r e v b r a s o r t o p . 2016;51(4):475–477
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Ulnar
nerve
paralysis
after
forearm
bone
fracture
夽
Carlos
Roberto
Schwartsmann
a,b,∗,
Paulo
Henrique
Ruschel
b,
Rodrigo
Guimarães
Huyer
baUniversidadeFederaldeCiênciasSaúdedePortoAlegre,PortoAlegre,RS,Brazil
bSantaCasadePortoAlegre,Servic¸odeOrtopediaeTraumatologia,PortoAlegre,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19August2015 Accepted22September2015 Availableonline12July2016
Keywords:
Ulnarnerve Forearminjuries Peripheralnerveinjuries
a
b
s
t
r
a
c
t
Paralysisornerveinjuryassociatedwithfracturesofforearmbonesfractureisrareandis morecommoninexposedfractureswithlargesoft-tissueinjuries.Ulnarnerveparalysisis arareconditionassociatedwithclosedfracturesoftheforearm.Inmostcases,thecauseof paralysisisnervecontusion,whichevolveswithneuropraxia.However,nervelacerations andentrapmentatthefracturesitealwaysneedtobeborneinmind.Thisbecomesmore importantwhenneuropraxiaappearsorworsensafterreductionofaclosedfractureofthe forearmhasbeencompleted.Theimportanceofdiagnosingthisinjuryanddifferentiatingits featuresliesinthefactthat,dependingonthetypeoflesion,differenttypesofmanagement willbechosen.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Paralisia
do
nervo
ulnar
seguida
de
fratura
dos
ossos
do
antebrac¸o
Palavras-chave:
Nervoulnar
Traumatismosdoantebrac¸o Traumatismosdosnervos periféricos
r
e
s
u
m
o
Aparalisiaoulesãonervosaassociadaàfraturadosossosdoantebrac¸oérara,émaiscomum nasfraturasexpostascomgrandelesãodepartesmoles.Aparalisiadonervoulnaréuma condic¸ãoincomumassociadaafraturasfechadasdoantebrac¸o.Nagrandemaioriadoscasos, acausadaparalisiaéacontusãodonervo,queevoluicomneuropraxia.Noentanto,devemos sempreestar atentosàslacerac¸õesdonervo eaoencarceramentodonervonofoco de fratura.Issosetornamaisimportantequandoocorreosurgimentodaneuropraxiaoupioria apósafeituradareduc¸ãodafraturafechadadoantebrac¸o.Aimportânciadodiagnóstico dalesãoediferenciarsuascaracterísticasestãonofatodeque,conformeotipodelesão, diferentestiposdemanejoserãoescolhidos.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheSantaCasadePortoAlegre,Servic¸odeOrtopediaeTraumatologia,PortoAlegre,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](C.R.Schwartsmann).
http://dx.doi.org/10.1016/j.rboe.2015.09.017
476
rev bras ortop.2016;51(4):475–477Introduction
Theauthorspresentacaseoffractureofbothbonesofthe forearm associated with neuropraxia in the sensitive area oftheulnarnerve,whichpresentedworseningof neurolog-icalsymptomsafterclosedreductionofthefracture.Simple nerve injuries should be treated conservatively. Additional tests,suchasmagneticresonanceimaging(MRI),canbeused to diagnose the status of the nerve in case of worsening ofneuropraxia.Conversely,surgicalexplorationofthenerve andfracturefixationshouldbedoneincasesof emergenc-ingorworseningneuropraxia,especiallyafterclosedfracture reduction,associatedwithsuspectednervelacerationornerve entrapmentatthefracturesite.Paralysisoftheulnarnerve isanuncommonconditionassociatedwithclosedfractures ofthe forearm.1–3 In mostcases, the cause ofparalysis is
thenerveinjury.Nevertheless,orthopedistsmustalwaysbe watchfulforlacerationsandentrapment.Thisbecomesmore importantincasesofonsetorworseningofneuropraxiaafter aclosedreductionofaforearmfracture.Theimportanceof diagnosingthisinjuryanddifferentiatingitsfeaturesliesin thefactthat,dependingonthetypeoflesion,differenttypes ofmanagementwillbechosen.4,5
Case
report
Amalepatient, 17,presentedtothe emergencyroom with complaintofforearmpainduetoaskateboardingfall, func-tionallimitationoftheupperlimb,and“tingling”ofthefifth finger. Radiological examination indicated fracture of both radiusandulna.Aclosedreductionwasperformed,followed byimmobilizationofthefracture(Figs.1and2).
Post-reduction control radiographs showed satisfactory results.However,thepatientreportedworseningofthe tin-glingsensationinthefifthfingerandworseningofsensitivity. Basedonthesymptoms, ulnarnervelaceration/injuryafter fracturereductionwassuspected.Thus,surgicalexploration
Fig.1–X-rayafterclosedreductionofforearmfracture.
Fig.2–Ulnarnerveentrapment.
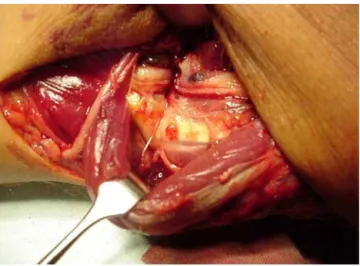
of the nerve was performed, with internal fixation of the forearmfracture.Duringsurgery,aftercarefuldissection,the ulnarnervewasfoundtobeentrappedintheulnarfracture (Figs.3and4).Aftercarefulnervereleaseandmicrosurgical sutureofthelacerationwith8.0nylonsuture,bothfractures werefixatedwithaDCPplateand3.5-mmscrews.
Discussion
Ulnarnerveinjuryisararecomplicationofclosedfracturesof theforearm.Fewcaseshavebeendocumentedandpublished. Therapyrangesfromconservativetreatmentandobservation ofthe neuropraxia tonerve exploration,neurolysis,and/or microsurgicalrepairofinjuries.1,3,5,6Atfirstevaluationinthe
rev bras ortop.2016;51(4):475–477
477
Fig.3–Nerveinjuryafterneurolysis.
Fig.4–Sutureoftheulnarnerve.
contractures.Specificsignsobservedafterfracturereduction canleadtodiagnosis ofpost-reductionneuralentrapment, directing treatment and avoiding paralysis of the affected nerve.2,3,7
A nerve injury should always be suspected after wors-eningofneurologicalsymptomspriortofracturereduction.
Despite satisfactory reduction and the possibility of con-servative treatment if nerve damage is not observed, the managementchanges;orthopedistsshouldbeaggressiveand adoptasurgicalapproachwithsuchpatients.4,6,8Nerve
explo-ration, neurolysis, microsurgical treatment of the injury if necessary,andinternalfixationofthefractureareessentialfor afavorableoutcome,andforcompletereturnoftheforearm andhandfunctionaftertheinjury.2,3
Ulnar nerve injuries associated with closed forearm fracture are uncommon. When they occur, they are usu-ally associated with a contusion, and the treatment is conservative.1Itisimportanttorecognizeanddiagnosethe
etiologyofthelesion.Nerveexplorationandfracturefixation shouldbeperformedupon suspicionofnervelacerationor entrapment, inorder topreventnerve sequelae;additional testsarenotrequiredtoindicatesurgicalprocedure.3,7
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.TorpeyBM,PessGM,KircherMT,FaiermanE,AbsatzMG.Ulnar nervelacerationinaclosedbothboneforearmfracture.J OrthopTrauma.1996;10(2):131–4.
2.PaiVS.Injuryoftheulnarnerveassociatedwithfractureofthe ulna:acasereport.JOrthopSurg(HongKong).1999;7(1): 73–5.
3.AmitB,AshishD,VinitV,RajS,ShivaniB,NarenderM,etal. Missedulnarnerveinjuryandclosedforearmfractureina child.ChinJTraumatol.2013;16(4):246–8.
4.StahlS,RozenN,MichaelsonM.Ulnarnerveinjuryfollowing midshaftforearmfracturesinchildren.JHandSurgBr. 1997;22(6):788–9.
5.HirasawaH,SakaiA,TobaN,KamiuttanaiM,NakamuraT, TanakaK.Bonyentrapmentofulnarnerveafterclosed forearmfracture:acasereport.JOrthopSurg(HongKong). 2004;12(1):122–5.
6.ProsserAJ,HooperG.Entrapmentoftheulnarnerveina greenstickfractureoftheulna.JHandSurgBr.1986;11(2):211–2.
7.SuganumaS,TadaK,HayashiH,SegawaT,TsuchiyaH.Ulnar nervepalsyassociatedwithclosedmidshaftforearmfractures. Orthopedics.2012;35(11):e1680–3.