w w w . r b o . o r g . b r
Original
article
Comparison
of
grafts
for
anatomical
reconstruction
of
the
ACL:
patellar
versus
semitendinosus/gracilis
夽
Patrícia
Barros
Bitun
∗,
Carlos
Roberto
Miranda,
Ricardo
Boso
Escudero,
Marcelo
Araf,
Daphnis
Gonc¸alves
de
Souza
Dr.CarminoCaricchioMunicipalHospital,MunicipalHospitalAdministrativeAuthorityofSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received7September2013 Accepted24October2013 Availableonline14February2015
Keywords:
Reconstructionoftheanterior cruciateligament
Transplants Tendons
a
b
s
t
r
a
c
t
Objective:Tocomparethefunctionalresultsfromsurgicaltreatmentforanatomical recon-structionoftheanteriorcruciateligament(ACL)withasingleband,usingtwotypesof autologousgrafts.
Methods:Twenty-sevenpatientswhounderwentanatomicalreconstructionoftheACLby meansoftheChambattechniquewereevaluatedprospectively.Theyweredividedintotwo groups:A,with14patients,usinggraftsfromflexortendons;andB,with13patients,using graftsfromthepatellartendon.Inbothgroups,fixationwasperformedusinganabsorbable interferencescrew.
Results:BasedontheLysholmscore,groupApresentedameanscoreof71.6inthefirst month,whileBpresented75.Attheendofthesixthmonth,bothgroupspresented96.6. EvaluationofthetotalIKDCshowedthatinthefirstmonth,themajorityofthepatients, bothingroupA(85.7%)andingroupB(76.9%),presentedakneeassessmentthatwasclose tonormal.Inthesixthmonth,92.9%ofgroupAhadnormalpresentations,and100%of groupB.
Conclusion:AccordingtotheLysholmfunctionalevaluationandtheIKDCsubjective assess-ment,therewasnostatisticallysignificantdifferenceintheresultsbetweenthegroups,and theresultswerebetterinthesixthmonth.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedintheDr.CarminoCaricchioMunicipalHospital,MunicipalHospitalAdministrativeAuthorityofSãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](P.B.Bitun). http://dx.doi.org/10.1016/j.rboe.2015.02.004
Comparac¸ão
dos
enxertos
para
reconstruc¸ão
anatômica
do
LCA:
patelar
versus
semitendíneo/grácil
Palavras-chave:
Reconstruc¸ãodoligamento cruzadoanterior
Transplantes Tendões
r
e
s
u
m
o
Objetivo: Comparar o resultado funcional do tratamento cirúrgico da reconstruc¸ão anatômicadoligamentocruzadoanterior(LCA)combandaúnicacomousodedoistipos deenxertoautólogos.
Métodos: Foram avaliadosprospectivamente 27 pacientes, submetidos à reconstruc¸ão anatômicadoLCApelatécnicadeChambat,divididosemdoisgrupos:A,com14euso comoenxertodostendõesflexores;eB,com13eusocomoenxertodotendãopatelar.Em ambososgruposfoifeitafixac¸ãocomparafusodeinterferênciaabsorvível.
Resultados: CombasenoescoredeLysholm,ogrupoAapresentoupontuac¸ãomédiade71,6 noprimeiromês,enquantooBapresentou75.Jánofimdosextomêsambosapresentaram 96,6.Aavaliac¸ãodoIKDCtotalmostrouquenoprimeiromêsamaioriadospacientes,tanto nogrupoA(85,7%)nogrupoB(76,9%),apresentavaumaavaliac¸ãodojoelhopróximodo normalenosextomêsogrupoAapresentou92,9%comonormaleogrupoB,100%.
Conclusão: Osresultados,segundoavaliac¸ãofuncionaldeLysholmesubjetivadoIKDC,não apresentaramdiferenc¸asestatisticamentesignificantesentreosgruposeforammelhores nosextomês.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Surgerytoreconstructtheanteriorcruciateligament(ACL)is frequentlyperformedwithinorthopedicpractice.1
TheACLactsasanessentialstabilizerwithinthe biome-chanicsoftheknee.Inadditiontobeingconsideredtobethe primarystabilizeragainstanteriortranslationofthetibia,it actsasasecondarystabilizeragainstexcessiveinternal rota-tionandvalgusandvarusstress.1
Studieshavealsodemonstratedthatitdiminishesthe pos-sibilityofjointdegeneration,sinceitpromotesprotectionfor thecartilageandmenisci.2
Tearingof this importantligament is common in high-performancesports.Inmakingchangesindirectionorrapid decelerationwith the foot planted onthe ground, individ-ualsmaypromotevalgusstressandstressthroughinternalor externalrotation,therebyinjuringtheligamentwithoutdirect trauma.Oncetheinjuryhasbecomeestablished,thepatient willpresentfrequentepisodesofinstability,pain,edemaand diminishedfunction.Forthisreason,thepossibilityof retur-ningtosports activitieswiththesamevigor and thesame mobilityislow.3
ChoosingthebestautologousgraftforACLreconstruction, inkneeswithinsufficiencyofthisligament,isamatterfor discussion.Graftstakenfromthecentralthirdofthepatellar ligament,asdescribedbyCampbell,4werewidelyusedinthe
1980sand1990s.Attheendofthe1990s,useofthe semitendi-nosusandgracilisflexortendonswasdescribedbyMacey5and
thesegraftsstartedtobeusedmorefrequently.6
TheACLiscomposedoftwobands:posterolateral,which mainlystabilizes rotationalmovements;and anteromedial, which stabilizes movements of anteroposterior transla-tion. Through anatomical studies, a tendency toward ACL
reconstruction usingthe single-band anatomicaltechnique hasbeennoted.7,8
Today, with technological advances, arthroscopic intra-articularreconstructionmakesitpossibletoreduce postop-erative morbidity,9 but divergences between surgeons still
existregardingthebestgrafttouse.
Materials
and
methods
This was a blinded randomized controlled clinical trial. Twenty-seven patientsof bothsexes (25males,92.6%, and two females,7.4%)aged18–48years (mean:31.7)who pre-sented ACLinjurieswereprospectivelyevaluated.Theright sidewasaffectedin19(70.4%)andtheleftsideineight(29.6%). Twelve(44%)presentedlesionsofthemedialmeniscusand onepatient had lesionsofboththe medialand the lateral meniscus.
The inclusion criteriarequired that the patients should present a unilateral ACL tear and the absence of surgical antecedentsorpreviouspathologicalconditionsintheknee affected.
These patients were randomly divided into two groups, throughadrawthatdeterminedthetypeofgraft(patellaror flexor)tobeusedinACLreconstructionsurgery.
GroupA,composedof14patients,underwentACL recon-struction using autologous grafts from the flexor tendons, whilegroupB,with13patients,receivedagraftfromthe patel-lartendon.
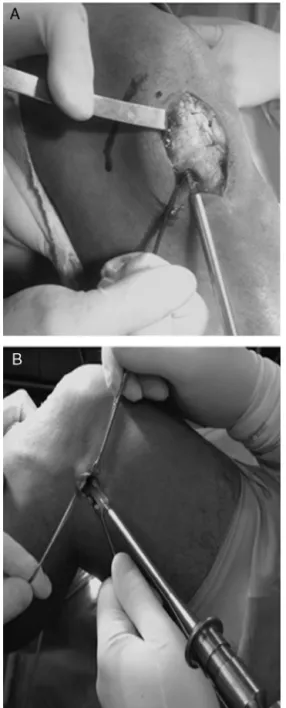
Fig.1–(A)Flexortendon;(B)patellartendon.
Afterthereconstruction,bothgroupswerereferredtothe sameearlyrehabilitationprogram,whichwasconducted indi-viduallybytrainedprofessionals.
All the patients were evaluated atthe outpatient clinic bythesameresearcher,one,threeandsixmonthsafterthe operation.TheInternational KneeDocumentation Commit-tee(IKDC)200010andLysholmprotocolswerefollowed.11The
IKDCiscomposedof10objectivequestions,subdividedinto sevenonsymptoms,twoonsportsactivitiesandoneon func-tionalitybeforeand aftertheinjury. ThemodifiedLysholm scaleiscomposedofeightquestionsinwhichtheoptionsare closedresponses,suchthatthefinalresultisexpressedthus: from95to100pointsas“excellent”;from84to94as“good”; from 65 to83 as “fair”; and 64 orunder as “poor”.11 After
thedata-gathering,thesedataweresubjectedtodescriptive statisticalanalysisusingpercentagefrequencies.
Thestatisticalanalysiswasperformedusingthefollowing software:SPSS®V17,Minitab®16andExcelOffice®2010.The
confidenceinterval(p)of95%wasusedinparametric statis-ticaltests,sincethedatawerequantitativeandcontinuous, andthecentrallimittheoremwasused,whichensured nor-maldistribution.Thus,therewasnoneedtotestthenormality oftheresidualsandparametrictestswereuseddirectly,given thatthesearemorepowerfulthannonparametrictestssuch asANOVAandequalityoftwoproportions.
Surgical
technique
Thetwogroupsdifferedregardingthegrafttobeused(Fig.1), whichwasharvestedfromtherespectivedonorareasusing routineprocedures.Thereconstructionwasdoneusingthe Chambattechniqueandwasthesameforbothgroups.12
Afterarthroscopyandtreatmentofassociatedlesions,the tunnelswereconstructedindependently,frominsideto out-side. By means of a lateral access, 2cm above the lateral epicondyle,aguidewirewasintroducedusingatibialguide adapted for constructing a femoral tunnel, at an angle of 80–90◦ (Figs. 2 and 3), which emerged between the joints,
betweentheoriginsofthetwobands(thefootprints)ofthe lateralcondyleattheanatomicallocationoftheACLonthe femur. Using this guidewire, progressivedrilling witha bit correspondingtothethicknessofthegraftwasperformed.
Thetibialtunnelwasconstructedwiththeremainsofthe ACLonthetibiaasareferencepoint,orinparalleltothe pos-teriormarginoftheanteriorcornuofthe lateralmeniscus,
Fig.2–Guideadaptedforthefemur.
Fig.4–Graftfixationusingabsorbablescrew:(A)tibial fixation;(B)femoralfixation.
withprogressivedrilling.Thegraftwaspassedthroughfrom distallytoproximally,usingtwoEthibond2.0threads.After this,thegraftwasfixedusingabsorbableinterferencescrews inthefemurandtibia,respectively13(Fig.4).
Results
Toanalyzetheresultsfromthegroupsafterthesurgical treat-ment,theparametersfromtheIKDCindexandthefunctional parametersfromtheLysholmscalewereusedinthefirst,third andsixthmonthsaftertheoperation.
TheLysholmfunctionalscalepresentedameanscoreof 71.6outof100ingroupA,inthefirstmonth,whilegroupB
120 100 80 60 40 20 0
1m 3m 6m
96.6 96.6 75
71.6
Group A Group B
Group comparison using lysholm
86.5 89.1
Fig.5–Comparisonbetweenthegroupsaccordingtothe Lysholmscale.
Group comparison using distribution of total IKDC
150%
100%
50%
0%
Group A Group B
1m 3m 6m
A B C A B A B
14.3% 15.4% 85.7% 76.9%
0.0% 7.7%
50.0%
76.9%
50.0%
23.1%
92.9% 100.0%
7.1% 0.0%
Fig.6–Comparisonbetweenthegroupsaccordingtothe totalIKDCscale.
presentedmeanof75.Attheendofthesixthmonth,they presentedthesamemeanscoresof96.6(Fig.5).
TheevaluationusingtheIKDCscaleshowedthatinthefirst month,thekneeassessmentsonthemajorityofthepatients wereclosetonormal,bothingroupA(85.7%)andingroup B(76.9%).Inthesixthmonth,92.9%ofthepatientsingroup Awere assessedasnormaland100%ingroupB.However, statistically,neithertheLysholmnortheIKDCscalepresented anysignificantdifferences,withp>0.05(Fig.6).
Bothgroupspresentedlimitationsregardingtherangeof motioninthefirstmonthaftertheoperation.Inrelationto flexion,14.3%ofthepatientsingroupAand7.7%ingroup Bpresentedlimitations.Inrelationtoextensioninthefirst month,groupAwasalreadyfreefromlimitations,while15.4% of the patientsin groupB presentedlimitations.After the rehabilitationwithphysiotherapy,therewereimprovements among the patients in bothgroups and no joint range-of-motiondeficits were seen inthe sixth month.Statistically, therewerenosignificantdifferencesbetweenthegroups.
FromtheevaluationusingtheIKDCscale,thecriteriaof graftdonorareaandanteriorkneepaindidnotpresentany statistically significant differences at the end of the sixth month,inbothgroups(Figs.7and8).GroupBpresentedtwo casesofhealingthatwasdelayeduntilthethirdmonth.
Inthe evaluationusingtheLachman test,theresultsin groupBwerebetterinthethirdandsixthmonths,with trans-lation of1–2mm in 100%, while in group A, 42.9% of the patientspresentedtranslationof3–5mm(Table1).
Group comparison using distribution of alterations in the graft donor areas
100.0%
84.6%
0.0% 15.4%
92.3%
100.0% 100.0% 100.0%
A
B
A
B A
7.7%
0.0%
3m 6m
m 1
Group A Group B 100%
150%
50%
0%
Fig.7–Comparisonbetweenthegroupsregarding
alterationsinthegraftdonorareas.
Group comparison using distribution of anterior knee pain
7.1% 7.7% m 6 m 3 m 1 100% 50% 0% Group A
A
B
C
A
B
C A
B
Group B
78.6%
69.2%
14.3% 23.1% 28.6%
53.8% 71.4% 38.5% 0.0% 7.7% 78.6% 84.6% 21.4% 15.4%
Fig.8–Comparisonbetweenthegroupsregardinganterior kneepain.
whiletherewasafallto84.6%ingroupB.Attheendofthe sixthmonth,groupBpresentedatendencytowardless ante-riorizationofthetibia(Table2).
Regardingthe ligamentevaluationoverall (i.e.Lachman, “full stop”, anterior drawer, posteriorization of the tibia, medialandlateralopeningandpivotshift),groupsAandB didnotpresentanydifferencesintheirresults,inanyofthe evaluations.
Table1–Comparisonbetweenthegroupsthrough assessmentbymeansoftheLachmantest.
Lachman GroupA GroupB p-Value
N % N %
1m A 11 78.6% 13 100% 0.077
B 3 21.4% 0 0% 0.077
3m A 8 57.1% 13 100% 0.007
B 6 42.9% 0 0% 0.007
6m A 8 57.1% 13 100% 0.007
B 6 42.9% 0 0% 0.007
Table2–Comparisonbetweenthegroupsthrough assessmentbymeansoftheanteriordrawertest.
Anteriordrawer GroupA GroupB p-Value
N % N %
1m A 8 57.1% 13 100% 0.007
B 6 42.9% 0 0% 0.007
3m A 5 35.7% 11 84.6% 0.010
B 9 64.3% 2 15.4% 0.010
6m A 5 35.7% 9 69.2% 0.082
B 9 64.3% 4 30.8% 0.082
Discussion
ACL reconstruction hasbeen widelydiscussed over recent
years.Theseinjuriesoccurfrequently,especiallyintheage groupfrom20to40years.Foralongtime,thepatellar ten-donwaschosenasthemainsourceofgrafts,14butbecauseof
themorbiditiespresented,someauthorshavechosentouse flexortendons.Thishasledtomanycomparativestudies.9
In2001,Erikssonetal.15demonstratedthatusingthe
patel-lartendonproducedaslightadvantageinrelationtostability. On the other hand,in ameta-analysis in2005,Prodromos etal.16showedthatinstabilityandlaxityamonggraftsfrom
theflexortendonsoccurredbecauseofthefixationmethods used,andthatifmethodsthatweremoreeffectivewereused, theresultsweresimilartothoseusinggraftsfromthepatellar tendon.17,18
Inthepresentstudy,itwasdecidedtofixthegraftsfrom thepatellarandflexortendons,bothinthetibialandinthe femoraltunnel,usinganabsorbableinterferencescrew,since thishasbeenshowntopresentexcellentfixationresults,with adequatestiffness.19–22
Inadditiontogoodfixation,theobjectivenowadaysisto achieveanatomicalreconstructionoftheACL,soasto reestab-lishthestructuralandbiomechanicalpropertiesoftheknee,7,8
especiallyinrelationtorotationalinstability.8Recentstudies
havecomparedanatomicACLreconstructionusingadouble bandandasingleband.7,23AccordingtoMisonooetal.,7there
arenostatisticaldifferencesregardingrotationalstability.In thepresentstudy,itwasdecidedtoperformanatomical recon-struction usingasingleband,sincethe techniquepresents lower complexity and lower cost and it facilitatespossible revisions.7
Thepresentstudydidnotpresentanystatistically signif-icantdifferenceincomparativeanalysisbetweengraftsfrom thepatellarandflexortendons,asobservedusingtheLysholm method,whichsubjectivelyevaluateskneefunctionand pro-ducedexcellentresultsattheendofthesixth month.This resulthasalsobeenseeninotherpublishedstudies.9,22,24
Asalsoobservedbyotherauthors,nodifferenceingraft use was observed whenthis was assessed usingthe IKDC scale.24–26
In2003,Janssonetal.27conductedaprospective
random-izedstudyon89patientswhowerefollowedupfor21months, in which they observedthat ACL reconstruction using the patellartendonpresentedlimitationofextensionduringthe firstyearandbecamenormalbytheendofthisperiod. Gold-blattetal.28demonstratedin2005thatpatientsinwhomthe
patellartendonwasusedasagraftpresentedgreater exten-sion deficits (5◦ or more), whilethose in whom the flexor
tendonswereusedpresentedflexiondeficitsof5◦ormore.In
2007,inaprospectivestudy,Laxdaletal.26didnotobserveany
statisticallysignificantdifferenceinrangeofmotionbetween thegroupsstudied,asalsoseeninthepresentstudy.
Some studies have shown thatpatients present greater complaintsofpainintheanteriorregionoftheknee, particu-larlywhenkneelingdown,whenthepatellartendonisusedas agraft.9,25,27InastudybyVasconcelosetal.,25amongpatients
otherstudieshavereportedthattherewasnostatistical dif-ferenceinkneepainbetweenthegraftsused,15,18inthesame
wayasseenintheresultsfromthepresentstudy.
Overall,theligamentevaluationsinkneesthatunderwent ACLreconstructiondidnotshowany statisticaldifferences between the groups observed, either in our study or in others.15,27,29 Usingthe anteriordrawertestaloneto
evalu-atethereconstructedtendon,itwasobservedoverthefirst threepostoperativemonthsthattheanteriortranslationofthe tibiaatflexionof90◦wasgreaterinthegroupinwhichflexor
tendonswereused.Aftersixmonthsofevaluation,therewas nodifferencebetweenthegroups.22IntheLachmantest,
bet-terresultswereobservedinthethirdandsixthmonthsafter theoperation,inthepatientsinwhomtheligament recon-structionwasperformedusingthepatellartendon.Thisresult differedfromwhatwasobservedinthestudybyPinczewski etal.,24inwhichnodifferencebetweenthegroupsafter10
yearsoffollow-up.
Thepresentstudycanbecriticizedintermsofthesmall numberofpatientsselected(n=27),theshortlengthof follow-up,the greaterproportionofmalepatients, theabsence of statisticalevaluation on associatedlesions and the lackof arthrometerforgreaterprecisionofevaluationonthe recon-structedligament.
Conclusion
AccordingtotheLysholmfunctionalevaluationandtheIKDC subjectiveassessment,therewasno statisticallysignificant differenceintheresultsbetweenthegroups.Itissuggested thatinfuturestudies,associatedlesionsshouldbeevaluated, withlongerfollow-upanduseofanarthrometerfor assess-mentsofgreaterprecision.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. FukubayashiT,TorzilliPA,ShermanMF,WarrenRF.An invitrobiomechanicalevaluationofanterior–posterior motionoftheknee.Tibialdisplacement,rotation,andtorque. JBoneJointSurgAm.1982;64(2):258–64.
2. BusfieldBT,SafranMR,CannonWD.Extensormechanism disruptionaftercontralateralmiddlethirdpatellartendon harvestforanteriorcruciateligamentrevision
reconstruction.Arthroscopy.2005;21(10):1268.
3. LymanS,KoulouvarisP,ShermanS,DoH,MandlLA,MarxRG. Epidemiologyofanteriorcruciateligamentreconstruction: trends,readmissions,andsubsequentkneesurgery.JBone JointSurgAm.2009;91(10):2321–8.
4. CampbellWC.Reconstructionoftheligamentsoftheknee. AmJSurg.1939;43:473–80.
5. MaceyBH.Anewoperativeprocedureforrepairofruptured cruciateligamentsofthekneejoint.SurgGynecolObstet. 1939;69:108–9.
6. KopfS,MartinDE,TashmanS,FuFH.Effectoftibialdrill anglesonbonetunnelapertureduringanteriorcruciate
ligamentreconstruction.JBoneJointSurgAm. 2010;92(4):871–81.
7.MisonooG,KanamoriA,IdaH,MiyakawaS,OchiaiN. Evaluationoftibialrotationalstabilityofsingle-bundlevs. anatomicaldouble-bundleanteriorcruciateligament reconstructionduringahigh-demandactivity–a quasi-randomizedtrial.Knee.2012;19(2):87–93. 8.SteinerM.Anatomicsingle-bundleACLreconstruction.
SportsMedArthrosc.2009;17(4):247–51.
9.ShaiebMD,KanDM,ChangSK,MarumotoJM,RichardsonAB. Aprospectiverandomizedcomparisonofpatellartendon versussemitendinosousandgracilistendonautograftsfor anteriorcruciateligamentreconstruction.AmJSportsMed. 2002;30(2):214–20.
10.MetsavahtL,LeporaceG,RibertoM,deMelloSpositoMM, BatistaLA.Translationandcross-culturaladaptationofthe BrazilianversionoftheInternationalKneeDocumentation CommitteeSubjectiveKneeForm:validityand
reproducibility.AmJSportsMed.2010;38(9):1894–9.
11.PeccinMS,CiconelliR,CohenM.Questionárioespecíficopara sintomasdojoelhoLysholmKneeScoringScale:traduc¸ãoe validac¸ãoparaalínguaportuguesa.ActaOrtopBras. 2006;14(5):268–72.
12.GarofaloR,MouhsineE,ChambatP,SiegristO.Anatomic anteriorcruciateligamentreconstruction:thetwo-incision technique.KneeSurgSportsTraumatolArthrosc.
2006;14(6):510–6.
13.HarilainenA,LinkoE,SandelinJ.Randomizedprospective studyofACLreconstructionwithinterferencescrewfixation inpatellartendonautograftsversusfemoralmetalplate suspensionandtibialpostfixationinhamstringtendon autografts:5-yearclinicalandradiologicalfollow-upresults. KneeSurgSportsTraumatolArthrosc.2006;14(6):
517–28.
14.ShelbourneKD,GrayT.Resultsofanteriorcruciateligament reconstructionbasedonmeniscusandarticularcartilage statusatthetimeofsurgery.Five-tofifteen-yearevaluations. AmJSportsMed.2000;28(4):446–52.
15.ErikssonK,AnderbergP,HambergP,LöfgrenAC,Bredenberg M,WestmanI,etal.Acomparisonofquadruple
semitendinosusandpatellartendongraftsinreconstruction oftheanteriorcruciateligament.JBoneJointSurgBr. 2001;83(3):348–54.
16.ProdromosCC,JoyceBT,ShiK,KellerBL.Ameta-analysisof stabilityafteranteriorcruciateligamentreconstructionasa functionofhamstringversuspatellartendongraftand fixationtype.Arthroscopy.2005;21(10):1202.
17.MilanoG,MulasPD,ZiranuF,PirasS,ManuntaA,Fabbriciani C.Comparisonbetweendifferentfemoralfixationdevicesfor ACLreconstructionwithdoubledhamstringtendongraft:a biomechanicalanalysis.Arthroscopy.2006;22(6):660–8. 18.BiauDJ,TournouxC,KatsahianS,SchranzPJ,NizardRS.
Bone-patellartendon-boneautograftsversushamstring autograftsforreconstructionofanteriorcruciateligament: meta-analysis.BMJ.2006;332(7548):995–1001.
19.KousaP,JärvinenTL,KannusP,JärvinenM.Initialfixation strengthofbioabsorbableandtitaniuminterferencescrewsin anteriorcruciateligamentreconstruction.Biomechanical evaluationbysinglecycleandcyclicloading.AmJSports Med.2001;29(4):420–5.
20.RadfordMJ,NoakesJ,ReadJ,WoodDG.Thenaturalhistoryof abioabsorbableinterferencescrewusedforanteriorcruciate ligamentreconstructionwitha4-strandhamstring
technique.Arthroscopy.2005;21(6):707–10.
21.BrandJCJr,NylandJ,CabornDN,JohnsonDL.Soft-tissue interferencefixation:bioabsorbablescrewversusmetal screw.Arthroscopy.2005;21(8):911–6.
22.MaletisGB,CameronSL,TenganJJ,BurchetteRJ.A
reconstruction:acomparisonofpatellartendonand quadruple-strandsemitendinosus/gracilistendonsfixedwith bioabsorbableinterferencescrews.AmJSportsMed. 2007;35(3):384–94.
23.FerrettiA,MonacoE,LabiancaL,DeCarliA,MaestriB, ConteducaF.Double-bundleanteriorcruciateligament reconstruction:acomprehensivekinematicstudyusing navigation.AmJSportsMed.2009;37(8):
1548–53.
24.PinczewskiLA,LymanJ,SalmonLJ,RussellVJ,RoeJ,Linklater J.A10-yearcomparisonofanteriorcruciateligament reconstructionswithhamstringtendonandpatellartendon autograft:acontrolled,prospectivetrial.AmJSportsMed. 2007;35(4):564–74.
25.VasconcelosW,SantosC,FerraciniAM,DejourD.Influenceof anteriorpainonresultsfromanteriorcruciateligament reconstruction.RevBrasOrtop.2011;46(1):40–4.
26.LaxdalG,SernertN,EjerhedL,KarlssonJ,KartusJT.A prospectivecomparisonofbone-patellartendon-boneand hamstringtendongraftsforanteriorcruciateligament reconstructioninmalepatients.KneeSurgSportsTraumatol Arthrosc.2007;15(2):115–25.
27.JanssonKA,LinkoE,SandelinJ,HarilainenA.Aprospective randomizedstudyofpatellarversushamstringtendon autograftsforanteriorcruciateligamentreconstruction.AmJ SportsMed.2003;31(1):12–8.
28.GoldblattJP,FitzsimmonsSE,BalkE,RichmondJC. Reconstructionoftheanteriorcruciateligament:
meta-analysisofpatellartendonversushamstringtendon autograft.Arthroscopy.2005;21(7):791–803.