SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Is
the
size
of
the
acetabular
bone
lesion
a
predictive
factor
for
failure
in
revisions
of
total
hip
arthroplasty
using
an
impacted
allograft?
夽
Rodrigo
Pereira
Guimarães
∗,
Alexandre
Maris
Yonamine,
Carlos
Eduardo
Nunes
Faria,
Marco
Rudelli
FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,DepartamentodeOrtopediaeTraumatologia,GrupodoQuadril,SãoPaulo, SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12August2015 Accepted25September2015 Availableonline27June2016
Keywords: Hiparthroplasty Bonetransplantation Acetabulum Allografts
a
b
s
t
r
a
c
t
Objective:Theaimofthisstudywastodeterminetheacetabularbonelesionsize(in mil-limeters)fromwhichimpactedbonegraftfailurestartstooccurmorefrequently,through simpleanteroposteriorhipradiographs,andwhethermeasurementofthedefectonsimple radiographsmaintainsthesamepatternininterandintraobserverassessments.
Methods:Thirty-eight anteroposterior pelvic-viewradiographsfrompatientsundergoing revisionofanacetabularprosthesiswereretrospectivelyanalyzedandassessed.Inthe ver-ticalplane,thebilacrimallinewasmeasuredinmillimetersfromthefarthestpointfound ontheboneedgeoftheacetabularosteolysistothetopedgeofthecementationorofthe acetabularimplantinuncementedcases.Thebasewastakentobealineperpendicularto bilacrimalline,withtheaimofeliminatinganypelvictilteffects.Thismeasurementwas namedtheverticalsizeoffailure.Radiographsproducedfouryearsaftertheoperationwere analyzedtoinvestigateanyfailureofthetechnique.
Results:Thegraftfailurerateinthestudygroupwas26.3%.Thefailuresoccurredincases withaninitialbonedefectlargerthan11mm.Nocaseswithmeasurementssmallerthan thisevolvedwithfailureoftherevision.Thehighestincidenceofgraftfailureoccurredin casesdescribedasadvancedaccordingtothe“Paprosky”classification.
Conclusion:Failure of acetabular revisionarthroplasty using an impacted graft did not presentanystatisticallysignificant correlationwiththeverticalextentofthelesionon simpleanteroposteriorradiographs,asapredictoroftreatmentfailure.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheFaculdadedeCiênciasMédicasdaSantaCasadeMisericórdiadeSãoPaulo,DepartamentodeOrtopediae Traumatologia,GrupodoQuadril,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.P.Guimarães). http://dx.doi.org/10.1016/j.rboe.2015.09.015
O
tamanho
da
lesão
óssea
acetabular
é
fator
preditivo
para
a
falha
nas
revisões
de
artroplastia
total
do
quadril
com
enxerto
impactado?
Palavras-chave: Artroplastiadequadril Transplanteósseo Acetábulo Aloenxertos
r
e
s
u
m
o
Objetivo: Opresentetrabalhobuscou,atravésdeumaradiografiasimplesanteroposterior doquadril,quantificaremmilímetrosapartirdequaltamanhodalesãoósseaacetabular ocorrecommaiorfrequênciafalhadoenxertoósseoimpactadoeseamedic¸ãododefeito nasradiografiassimplesmantémomesmopadrãonaavaliac¸ãointereintraobservador. Métodos: Foramanalisadaseaferidasretrospectivamente38radiografiasdepacientes sub-metidosàrevisãodepróteseacetabularnaincidênciaanteroposteriordebacia,mensurando emmilímetros,noplanoverticalalinhabilacrimal,amedidaentreopontomaisdistante encontradonabordaósseadaosteoliseacetabular,comamargemsuperiordacimentac¸ão ouimplanteacetabularnoscasosnãocimentados.Tomamoscomobaseumalinha perpen-dicularalinhabilacrimalcomointuitodeeliminarefeitosdeinclinac¸ãopelvic.Essamedida foidenominadaTamanhoVerticaldaFalha.Radiografiaspós-operatóriascomquatroanos foramanalisadasparaaveriguarfalhadatécnica.
Resultados: Nogrupoestudadoobservamos26,3%defalhasdoenxertoqueocorrerama partirde11mmdetamanhodafalhaósseainicialmensuradaequeabaixodessevalor nenhumcasoevoluiucomfalhadarevisão.Amaiorincidênciadafalhadoenxertoocorreu noscasosavanc¸adossegundoaclassificac¸ãodePaprosky.
Conclusão: Afalhanaartroplastiaderevisãoacetabularcomenxertoimpactadoquando relacionadoàmedidaverticaldalesãoemradiografiasimplesanteroposteriordoquadril nãoapresentousignificânciaestatísticacomofatorpreditivodefalhadotratamento.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The consolidation of contemporary total hip arthroplasty techniqueshasresultedinanincreaseintheuseofthis pro-cedure.Therefore,theneedforrevisionsurgeryhasbecomea morecommonproblem.1
The restoration of the anatomy and biomechanics improvesdurabilityandfunctionoftherevisedhip.Themost challengingaspectofacetabularrevisionistocompensatefor acetabularbonelossandcreateastablereconstruction,with goodlongtermdurability.2
Various techniques are described to rebuild extensive acetabular defects, including structural grafts or impacted graftchips,reinforcementringswithcages,placementofthe acetabularcomponentinahighhipcenter,jumboacetabular cups,bilobedacetabularcups,triflangecups,andtrabecular metalacetabularaugments.2
Although more modern prosthesis revision techniques areavailable,associatedwithnewimplants,thisprocedure remainsachallenge,evenformoreexperiencedsurgeons.3
Thelooseningofcementedorcementlesscomponentsin totalhiparthroplastyisalwaysaccompaniedbylossofbone stock.Sloofetal.4proposedtheuseofimpactedbonegraftin
revisionsofthiscomponentwhenbonelosswassignificant. Acetabularreconstructionwithimpactedbonegraftanda cementedcupisareliabletechnique,withaten-yearsurvival rateof 88% inpatients withextensive acetabulardefects.2
BonelosscanbedeterminedbytheclassificationofPaprosky etal.,5whichprovidesasimplealgorithmtodeterminebone
defectand directtreatmentforrevisionintotalhip arthro-plasty.
Brownetal.,6 inastudythatusedthePaprosky
classifi-cation,demonstratedaninterobserverreliabilityof0.61.This indicatesasubstantialagreementamongsurgeons.The intra-observerreliabilityforeachofthefoursurgeonsinthatstudy was 0.81, 0.78, 0.76, and 0.75, which indicates substantial agreement.
Thisstudyaimedtoassesswhetheracetabularboneloss, measuredinasimpleanteroposteriorradiographofthepelvis, isapredictivefactorforfailureintherevisiontechniquewith impactedbonegraft,andwhether themeasurementofthe defectinplainradiographsmaintainsthesame patternfor inter-andintraobserverassessments.
Material
and
methods
This study was approved by the Research Ethics Commit-tee,underCAEENo.07779812.6.0000.5479.Postoperativepelvic radiographs of 38 patients undergoing revision surgeryfor total hip arthroplastieswere assessed;these patientswere operatedonbythreeexperiencedhipsurgeonsbetween1995 and2008.
Line A (bilacrimal)
Line B
Point C
Point D
Fig.1–HipX-rayinanteroposteriorincidenceshowing
measurementofthesizeofbonedefectinmillimetersin
theverticalplane;thismeasurementcorrespondstothe
greatestdistancebetweentheedgeoftheacetabularlesion
(pointC)andtheacetabularroofinitsanatomicalposition
(pointD).
publishedstandardsbythehipgroup:patientinthesupineor standingposition;rayincidenceonthemedianline, imme-diately above the pubic symphysis, feet internally rotated at15–20◦whenpossible(forcorrectionoftheneck antever-sion angle),so that the greater trochanter didnot overlap thefemoralneck;and thecoccyx shouldbevisualizedand alignedwiththepubicsymphysis,withacranialdistanceof 2.5cminfemalesand1.5cminmales.Theobturatorforamen shouldbesymmetrical.7Allradiographsstudiedwere
analogi-cal,withmagnificationof100%.Casesofsepticlooseningwere excluded.
AftertheselectionofX-rays,theacetabularcomponentof theprosthesiswasanalyzedandthebonelosspriortothe reviewwasclassifiedusingthePaproskymethod.Thebone defectwasmeasuredinmillimeters.Themeasurementwas madebythreeorthopedists:eachmadetwoassessments,with anintervalofoneweek.
Bonelosswasmeasuredasfollows:inthehipradiography inanteroposteriorincidence,thebilacrimallinewasdrawn (lineA).Next,lineBwasdrawnperpendiculartolineA,ina paththatincludedmostoftheacetabularfailuretobestudied, andtwopointswereset(CandD).PointCcorrespondedto theupperedgeoftheacetabularfailure,andpointD,tothe topedgeoftheacetabularcementoroftheacetabularcup incementlesscases. ThedistancebetweenpointsC andD wasmeasuredinmillimetersandtermedverticalsizeofthe acetabularfailure(Fig.1).
Subsequently, radiographs were analyzed after a mean of 48 months follow-up and it was determined whether or notloosening ofthe revised acetabularcomponent had taken place. Treatment failurewas defined asa change of theacetabularcomponentposition,steepening,ormigration higherthan2mmwhencomparingX-rayintheimmediate postoperativeperiodwithafinal radiograph.8 Furthermore,
thepresenceofsolid radiolucentlineslargerthan 2mmor
progressionofradiolucentlinesaroundtheacetabulumalso characterizedtreatmentfailure.9
The reliability ofthe inter- and intraobserver measure-ment wasindicatedbytheintraclasscorrelationcoefficient (ICC).Nextstepconsistedincomparingwhetherornotthe implant loosened withthe sizeofacetabularfailure, using theMann–Whitneynon-parametricmethod.Inaddition,the samemethodwasusedtocomparefailurevs.ageandfailure vs.gender.Inallstatisticaltests,a5%significancelevelwas adopted.Todeterminewhetherthemethodusedwasa pre-dictivefactorforfailureoftheproposedtreatment,anROC curvewasused.
Results
Forthepresentstudy,38patients(38hips)wereselected:mean ageof60.5years(range29–87years),23females(60.5%)and15 males(39.5%).Ofthese,13hadinvolvementontherightside (34.2%)and25ontheleftside(65.8%).
According tothePaproskyclassification,twohips (5.3%) wereclassifiedastype1;nine(23.7%)as2A;eight(21.1%)as 2B;six(15.8%)as2C;ten(26.3%)as3A;andthree(7.9%)as3B. Regarding thetypeofsurgerythesepatientsunderwent, 33werefirstrevisionarthroplasties(86.8%),fourweresecond revisionarthroplasties(10.5%),andonewasathirdrevision arthroplasty(2.6%).Theprimarycauseofarthroplastieswas alsoanalyzed:14hipshadprimaryosteoarthritis(36.8%),eight had inflammatorydisease(21.1%),sixhadtraumasequelae (15.8%),fivehadmalformation(13.2%),andfivehadavascular necrosisofthefemoralhead(13.2%).
Failureintheproposedtreatmentwasobservedintenhips (26.3%):threefailureswereobservedintheavascularnecrosis ofthefemoralheadgroup(30%),threeintheinflammatory diseasesgroup(30%),twointheprimaryosteoarthritisgroup (20%),andtwointhehipmalformationgroup(20%).
Failureintheproposedtreatmentwas relatedtogender andsidewithinthetenpatientswithfailureafterreview,six ofwhomweremale(60%ofthefailures)andfourfemale(40% ofthefailures);threeontherightside(34.2%ofthefailures) andsevenontheleft(65.8%ofthefailures).
Therelationshipoflooseningormigrationofthe acetabu-larcomponentwiththePaproskyclassificationindicatedthat therewere nofailuresinhips classifiedasPaprosky1,two failuresinhipsclassifiedas2A(20%),nofailuresinthose clas-sifiedas2B,twofailuresinthoseclassifiedas2C(20%),sixin thoseclassifiedas3A(60%),andnofailuresinthoseclassified as3B.
Failureoftheproposedtreatmentwascomparedwiththe typeofsurgerythatthesepatientshadundergone:eight fail-ures (80%) were observed in patients who underwent first revisionarthroplasty,onefailure(10%)inapatientwho under-wentsecondrevisionarthroplasty,andone(10%)inthesingle patientwhounderwentthirdrevisionarthroplasty.
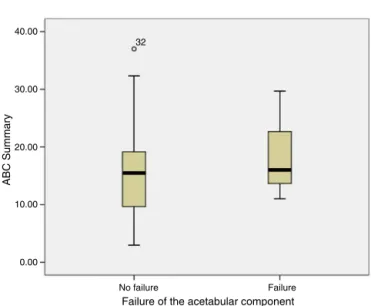
Thesizeoftheinitialbonelesionrangedfrom3to37mm; inthisstudy,patientswhosebonelesionsweresmallerthan 11mm did not present failure of the proposed treatment (Fig.2).
40.00
32
30.00
20.00
10.00
0.00
Failure No failure
Failure of the acetabular component
ABC Summary
Fig.2–Boxplotcomparingfailureoftheacetabular
componentvs.sizeofinitialbonelesion.
40
32
12
32 32
30
20
10
0
Exc_mm Exb_mm
Exa_mm
Fig.3–Boxplotcomparingmeasurementsperformedby
evaluatorsvs.sizeoftheinitialboneinjury.
inter-observeragreement(ICC>0.70)betweenthe measure-mentsoftheverticalsizeofthefailure,demonstratingthe reliabilityofthemethod(Fig.3).
Discussion
Acetabular bone deficiency may be caused by wear, loos-ening, infection,bonelossatthe time ofprevioussurgery, pre-existing fracture, acetabular dysplasia, or even bone destructionduringremovalofthecomponentorcement.All thesefactorsleadtobonedeficiency,whichhinderstreatment. Totalhiparthroplastyrevisionsareoftenassociatedwith lossofacetabularbonestock.4Intheliterature,thereare
var-ioustreatmentsto managethis problem, but none isfully effective.Treatmentaimstoprovidestabilityoftheimplant andrestorethejointcenterofrotation.10
Theselesionscanbetreatedwithbonegraftingorlarger prostheses, according to the techniques described in the
literature.2,11 Thebone grafts used for revision
arthroplas-ties have been an important object of study for some authors,1–4,11–14withgrowingexpectationsofsolvinga
prob-lemthathasnodefinitivesolutionyet.
Thehomograftusedforacetabularreconstructioncanbe dividedintotwogroups:blockgraftandgraftchips.Theuseof blockgraftiscontroversial10,11andusuallyrestrictedtocases
withextendedacetabularfailure.12,13Theuseofthisgraftto
fillthebonedefecthasbeenlinkedtoearlyfailureduetograft absorptionand fracture,especiallywhenusedasasupport system.14
In recent studies, Hooten et al.15,16 have shown that
althoughradiographicallytheautologousgraftappearstobe integratedandabsorptionareasarenotobserved,therefore indicatinganapparentstabilityoftheacetabularcomponent, postmortemhistologicalexamsrevealedvascularizationonly onthe surfaceofthe graftincontactwithhostbone.Only peripheralintegrationwasobserved,tonomorethan2mm, making thegraftanavascularmasswithoutany chanceof integration.
Theliteratureshowsthatgraftfailureratesincreasewhen usingstructuredgraftstosupportareaslargerthan50%ofthe acetabularcomponentsurface.15However,aspreviously
men-tioned,themainindicationforblockgraftsarebonedefects ofgreatermagnitude,inwhichover50%ofthesurfaceofthe acetabularcupissupportedbyfreshbonegraft.15
Inarecentstudy,Bilgen etal.3 concludedthathavingat
least50%contactbetweentheacetabularcup andthehost boneisnotabsolutelynecessaryforastableconstruction.
JastyandHarris17,18foundnodifferencesbetweentheuse
ofautograftorhomograft,consideringbothformsofgraftto havesimilarefficacyforacetabularboneloss.
Sloofetal.4proposedtheuseofimpactedgraftchips;their
techniquehasgained wideacceptanceand isusedin vari-ousservices.Theirstudyusedimpactedbonegraftchipsand obtained90%goodresultsinameanfollow-upof11.8years.
Buttaro et al.19 assessed23 revisions, appliedthe same
techniquewithfrozengraft chipswithameanfollow-upof 35.8 months, and obtained 90.8% good results.In a recent study,Combaetal.20evaluated30cases,alsowithfrozengraft
chips,withameanfollow-upof86.5monthsand86%good results.
Buckley et al.21 analyzed 123 acetabularrevision
proce-duresusinggraftchipswithameanof60months,achieving 86%goodresults.Theintegrationofimpactedgraftchipshas alreadybeenreportedinstudieswithhistologicalanalysis.20
Theimpactedgraftchipstechniquewasappliedinallpatients inthepresentstudy.
vanHaarenetal.22reportedahighfailurerateof28%at7.8
yearsoffollow-up,withtheuseofimpactedgraftsfordifferent magnitudesofacetabularfailure,includingpelvic discontinu-ity. However,theydidnotquantitativelyestablish towhich magnitudesofbonedefectimpactedgraftingiscorrectly indi-cated.
Inthepresentsample,similarresultswereobserved,with a26.3%incidenceofgraftfailureat48monthsfollow-upwith thetechniquepresentedfordifferenttypesofboneinjury.
Garcia-Cimbreloetal.23evaluatedtheacetabulargraft
ROC curve
Specificity
-1 Specificity
-1
Sensitivity Sensitivity
1.0
0.8
0.6
0.4
0.2
0.0
1.0
0.8
0.6
0.4
0.2
0.0 1.0 0.8 0.6 0.4 0.2
0.0 0.0 0.2 0.4 0.6 0.8 1.0
ROC curve
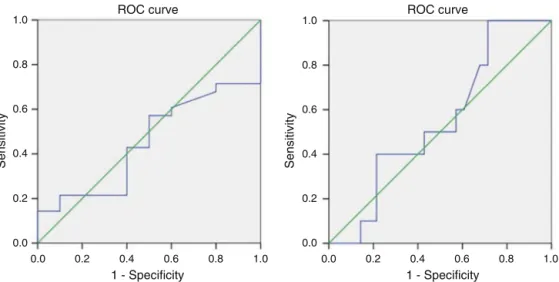
Fig.4–ROCcurveshowingabsenceofstatisticalsignificanceinmeasurementoftheverticalsizeofthelesionvs.revision
failure.
initialboneloss; theyacknowledged the needforcages or platesinlargerlesions.However,thismagnitudewasalsonot quantified.Thepresentstudydidnotadoptseriouslesionsas anexclusioncriterion,preciselytoaddressthelackof infor-mationontheacceptabledegreeofacetabularbonestockloss forimpactedbonegraft.
El-Kawyetal.24evaluated28patientsclassifiedasPaprosky
type3andfound96.4%goodresultsat72monthsoffollow-up. In the present study,the samplewas not largeenough tostatisticallycorrelatethePaproskyratingwith the num-ber of failures observed. The analysis of the ROC curve (Fig.4)shows that the verticalsizeofthe lesion isnot an implant failurepredictor (p>0.05). However,inasubjective analysisof the data, no revisionfailures were observed in lesionswithinitialverticalsizelowerthan11mm.Themain challenge inthis study wassurely tofind the best way to assessthemagnitudeofthislesionwithonlyanteroposterior X-rays.
Somelimitationsofthisstudyarenoteworthy.First,some studieshaveshownthesuperiorityofCTinrelationtoX-ray tomeasureacetabularpreoperativeboneloss.25,26 However,
asthepresentanalysiswasretrospective,from1995to2008, thevastmajorityofpatientshadnodocumentedtomographic images.Thus, theanalysisofhip X-raysinanteroposterior incidencewasthemethodchosen.
Anotherlimitationofthestudywastheuseofasimple X-raytomeasureacavity.Itisknownthattheacetabularlesion isathree-dimensionalconditionandthatitsprecise measure-mentinonlyoneradiograph isnotpossible.However,this studyaimedtoevaluatethepossibilityofaquickandeasy study,whichcouldbedoneintheoffice,topredictapossible failure,aswellastoassesswhetherthemeasurementofthe verticalsizeofthelesiononsimpleradiographswassimilar intheinter-andintraobserverevaluation.
Inthiscase,astheradiographicevaluationpresenteda con-sistentinter-andintraobserveragreement,theauthorsbelieve thattheresultswerenotcompromised.
Finally, authors believe that studies with larger sample sizes are needed to better define the correlation of the
failureinthistypeoftreatmentwiththesizeofthe preop-erativebonelesionmeasuredinsimpleradiographs.
Conclusion
Failure in revision acetabular arthroplasty using impacted graftdidnotpresentastatisticallysignificantassociationwith variablesdescribedinthepresentstudy,demonstratingthat themeasureoffailureinananteroposteriorradiograph can-notbeusedinisolationasapredictivefactorforfailureofthe acetabularrevision,whichisconfirmedbylackofsignificance intheROCcurve.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Theauthorswouldliketothankthesurgeons:Prof.Dr. Gian-carlo Cavalli Polesello, Dr Walter Ricioli Junior, Dr Marcelo CavalheirodeQueiroz,Prof.DrEmersonKiyoshiHonda,and Prof. Dr Nelson Keiske Ono, for performing surgeries and follow-upofpatientsanalyzedinthisstudy.
r
e
f
e
r
e
n
c
e
s
1.RudelliS,HondaE,ViriatoSP,LibanoG,LeiteLF.Acetabular revisionwithbonegraftandcementlesscup.JArthroplast. 2009;24(3):432–43.
2.vanEgmondN,DeKamDC,GardeniersJW,SchreursBW. Revisionsofextensiveacetabulardefectswithimpaction graftingandacementcup.ClinOrthopRelatRes. 2011;469(2):562–73.
4. SlooffTJ,BumaP,SchreursBW,SchimmelJW,HuiskesR, GardeniersJ.Acetabularandfemoralreconstructionwith impactedgraftandcement.ClinOrthopRelatRes. 1996;324:108–15.
5. PaproskyWG,PeronaPG,LawrenceJM.Acetabulardefect classificationandsurgicalreconstructioninrevision arthroplasty.A6-yearfollow-upevaluation.JArthroplast. 1994;9(1):33–44.
6. BrownNM,ForanJR,ValleCJ,MoricM,SporerSM,LevineBR, etal.Theinter-observerandintra-observerreliabilityofthe Paproskyfemoralbonelossclassificationsystem.J Arthroplast.2014;29(7):1482–4.
7. PoleselloGC,NakaoTS,QueirozMC,DaniachiD,RicioliJunior W,GuimarãesRP,etal.Propostadepadronizac¸ãodoestudo radiográficodoquadriledapelve.RevBrasOrtop.
2011;46(6):634–42.
8. CallaghanJJ,SalvatiEA,PellicciPM,WilsonPDJr,RanawatCS. Resultsofrevisionformechanicalfailureaftercementedtotal hipreplacement,1979to1982.Atwotofive-yearfollow-up.J BoneJointSurgAm.1985;67(7):1074–85.
9. DeLeeJG,CharnleyJ.Radiologicaldemarcationofcemented socketsintotalhipreplacement.ClinOrthopRelatRes. 1976;121:20–32.
10.CucklerJM.Managementstrategiesforacetabulardefectsin revisiontotalhiparthroplasty.JArthroplast.2002;174Suppl. 1:153–6.
11.ReesHW,FungDA,CerynikDL,AminNH,JohansonNA. Revisiontotalhiparthroplastywithoutbonegraftof high-gradeacetabulardefects.JArthroplast.2012;27(1):41–7. 12.MallNA,NunleyRM,SmithKE,MaloneyWJ,ClohisyJC,
BarrackRL.Thefateofgraftingacetabulardefectsduring revisiontotalhiparthroplasty.ClinOrthopRelatRes. 2010;468(12):3286–94.
13.LeopoldSS,JacobsJJ,RosenbergAG.Cancellousallograftin revisiontotalhiparthroplasty.Aclinicalreview.ClinOrthop RelatRes.2000;371:86–97.
14.BrubakerSM,BrownTE,ManaswiA,MihalkoWM,CuiQ, SalehKJ.Treatmentoptionsandallograftuseinrevisiontotal hiparthroplastytheacetabulum.JArthroplast.2007;227 Suppl.3:52–6.
15.HootenJPJr,EnghCAJr,EnghCA.Failureofstructural acetabularallograftsincementlessrevisionhiparthroplasty.J BoneJointSurgBr.1994;76(3):419–22.
16.HootenJPJr,EnghCA,HeekinRD,VinhTN.Structuralbulk allograftsinacetabularreconstruction.Analysisoftwografts retrievedatpost-mortem.JBoneJointSurgBr.
1996;78(2):270–5.
17.JastyM,HarrisWH.Totalhipreconstructionusingfrozen femoralheadallograftsinpatientswithacetabularboneloss. OrthopClinNAm.1987;18(2):291–9.
18.JastyM,HarrisWH.Salvagetotalhipreconstructionin patientswithmajoracetabularbonedeficiencyusing structuralfemoralheadallografts.JBoneJointSurgBr. 1990;72(1):63–7.
19.ButtaroMA,CombaF,PussoR,PiccalugaF.Acetabular revisionwithmetalmesh,impactionbonegrafting,anda cementedcup.ClinOrthopRelatRes.2008;466(10):2482–90. 20.CombaF,ButtaroM,PussoR,PiccalugaF.Acetabularrevision
surgerywithimpactedboneallograftsandcementedcupsin patientsyoungerthan55years.IntOrthop.2009;33(3):611–6. 21.BuckleySC,StockleyI,HamerAJ,KerryRM.Irradiated
allograftboneforacetabularrevisionsurgery.Resultsata meanoffiveyears.JBoneJointSurgBr.2005;87(3):310–3. 22.vanHaarenEH,HeyligersIC,AlexanderFG,WuismanPI.High
rateoffailureofimpactiongraftinginlargeacetabular defects.JBoneJointSurgBr.2007;89(3):296–300. 23.Garcia-CimbreloE,Cruz-PardosA,Garcia-ReyE,
Ortega-ChamarroJ.Thesurvivalandfateofacetabular reconstructionwithimpactiongraftingforlargedefects.Clin OrthopRelatRes.2010;468(12):3304–13.
24.El-KawyS,HayD,DrabuK.Clinicalandradiologicalbone allografttechniqueresultsofimpactioninacetabular revisionsassociatedwithmassivebonestockdeficiencies: fourtosevenyearsfollow-upstudy.HipInt.2005;15:46–51. 25.LeungS,NaudieD,KitamuraN,WaldeT,EnghCA.Computed
tomographyintheassessmentofperiacetabularosteolysis.J BoneJointSurgAm.2005;87(3):592–7.