftherepairof extensiverotatorcufftearwithinclusionofthetendonofthe longheadofthebiceps
RevistaBrasileirade Ortopedia
2013 48(2) 165–169
Malavoltaetal. Platelet-richplasmainthearthroscopicrepairofcomplete tearsoftherotatorcuff
RevistaBrasileirade Ortopedia
2012 47(6) 741–747
Ikemotoetal. Arthroscopicrepairofsmallandmediumtearsofthe supraspinalmuscletendon:evaluationofclinical-functional resultsaftertwoyearsoffollow-up
RevistaBrasileirade Ortopedia
2012 47(4) 436–440
Godinhoetal. Resultsofthearthroscopicrepairofisolatedtearsofthe subscapularmuscletendon
RevistaBrasileirade Ortopedia
2012 47(3) 330–336
Veadoetal. Prospectiveandcomparativestudyofthefunctionalresults aftertheopenandarthroscopicrepairofrotatorcufftears
RevistaBrasileirade Ortopedia
2011 46(5) 546–552
Miyazakietal. Evaluationofresultsofthearthroscopicrepairofrotatorcuff tearsinpatientsupto50yearsofage
RevistaBrasileirade Ortopedia
2011 46(3) 276–280
Almeidaetal. Comparativeanalysisoftheresultofarthroscopicsutureofthe rotatorcuffinsmokingandnon-smokingpatients
RevistaBrasileirade Ortopedia
2011 46(2) 172–175
Miyazakietal. Evaluationofresultsofreoperationsofpatientswithrotator cufftears
RevistaBrasileirade Ortopedia
2011 46(1) 45–50
Veadoetal. Functionalevaluationofpatientsundergoingarthroscopic debridementforthetreatmentofextensiveandirreparable tearsoftherotatorcuff
RevistaBrasileirade Ortopedia
2010 45(5) 426–431
Godinhoetal. Evaluationoftheanatomicalintegritythroughultrasoundand functionalintegritythroughConstant&Murleyindexofthe rotatorcuffafterarthroscopicrepair
RevistaBrasileirade Ortopedia
2010 45(2) 174–180
Miyazakietal. Extensivetearsoftherotatorcuff:evaluationofresultsofthe arthroscopicrepair
RevistaBrasileirade Ortopedia
2009 44(2) 148–152
Veadoetal. Functionalevaluationofthearthroscopicrepairofcomplete tearsoftherotatorcuffassociatedwithacromyoplasty
RevistaBrasileirade Ortopedia
2008 43(11/12) 505–512
Balsinietal. Arthroscopicrepairofcompleteisolatedtearsofthe subescapular
RevistaBrasileirade Ortopedia
2008 43(11/12) 497–504
Veadoetal. Functionalandstructuralanalysisofrotatorcuffextensive tearsrepair
RevistaBrasileirade Ortopedia
2006 41(8) 294–301
Veadoetal. Efficacyofarthroscopicdebridementinpartialrotatorcuff tears
RevistaBrasileirade Ortopedia
2006 41(1/2) 22–28
publications(16%) usednon-enhancedmagneticresonance
imagingtocheckfortendonintegrity,andinthree(12%)an ultrasoundexamwasused.Allstudiesusedonlya categori-calevaluation,completeorrupturedrepair.Onlythreestudies (12%)mentionthenumberofevaluatorsandintwo(8%)the specificationsofthedeviceusedarereported.Nostudy men-tionsimageacquisitionprotocols.Thetestsweredoneonce
inallstudies,andonlyonestudyperformedtheexamona regularbasis(12months).22
Satisfaction
50
40
30
20
10
0
1 2
Number of outcomes evaluated
Percentage of studies
3 4
4 8
20 44
24
5
Fig.1–Percentagedistributionofnumberofoutcomes analyzedperstudy.
50
40
30
20
10
0
0 1
Range of motion position evaluated
Percentage of studies
2 4 12
36 48
3
Fig.2–Percentagedistributionofnumberofrangeof motionpositionsevaluatedperstudy.
agree to undergo treatment again, and two (8%) assessed satisfactionthrough asimplequestion withtwocategories (satisfied/dissatisfied).
Evaluationscalesandquestionnaires
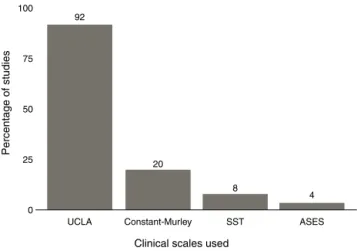
Of the 25 studies included, 23 (92%) used the University of California, Los Angeles Shoulder Rating Scale (UCLA),36
five papers (20%) used the Constant–Murley evaluation questionnaire,37 two(8%)evaluatedtheresultsthroughthe
Simple Shoulder Test (SST)38 and one (4%) through the
questionnaireAmericanShoulderandElbowSurgeons Stan-dardized Shoulder Assessment Form (ASES)39 (Fig. 3); 20
publications(80%)usedonlyonescale,four(16%)madethe evaluationthrough twoscales and one study (4%)through threequestionnaires.Infourarticles(16%)VASwasusedto quantifypainbeforeandaftertreatment.
Discussion
Rotatorcufftearisthemaincauseofshoulderpain2andthe
repairofthe rotatorcuffisthe mostcommonlyperformed surgeryofthisjoint.40However,intheperiodevaluated,only
100
75 92
20
UCLA Constant-Murley SST ASES
Clinical scales used
Percentage of studies
8
4 50
25
0
Fig.3– Percentageofstudiesusingclinicalscales.
25publicationswerefoundthatevaluatedtheclinicalresults ofthetreatmentofrotatorcufftearsinthetwomain Brazil-ianjournalsoforthopedicsandtraumatology.Thenational average was 2.5 articles per year. Between 2010 and 2014, an average of4.8and 8.8articles per year were published inthetwomajorcomprehensiveorthopedicjournals,Journal ofBone&JointSurgeryandTheAmericanJournalofSports Medicine,respectively.
TheBrazilianstudiesevaluatedtheresultswithameanof 2.2outcomesperarticle,anumber thatwassimilartothat observedininternationalstudies.9However,only32%ofthe
studieshadpatients’follow-upofmorethantwoyears,and 8%had afollow-up withstandardizedevaluationtime.We alsofoundthatnationalpublicationsonthistopichavealow levelofevidence,80%werecaseseries,andwedidnotfind anarticlewithlevelIevidence,unlikethemainforeign jour-nals,whichreport13%ofstudieswithlevelI,17%withlevel II,26%withlevelIII,andonly43%withlevelIV.9The
predom-inanceofcaseseriesisacharacteristicofBrazilianorthopedic publications.41
ThemostusedevaluationquestionnaireforBrazilian stud-ieswastheUCLAscale,usedin92%ofthepublications.This numberisfarsuperiortothatofMakhnietal.,9whofound
that it had been usedonly in35% of articles, the thirdin prevalence. This scale was initially developed for patients undergoingtotalshoulderarthroplasty.42Ellmanetal.43were
thefirstauthorstoapplythistooltoevaluatetheresultsofthe treatmentofrotatorcufftears;sincethen,ithasbeenused inseveralpublications.However,therearenostudiesto vali-dateitsdevelopmentandtheapplicationofthisinstrument inthesepatients. Itisconsidered ascale withlow reliabil-ityandvalidity,andhasseverallimitationsinthecollection ofinformation.44 Arecentsystematicreviewcomparingthe
assessmentscalesforshoulderdiseasesfoundthatthebest are the ASES, SST and OxfordShoulder Scorescales. They areconsideredreliable,withgreatinternalconsistency,good responsivity, and were previouslyvalidated.45 In ourstudy,
onlyonepublication(4%)18usedtheASESscale,andtwo
stud-ies (8%)15,32 usedSSTforevaluation.Ontheirturn,Makhni
etal.9observedthatthepublicationsofthesixmajor
consideredmorereliable;ASESquestionnairewasusedin59%, andtheSSTin28%.
TheConstant–Murleyscale37 wasthesecondmostused,
obsrvedinfivearticles(20%).Thisscaleisthemostusedin internationallypublishedstudies(61%ofpublications).This toolhasasmainlimitationthedifficultyandvariabilityforthe evaluationoftheabductionstrength,whichrepresents25% ofits totalscore.Severalauthorsreportits inconsistency,46
depending on the dynamometer used,47 on the degree of
shoulderabductionandrotation,48andonstrength relative
toageandgender.49Onlyrecentlyhasthisscalebeen
trans-lated and culturally adaptedto the Portugueselanguage.37
Indexesofnormalityareavailableforsomecountriesbuthave notbeenvalidatedinBrazil.49Webelievethattheuseofthe
Constant–MurleyIndividualRelativeScale,whencomparedto thecontralateralshoulderwhenitisasymptomatic,theuseof digitaldynamometers,andscaletrainingreducedbiasinthe useofthisinstrument.50–52
IntheBrazilianjournals,only28%ofstudiesevaluate tendi-nousintegrityaftersurgery. Ofthese,16% dosowithMRI, and12%withultrasound.Thesevaluesarelowerthanthose reportedininternationaljournals,inwhich65%ofthestudies useimaginginthepostoperativeperiod,MRIiscitedin38%, ultrasoundin31%,andarthrotomographyin8%.9Inaddition,
noneofthe articlesevaluating integritythroughMRIuse a scaleofevaluation,onlythestratificationintointactand rup-tured.Exceptforthedeterminationofthesimpleabsenceor presenceofatear,theclassificationproposedbySugayaetal.53
isthemostusedandreliable,citedin33studiesinarecent meta-analysis.54
Ourresultsshowthatthedescriptionofmeasuresofthe rangeofmotionismadein52%ofthearticles,afigureslightly lowerthanthe63%reportedinforeignjournals.9 Thesame
occursregardingevaluationofstrength,describedin28%of nationalstudies,and38%ofinternationalones.9Satisfaction,
initsturn,isevaluatedinonly16%ofthestudies,considerably lessthanthe54%foundininternationalstudies.9 However,
fewarticleshavereportedthemethodologyusedtoevaluate thesemeasuresclearlyandreproducibly.Itshouldbenoted thatnoneofthenationalstudiesusedtoolstomeasurequality oflife, unlikeinternational journals, whichcite these out-comesinmorethan15%ofcases.9
Ourstudy hassomelimitations.Itincluded all typesof clinical studies,thus havinglevel IVofevidence. However, thegreaterpossibilityofbiasinarticlesoflowerlevelof evi-dencedidnotinfluenceourresults,sinceweevaluatedthe toolsused,nottheoutcomesthemselves.Inaddition,wehave reviewedthe articlesofonly onedecade and two national journals.Theaimofthisapproachwastoplotthenational pictureinarelativelyrecentperiod.Finally,oursearch strat-egymayhaveincludedarticlesbyforeignauthorspublished innationaljournals,anddidnotincludearticlesbyBrazilian authorspublishedininternationaljournals.
Webelievethat themembers ofthe BrazilianSocietyof ShoulderandElbowSurgeryshouldinitiate adiscussionto standardize the evaluation tools. Attitudes such as these, already takenbyUS55 and Japan56 societies,facilitate data
comparison amongthe studies, allow for more consistent exposureofresults, and increase the possibilitiesofciting nationalarticles.ASESandSSTscale,alreadyvalidatedforthe
Portugueselanguage,andwithgoodreliability,38,57shouldbe
prioritized,alongwiththeConstant–Murleyscaleadjustedfor genderandage;normalityindicesshouldbeobtainedforthe Brazilianpopulation. Inaddition,qualityoflifeassessment shouldbeencouraged.Likewise,theassessmentofstrength andamplitudecouldbeinlinewiththatusedininternational studies.Theassessmentoftendinousintegrityaftersurgery shouldbeencouragedandwhenMRIisused,itshouldbemade throughtheclassificationbySugayaetal.53
Final
considerations
Twenty-fiveclinicalstudiesonrotatorcuffwerepublishedin thetwomainBrazilianorthopedicjournalsinthelastdecade. ThemostusedscalewasUCLA,presentin92%ofthearticles. Scalesconsideredreliable,withgreatinternalconsistencyand good responsiveness, were rarelyused.Objective measures suchasmusclestrength,patientsatisfactionandevaluation oftendonintegritywerepoorlyused.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.LuimeJJ,KoesBW,HendriksenIJM,BurdorfA,VerhagenAP, MiedemaHS,etal.Prevalenceandincidenceofshoulderpain inthegeneralpopulation;asystematicreview.ScandJ Rheumatol.2004;33(2):73–81.
2.YamamotoA,TakagishiK,OsawaT,YanagawaT,NakajimaD, ShitaraH,etal.Prevalenceandriskfactorsofarotatorcuff tearinthegeneralpopulation.JShoulderElbSurg. 2010;19(1):116–20.
3.GartsmanGM,BrinkerMR,KhanM.Earlyeffectivenessof arthroscopicrepairforfull-thicknesstearsoftherotatorcuff: anoutcomeanalysis.JBoneJtSurgAm.1998;80(1):33–40.
4.GartsmanGM,MorrisBJ,UngerRZ,LaughlinMS,ElkousyHA, EdwardsTB.Characteristicsofclinicalshoulderresearchover thelastdecade:areviewofshoulderarticlesinTheJournalof Bone&JointSurgeryfrom2004to2014.JBoneJtSurgAm. 2015;97(5):e26.
5.PugaVO,LopesAD,CostaLO.Avaliac¸ãodasadaptac¸ões transculturaisepropriedadesdemedidadequestionários relacionadosàsdisfunc¸õesdoombroemlínguaportuguesa: umarevisãosistemática.RevBrasFisioter.2012;16(2):85–93.
6.BrinkerMR,CuomoJS,PophamGJ,O’ConnorDP,BarrackRL. Anexaminationofbiasinshoulderscoringinstruments amonghealthycollegiateandrecreationalathletes.J ShoulderElbSurg.2002;11(5):463–9.
7.GarrattA,SchmidtL,MackintoshA,FitzpatrickR.Qualityof lifemeasurement:bibliographicstudyofpatientassessed healthoutcomemeasures.BMJ.2002;324(7351):1417.
8.HigginsonIJ,CarrAJ.Measuringqualityoflife:usingquality oflifemeasuresintheclinicalsetting.BMJ.
2001;322(7297):1297–300.
9.MakhniEC,SteinhausME,MorrowZS,JobinCM,VermaNN, ColeBJ,etal.Outcomesassessmentinrotatorcuffpathology: whatarewemeasuring?JShoulderElbSurg.
10.HarvieP,PollardTCB,ChennagiriRJ,CarrAJ.Theuseof outcomescoresinsurgeryoftheshoulder.JBoneJtSurgBr. 2005;87(2):151–4.
11.PecoraJOR,MalavoltaEA,Assunc¸ãoJH,GracitelliME,Martins JP,FerreiraAAJr.Fatoresprognósticosparaoresultadoclínico apósoreparodomanguitorotador.ActaOrtopBras.
2015;23(3):146–9.
12.PortoFM,AlvesMW,deAndradeAL.Avaliac¸ãodepacientes submetidosàsuturadomanguitorotadorcomatécnicade mason-allenmodificada.ActaOrtopBras.2013;21(3): 167–9.
13.RamosCH,SallumJS,SobaniaRL,BorgesLG,SolaWCJr, RibeiroLY.Resultadosdotratamentoartroscópicodas rupturasdomanguitorotador.ActaOrtopBras. 2010;18(1):15–8.
14.ChecchiaSL,MiyazakiAN,FregonezeM,dosSantosPD,Silva LA,OrtizRT,etal.Lesãoisoladadotendãodosubescapular. ActaOrtopBras.2009;17(1):26–30.
15.deCastroVeadoMA,PrataEF,GomesDC.Lesãodomanguito rotadorempacientesmaioresde65anos:avaliac¸ãoda func¸ão,integridadeeforc¸a.RevBrasOrtop.2015;50(3):318–23.
16.MiyazakiAN,SilvaLAda,SantosPD,ChecchiaSL,CohenC, GioraTS.Avaliac¸ãodosresultadosdotratamentocirúrgico artroscópicodaslesõesdomanguitorotadorempacientes com65anosoumais.RevBrasOrtop.2015;50(3):305–11.
17.GodinhoGG,Franc¸aFO,FreitasJMA,LagoE,SantosFM, ResendeDS,etal.Avaliac¸ãofuncionalemlongoprazodo tratamentovideoartroscópicodaslesõesparciaisdo manguitorotador.RevBrasOrtop.2015;50(2):200–5.
18.GodinhoGG,Franc¸aF,deO,FreitasJMA,SantosFM,Prandini A,etal.Resultadodotratamentocirúrgicoartroscópicodas rerrupturasdomanguitorotadordoombro.RevBrasOrtop. 2015;50(1):89–93.
19.AlmeidaA,AttiV,AgostiniDC,ValinMR,deAlmeidaNC, AgostiniAP.Análisecomparativadasuturaartroscópicade lesõesgrandeseextensasdomanguitorotadorcomrelac¸ão aograudeosteopenia.RevBrasOrtop.2015;50(1):83–8.
20.MiyazakiAN,FregonezeM,SantosPD,daSilvaLA,doVal SellaG,NetoDL,etal.Avaliac¸ãofuncionaldoreparo artroscópicodalesãodomanguitorotadorempacientescom pseudoparalisia.RevBrasOrtop.2014;49(2):178–82.
21.IkemotoRY,MurachovskyJ,NascimentoLGP,BuenoRS, AlmeidaLH,StroseE,etal.Avaliac¸ãodosresultados clínico-funcionaisdoreparodalesãoextensadomanguito rotadorcominclusãodotendãodacabec¸alongadobíceps. RevBrasOrtop.2013;48(2):165–9.
22.MalavoltaEA,GracitelliMEC,SunadaEE,BenegasE,PradaFS, BolligerNetoR,etal.Plasmaricoemplaquetasnoreparo artroscópicodasroturascompletasdomanguitorotador.Rev BrasOrtop.2012;47(6):741–7.
23.IkemotoRY,MurachovskyJ,NascimentoLGP,BuenoRS, AlmeidaLH,StroseE,etal.Reparac¸ãoartroscópicadelesões pequenasemédiasdotendãodomúsculosupraespinal: avaliac¸ãodosresultadosclínico-funcionaisapósdoisanosde seguimento.RevBrasOrtop.2012;47(4):436–40.
24.GodinhoGG,Franc¸aF,deO,FreitaJMA,SantosFM,dosSantos RB,etal.Resultadosdoreparoartroscópicodasroturas isoladasdotendãodomúsculosubescapular.RevBrasOrtop. 2012;47(3):330–6.
25.VeadoMAC,CastilhoRS,MaiaPE,RodriguesAU.Estudo prospectivoecomparativodosresultadosfuncionaisapós reparoabertoeartroscópicodaslesõesdomanguitorotador. RevBrasOrtop.2011;46(5):546–52.
26.MiyazakiAN,FregonezeM,SantosPD,daSilvaLA,ValSellaG, SantosRM,etal.Avaliac¸ãodosresultadosdoreparo
artroscópicodelesõesdomanguitorotadorempacientes comaté50anosdeidade.RevBrasOrtop.2011;46(3): 276–80.
27.AlmeidaA,ValinMR,ZampieriR,deAlmeidaNC,RovedaG, AgostiniAP.Análisecomparativadoresultadodasutura artroscópicadalesãodomanguitorotadorempacientes fumantesenãofumantes.RevBrasOrtop.2011;46(2): 172–5.
28.MiyazakiAN,FregonezeM,SantosPD,daSilvaLA,doVal SellaG,SantosRM,etal.Avaliac¸ãodosresultadosdas reoperac¸õesdepacientescomlesõesdomanguitorotador. RevBrasOrtop.2011;46(1):45–50.
29.VeadoMAC,RodriguesAU.Avaliac¸ãofuncionaldospacientes submetidosaodesbridamentoartroscópicoparatratamento dasrupturasextensaseirreparáveisdomanguitorotador. RevBrasOrtop.2010;45(5):426–31.
30.GodinhoGG,Franc¸aFO,FreitasJM,WatanabeFN,NobreLO, AlmeidaNetoMA,etal.Avaliac¸ãodaintegridadeanatômica porexamedeultrassomefuncionalpeloíndicedeConstant &Murleydomanguitorotadorapósreparoartroscópico.Rev BrasOrtop.2010;45(2):174–80.
31.MiyazakiAN,FregonezeM,SantosPD,SilvaLA,PintoCM, OrtizRT,etal.Lesõesextensasdomanguitorotador: avaliac¸ãodosresultadosdoreparoartroscópico.RevBras Ortop.2009;44(2):148–52.
32.VeadoMA,AlmeidaFilhoIA,DuarteRG,LeitãoI.Avaliac¸ão funcionaldoreparoartroscópicodaslesõescompletasdo manguitorotadorassociadoaacromioplastia.RevBrasOrtop. 2008;43(11/12):505–12.
33.BalsiniNE,BalsiniN,KochenL,PalkaLJ,VilelaA,dosSantos JS.Reparoartroscópicodaslesõescompletasisoladasdo subescapular.RevBrasOrtop.2008;43(11/12):
497–504.
34.VeadoAM,GomesTP,PintoRZ.Análisefuncionaleestrutural doreparodaslesõesextensasdomanguitorotador.RevBras Ortop.2006;41(8):294–301.
35.VeadoAM,BertoliniFM,MaiaPE,RodriguesAU.Eficáciado desbridamentoartroscópiconaslesõesparciaisdomanguito rotador.RevBrasOrtop.2006;41(1/2):22–8.
36.OkuEC,AndradeAP,StadinikySP,CarreraEF,TelliniGG. Traduc¸ãoeadaptac¸ãoculturaldoModified-Universityof CaliforniaatLosAngelesShoulderRatingScaleparaalíngua portuguesa.RevBrasReumatol.2006;46(4):246–52.
37.BarretoRP,BarbosaML,BalbinottiMA,MothesFC,daRosaLH, SilvaMF.TheBrazilianversionoftheConstant–MurleyScore (CMS-BR):convergentandconstructvalidity,internal consistency,andunidimensionality.RevBrasOrtop. 2016;51(5):515–20.
38.NetoJOB,GesserRL,SteglichV,BonilauriFerreiraAP,Gandhi M,VissociJR,etal.ValidationoftheSimpleShoulderTestina Portuguese-Brazilianpopulation.Isthelatentvariable structureandvalidationoftheSimpleShoulderTestStable acrosscultures?PLOSONE.2013;8(5):e62890.
39.KnautLA,MoserADL,MeloSDA,RichardsRR.Translationand culturaladaptationtotheportugueselanguageofthe AmericanShoulderandElbowSurgeonsStandardized Shoulderassessmentform(ASES)forevaluationofshoulder function.RevBrasReumatol.2010;50(2):176–89.
40.JainNB,HigginsLD,LosinaE,CollinsJ,BlazarPE,KatzJN. Epidemiologyofmusculoskeletalupperextremity
ambulatorysurgeryintheUnitedStates.BMCMusculoskelet Disord.2014;15:4.
41.MalavoltaEA,GobbiRG,MancusoFilhoJA,DemangeMK. Análisecríticadaspublicac¸õescientíficasdaRevista BrasileiradeOrtopedianoperíodode2006a2010.RevBras Ortop.2013;48(3):211–5.
42.AmstutzHC,SewHoyAL,ClarkeIC.UCLAanatomictotal shoulderarthroplasty.ClinOrthopRelatRes.1981;(155):7–20.
44.KirkleyA,GriffinS,DaintyK.Scoringsystemsforthe functionalassessmentoftheshoulder.Arthroscopy. 2003;19(10):1109–20.
45.SchmidtS,FerrerM,GonzálezM,GonzálezN,ValderasJM, AlonsoJ,etal.Evaluationofshoulder-specific
patient-reportedoutcomemeasures:asystematicand standardizedcomparisonofavailableevidence.JShoulderElb Surg.2014;23(3):434–44.
46.ConboyVB,MorrisRW,KissJ,CarrAJ.Anevaluationofthe Constant–Murleyshoulderassessment.JBoneJtSurgBr. 1996;78(2):229–32.
47.WaltonMJ,WaltonJC,HonorezLA,HardingVF,WallaceWA.A comparisonofmethodsforshoulderstrengthassessment andanalysisofConstantscorechangeinpatientsagedover fiftyyearsintheUnitedKingdom.JShoulderElbSurg. 2007;16(3):285–9.
48.HirschmannMT,WindB,AmslerF,GrossT.Reliabilityof shoulderabductionstrengthmeasureforthe
Constant–Murleyscore.ClinOrthopRelatRes. 2010;468(6):1565–71.
49.TavakkolizadehA,GhassemiA,Colegate-StoneT,LatifA, SinhaJ.Gender-specificConstantscorecorrectionforage. KneeSurgSportsTraumatolArthrosc.2009;17(5):529–33.
50.FialkaC,OberleitnerG,StampflP,BrannathW,HexelM, VécseiV.ModificationoftheConstant–Murleyshoulder score–introductionoftheindividualrelativeConstantscore. Injury.2005;36(10):1159–65.
51.ConstantCR,GerberC,EmeryRJ,SøjbjergJO,GohlkeF, BoileauP.AreviewoftheConstantscore:modificationsand guidelinesforitsuse.JShoulderElbSurg.2008;17(2):355–61.
52.BlonnaD,ScelsiM,MariniE,BellatoE,TelliniA,RossiR,etal. CanweimprovethereliabilityoftheConstant–Murleyscore? JShoulderElbSurg.2012;21(1):4–12.
53.SugayaH,MaedaK,MatsukiK,MoriishiJ.Functionaland structuraloutcomeafterarthroscopicfull-thicknessrotator cuffrepair:single-rowversusdual-rowfixation.Arthroscopy. 2005;21(11):1307–16.
54.SaccomannoMF,CazzatoG,FodaleM,SircanaG,MilanoG. Magneticresonanceimagingcriteriafortheassessmentof therotatorcuffafterrepair:asystematicreview.KneeSurg SportsTraumatolArthrosc.2015;23(2):423–42.
55.RichardsRR,AnKN,BiglianiLU,FriedmanRJ,GartsmanGM, GristinaAG,etal.Astandardizedmethodfortheassessment ofshoulderfunction.JShoulderElbSurg.1994;3(6):347–52.
56.HirookaA,YonedaM,WakaitaniS,IsakaY,HayashidaK, FukushimaS,etal.AugmentationwithaGore-Texpatchfor repairoflargerotatorcufftearsthatcannotbesutured.J OrthopSci.2002;7(4):451–6.