w w w . r b o . o r g . b r
Original
Article
Surgical
treatment
for
myelodysplastic
clubfoot
夽
,
夽夽
Alexandre
Zuccon
∗,
Sérgio
Inácio
Cristiano
Cardoso,
Fábio
Peluzo
Abreu,
Antonio
Carlos
Fernandes
Associac¸ãodeAssistênciaàCrianc¸aDeficiente(AACD),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19July2013 Accepted29October2013 Availableonline22October2014
Keywords:
Myelomeningocele Clubfoot
Acquireddeformitiesofthefoot
a
b
s
t
r
a
c
t
Objective:To analyze the results from surgical treatment of69 casesof clubfoot in43 patientswithmyelodysplasiaaccordingtoclinicalandradiographiccriteria,atour insti-tutionbetween1984and2004.
Methods:Thiswasa retrospectivestudy involvinganalysisofmedicalfiles,radiographs andconsultationsrelatingtopatientswhounderwentsurgicalcorrectionofclubfoot.The surgicaltechniqueconsistedofradicalposteromedialandlateralreleasewithorwithout associatedtalectomy.
Results:Thepatients’meanageatthetimeofthesurgerywasfouryearsandtwomonths, andthemeanlengthofpostoperativefollow-upwassevenyearsandtwomonths. Sat-isfactoryresults wereachievedin73.9%ofthefeetandunsatisfactoryresults in26.1% (p<0.0001).
Conclusion: Residualdeformityintheimmediatepostoperativeperiodwasassociatedwith unsatisfactoryresults.OpeningoftheKite(talocalcaneal)angleinfeetthatonly under-wentposteromedialandlateralrelease,alongwithappropriatepositioningofthecalcaneus incasesthatunderwenttalectomy,wastheradiographicparameterthatcorrelatedwith satisfactoryresults.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Tratamento
cirúrgico
do
pé
equinovaro
mielodisplásico
Palavras-chave:
Mielomeningocele Pétorto
Deformidadesadquiridasdopé
r
e
s
u
m
o
Objetivo:Analisarosresultadosentre1984e2004emnossainstituic¸ãodotratamento cirúr-gico de 69 pésequinovaros em 43 pacientes portadores de mielodisplasia segundo os critériosclínicoeradiográfico.
Métodos:Estudo retrospectivo com análise de prontuário, radiografias e consulta com pacientesportadoresdemielomeningocelequeforamsubmetidosacorrec¸ãocirúrgicade pésequinovaros.Atécnicacirúrgicafoialiberac¸ãoposteromediolateral(LPML)radical asso-ciadaounãoatalectomia.
夽
Pleasecitethisarticleas:ZucconA,CardosoSIC,AbreuFP,FernandesAC.Tratamentocirúrgicodopéequinovaromielodisplásico.Rev BrasOrtop.2014;49:653–660.
夽夽
WorkdevelopedattheAssociationforDisabledChildren’sCare(AACD),SãoPaulo,SP,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](A.Zuccon). http://dx.doi.org/10.1016/j.rboe.2014.10.006
Resultados: Amédiadeidadenaépocada cirurgiafoidequatroanosedoismeseseo seguimentomédiopós-operatório,deseteanosedoismeses.Foramencontradosresultados satisfatóriosem73,9%dospéseinsatisfatóriosem26,1%(p<0,0001).
Conclusão: Adeformidaderesidualnopós-operatórioimediatoestárelacionadacom result-adosinsatisfatórioseaaberturadoângulodeKite(talocalcaneano)nospéssubmetidos somenteaLPML,alémdoposicionamentoadequadodocalcâneo,noscasosemquefoi feitaatalectomia,éoparâmetroradiográficorelacionadoaosresultadossatisfatórios.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Thereareseveralformsofpresentationofneuraltubeclosure defects,suchasmyelomeningocele,myelocele,meningocele andlipomeningocele.Theseconditionshavethecommon fea-tureofdeficientfusionofposteriorelementsofthespine,in associationwithmedullarydysplasia.1
Theworldwideincidenceofmyelomeningoceleis1:1000 livebirths,onaverage.1
Medullarydysplasia,ormyelodysplasia,mayoccurto vary-ingdegreesandmaycompromisevariousorgansandsystems, suchasthemusculoskeletal,genitourinary,digestiveand neu-rologicalsystems.Hydrocephalyoccursduringthecourseof 90%ofmyelomeningocelecases.1,2
Theinnervationofthelowerlimbsiscompromisedandthis givesrisetomotorandsensoryparalysis,muscleimbalance anddeformities.
Thefeet are frequentlyaffected bydeformitiesin these cases.3–6Inastudyconductedinthemyelomeningoceleclinic
ofour hospital,the mostprevalent deformity was equino-varus,whichwasobservedin31%ofthe480feetthatwere evaluatedrandomly.1
Myelodysplasticequinovarusfootisoneofthemost fre-quent abnormalities. It is difficult to treat and has high complicationrates.3–5
Conservativetreatmentofmyelodysplasticfeetusingserial plaster casts in accordance with the Ponseti method has increasedinpopularityamongpediatricorthopedists. How-ever, so far, there is still no scientific evidence regarding long-termmaintenanceofthecorrectionachievedand there-foresurgicaltreatmentisstillused.1,7–9Intheliterature,there
arereportsonproceduresgoingfromsoft-tissuereleasewith tendonstretchingtobonesurgeryofamoreaggressivenature, suchastalectomy.3,10–13
Theobjective ofthe present study was to evaluatethe resultsfrom surgical treatmentofmyelodysplastic equino-varusfeetatourinstitutionfromOctober1984toOctober2004 andtocorrelatethedeformities,surgicaltechniqueusedand resultsobtained.
Material
and
method
Aretrospective study was conducted,withanalysis onthe medicalfilesofpatientspresentingmyelodysplasticclubfoot. Subsequently,patientswhounderwentsurgicaltreatmenton
theirfeet atourservicebetweenOctober1984andOctober 2004, asshown inourdatabase, were invited toreturnfor clinicalassessment.
Noclassificationregardingtheseverityofthedeformities wasmade.
Theinclusioncriteriawerethatthepatientsneededtohave hadthefollowing:(1)myelodysplasiawithequinovarusfeet from thetimeofbirththathadnotbeen treatedsurgically priortothetreatmentatourinstitutionand(2)aminimum postoperativefollow-upoftwoyears.
Patientswhowewereunabletocontact,thosewhosedata wereinsufficientandthosewhodidnotcomeforclinical eval-uationwereexcluded.
The surgical technique used was posteromedial lateral release(PMLR),withorwithoutassociatedtalectomy.Insome feet, shorteningofthe lateral columnwasalso performed. Twoaccessincisionsused(oneposteromedialandtheother, lateral) andtheCincinnatiroute wasusedinfeet that pre-sentedequinus≤30◦(24.6%).Tenotomywasperformedwith
resection of around 2cm of the tendons ofthe calcaneus, longflexorofthehallux,commonflexorofthetoes,posterior andanteriortibialisand abductorofthehallux. Posterome-diallateralcapsulotomyofthetibiotarsalandsubtalarjoints wasthenperformed,includingtheinterosseous, talonavicu-lar,calcaneocuboid,naviculocuneiformandcuneometatarsal ligaments.Whenreductionofthedeformityofthehindfoot throughtheseprocedureswasnotpossible,orwhenthetalus wasverydeformed,talectomywaschosen.Incasesinwhich deformityinadductionpersistedaftertheprocedures, short-eningofthelateralcolumnwasalsoperformed(36feet).The location wasat the level ofthe cuboid in 33 casesand at thelevelofthecalcaneocuboidinthreecases.Fixationwith Kirschnerwireswasperformedaftercorrectionofthe defor-mity, with placement ofa retrograde wire inthe hindfoot (calcaneus-talus-tibia),awireinthemedialcolumntokeep themedialjointsopenandanotherwireinthelateralcolumn toclosethejointsinthiscolumn.Thewireswerethreaded, becauseuponperformingthereleaseandthecapsulotomies and reducing thedeforming, therewasa needtokeepthe jointsinthemedialregionopen.
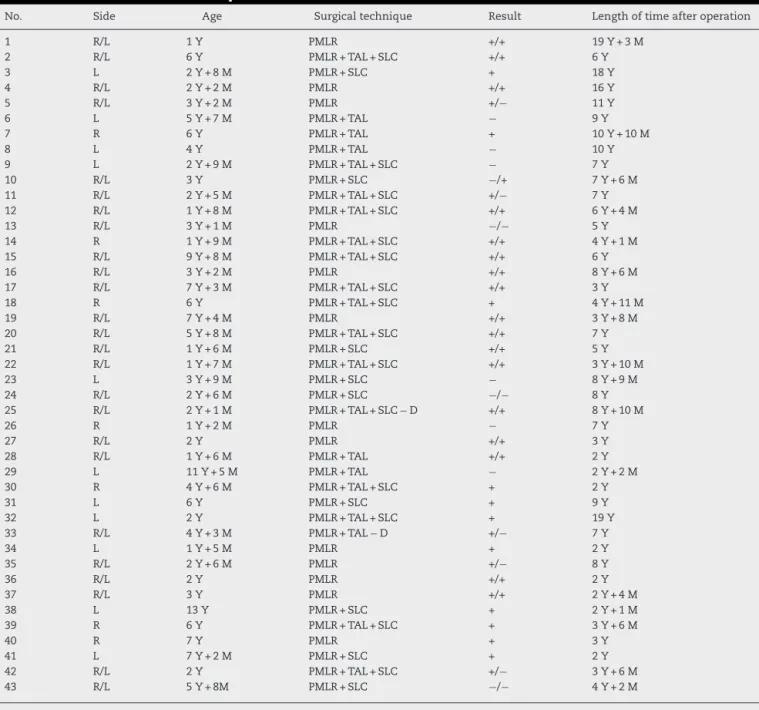
Table1–Generaldistributionofthepatients.
No. Side Age Surgicaltechnique Result Lengthoftimeafteroperation
1 R/L 1Y PMLR +/+ 19Y+3M
2 R/L 6Y PMLR+TAL+SLC +/+ 6Y
3 L 2Y+8M PMLR+SLC + 18Y
4 R/L 2Y+2M PMLR +/+ 16Y
5 R/L 3Y+2M PMLR +/− 11Y
6 L 5Y+7M PMLR+TAL − 9Y
7 R 6Y PMLR+TAL + 10Y+10M
8 L 4Y PMLR+TAL − 10Y
9 L 2Y+9M PMLR+TAL+SLC − 7Y
10 R/L 3Y PMLR+SLC −/+ 7Y+6M
11 R/L 2Y+5M PMLR+TAL+SLC +/− 7Y
12 R/L 1Y+8M PMLR+TAL+SLC +/+ 6Y+4M
13 R/L 3Y+1M PMLR −/− 5Y
14 R 1Y+9M PMLR+TAL+SLC +/+ 4Y+1M
15 R/L 9Y+8M PMLR+TAL+SLC +/+ 6Y
16 R/L 3Y+2M PMLR +/+ 8Y+6M
17 R/L 7Y+3M PMLR+TAL+SLC +/+ 3Y
18 R 6Y PMLR+TAL+SLC + 4Y+11M
19 R/L 7Y+4M PMLR +/+ 3Y+8M
20 R/L 5Y+8M PMLR+TAL+SLC +/+ 7Y
21 R/L 1Y+6M PMLR+SLC +/+ 5Y
22 R/L 1Y+7M PMLR+TAL+SLC +/+ 3Y+10M
23 L 3Y+9M PMLR+SLC − 8Y+9M
24 R/L 2Y+6M PMLR+SLC −/− 8Y
25 R/L 2Y+1M PMLR+TAL+SLC−D +/+ 8Y+10M
26 R 1Y+2M PMLR − 7Y
27 R/L 2Y PMLR +/+ 3Y
28 R/L 1Y+6M PMLR+TAL +/+ 2Y
29 L 11Y+5M PMLR+TAL − 2Y+2M
30 R 4Y+6M PMLR+TAL+SLC + 2Y
31 L 6Y PMLR+SLC + 9Y
32 L 2Y PMLR+TAL+SLC + 19Y
33 R/L 4Y+3M PMLR+TAL−D +/− 7Y
34 L 1Y+5M PMLR + 2Y
35 R/L 2Y+6M PMLR +/− 8Y
36 R/L 2Y PMLR +/+ 2Y
37 R/L 3Y PMLR +/+ 2Y+4M
38 L 13Y PMLR+SLC + 2Y+1M
39 R 6Y PMLR+TAL+SLC + 3Y+6M
40 R 7Y PMLR + 3Y
41 L 7Y+2M PMLR+SLC + 2Y
42 R/L 2Y PMLR+TAL+SLC +/− 3Y+6M
43 R/L 5Y+8M PMLR+SLC −/− 4Y+2M
Results:(+),satisfactory;(−),unsatisfactory;SLC,shorteningoflateralcolumn;TAL,talectomy.
Thecaseswereanalyzedusingclinicalandradiographic criteria. According to the clinical criteria, we divided the resultsintosatisfactoryandunsatisfactory,ascanbeseenin thefollowing:
• Satisfactory result–feetthatpresentedthecriterialisted
below:
1. Plantigradefeet;
2. Feetcompatiblewithuseofabraceintheneutral posi-tion;
3. Feetwithoutskinlesionsorpressureulcers.
• Unsatisfactoryresult–atleastoneofthefollowingcriteria:
1. Non-plantigradefeet;
2. Feetincompatiblewithuseofabraceintheneutral posi-tion;
3. Feetwithskinlesions(ulcers)duetopressure;
4. Feetrequiringsubsequentsurgicalprocedures.
Thepatientsweregroupedaccordingtonumericalorder, initials oftheirname,sideofthebody affected,ageatthe timeofthesurgery,surgicaltechniqueused,resultobtained andlengthofpostoperativefollow-up(Table1).
We evaluated the immediate complications (those that occurredduringtheimmediatepostoperativeperiodorupto twoweeksafterthesurgicalprocedure)andthelate compli-cations(morethantwoweeksafterthesurgery),withregard tofrequencyandtype.
(giventhatthismeasurementwouldbeimpossibleincases oftalectomy).Thisanglemeasurestheopeningbetweenthe talusandcalcaneusandnormalvaluesarebetween20◦and
40◦.Itisgreatlyusedintheliteratureforevaluatingtalipes
equinovarusandfrequentlyisdiminished(<20◦)incasesof
thisdeformity.5 Wealsoanalyzedthepositionofthe
calca-neusinthefeetthatunderwenttalectomyandconsideredthe radiographicresulttobeacceptablewhenthecalcaneuswas positionedbelowthetibia,inaneutralpositionandslightly posteriorizedinrelationtoit,andifnoresidualfragmentof thetaluswasidentifiedbetweenthecalcaneusandthetibia.
Our initial hypothesis was that if the deformities were notcompletelycorrectedthroughthesurgicalprocedure,i.e. iftherewas someresidualdeformityafterthe surgery,the chanceofobtaininganunsatisfactoryresultwouldbegreater. Toassess whethertheresidual deformitywasrelatedto theresults,weusedtheFisherexacttest.Situationsof sat-isfactoryresultswiththe presenceofresidualdeformityor unsatisfactoryresultswithoutresidualdeformityweretaken tobediscordant.
Statistical values from the radiographic analyses were obtainedusingtheMcNemartest.
Inall cases,therejectionlevelforthenullityhypothesis wassetatavalue≤0.05(5%).
Whenthestatisticscalculatedpresentedsignificance,we used an asterisk (*) to denote this. If otherwise, i.e. non-significant,weusedtheabbreviationNS.
Results
Weanalyzed90 medicalfilesand attemptedtocontactthe individualsconcernedbymeansofthetelephone,inorderto invitethemforclinicalassessmentandfinalradiography.Out ofthese90patients,weobtaineddataonandattendanceby 43.
Weincluded69feet(43patients)inthestudy.Thus, defor-mities in both feet were observed in 26 patients (60.4%). Regarding gender, there were slightly more females: 22 patients(51.1%).
Thepatients’meanageatthetimeofthesurgerywasfour yearsandtwomonths.Theminimumagewasoneyearand themaximumwas13years.
Theminimumpostoperativelengthoffollow-upwastwo yearsandthemaximumwas19yearsandthreemonths.The meanwassevenyearsandtwomonths.
Outofthe69feetevaluated,wefoundthattheresultwas satisfactoryin51(73.9%)andunsatisfactoryin18(26.1%),in accordance withtheclinical criteriastated inthe methods section(p<0.0001).
In31feet(44.9%),posteromediallateral releasewas per-formed in association with talectomy, whilein 38 (55.1%), posteromediallateralreleasealonewasperformed.
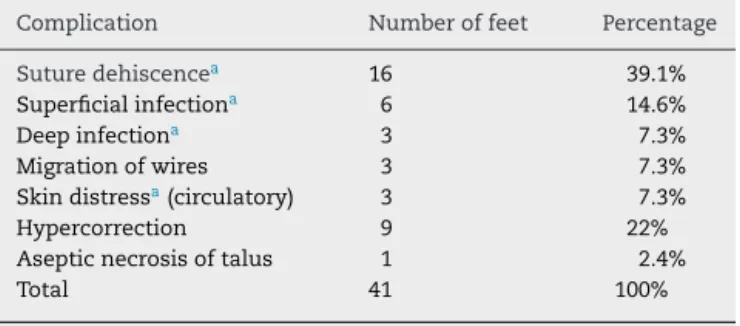
Immediate (I)and late (T) complicationswere observed in34feet(49.2%).Suturedehiscence(16feet)occurredmost frequently and, later on, hypercorrection showing valgus deformity(ninefeet)(Table2).
– Partialortotalrecurrenceoccurredin12feet(17.4%ofthe cases).
Table2–Frequenciesofpostoperativecomplications.
Complication Numberoffeet Percentage
Suturedehiscencea 16 39.1%
Superficialinfectiona 6 14.6%
Deepinfectiona 3 7.3%
Migrationofwires 3 7.3%
Skindistressa(circulatory) 3 7.3%
Hypercorrection 9 22%
Asepticnecrosisoftalus 1 2.4%
Total 41 100%
a Note:Insevenfeet,morethanonecomplicationoccurred.
– Reoperationwasperformedon12feet(17.4%).
Inanalyzingthefeetthatpresentedresidualdeformity,i.e. which presenteddeformity intheimmediatepostoperative period(ninefeet),weidentifiedunsatisfactoryresultsineight cases(88.9%). When weanalyzedthefeet without residual deformities(60),weidentifiedsatisfactoryresultsin50(83.3%) andunsatisfactoryresultsinonly10(16.7%)(Table3).
Weobservedrecurrenceofthedeformityin12feet.Eight (66.6%)hadresidualdeformityintheimmediatepostoperative periodandfour(33.3%)didnotpresentthis.
Regardingtheradiographicevaluation,weobtained com-pletedocumentationfor45feetand,amongthese,wefound that thepreoperativeAPKite anglewasclosed(<20◦)in41
(91.1%).InthefeetthatunderwentPMLRforwhich satisfac-toryresultswereobtained(22),theKiteangleincreasedin21 cases(95.4%),whileinthefeetwithunsatisfactoryresultsthat underwent PMLR(six),the Kiteangleincreasedinonlyone (16.6%)(Table4).InthefeetthatunderwentPMLR+talectomy forwhichsatisfactoryresultswereobtained(15),14(93.3%) presentedcorrectpositioningofthecalcaneusandonlyone didnot.Ontheotherhand,amongthefeetthatunderwent
Table3–Relationshipbetweentheresultsandresidual deformity.
Result Residualdeformity
Present Absent Total
Unsatisfactory 8feet* 10feet 18feet
Satisfactory 1foot 50feet 51feet
Total 9feet 60feet 69feet
∗ p=0.00004(Fishertest).
Table4–RelationshipbetweenpostoperativeKiteangle andfinalresult.
Result Kite
Open Closed Total
Satisfactory 21feet 1foot 22feet
Unsatisfactory 1foot 5feet 6feet
Total 22feet 6feet 28feet
Table5–Relationshipbetweenthepositionofthe calcaneusandthefinalresult.
Result Radiography
Position+ Position− Total
Satisfactory 14 1 15
Unsatisfactory 1 1 2
Total 15 2 17
p=0.7500NS.Concordance=88.23%(McNemartest). Position+:correctpositionforcalcaneus.
Position−:incorrectpositionforcalcaneus.
PMLR+talectomywithunsatisfactoryresults(two),one pre-sentedcorrectpositioningofthecalcaneusandone,incorrect positioning(Table5).
Discussion
Equinovarusdeformityoffeetincasesofmyelodysplasiais difficult to manage, with high rates of complications and recurrenceduetothespecificcharacteristicsofthis patholog-icalcondition, whichpresentsparalysis,muscleimbalance, insensitivityandstiffness.3–5,8
Thepreferredtreatmentforthisdeformityhashistorically beensurgical.Thus,thetechniqueusedisimportant,because itmayinfluencethefinalresult.7
Althoughconservative treatmentfor casesofidiopathic clubfootiswellestablishedintheliterature,thistreatment isstillnotcompletelyreproducibleandtherearestillno long-termstudiesrelatingtomyelodysplasticfeet.
Morestudiesandclinicaltrialsusingplaster-casttreatment arenowappearing,especiallyusingtheprinciplesofthe Pon-setimethodforcorrectionofthesedeformities.However,the recurrenceratesinnon-idiopathicfeetarestillhigh.14In
ana-lyzingoursample,particularlywithregardtoageatthetime ofthetreatment,thechoiceofsurgicaltreatmentwasmore viable.
Thepatients’ ageatthe timeofthe surgerywasa deci-sivefactor,giventhattheirmeanageasfouryearsandtwo months.Thisisanadvancedagefortreatingthispathological condition, giventhat the feetalready present greater stiff-ness,alterationstotheboneformatandjointincongruence (Figs.1and2).
Theincisionsusedinsurgicaltreatmentsforclubfootvary widely.Turcodescribedastraightincision fromthebaseof thefirstmetatarsaltotheAchillestendon,without subcuta-neousdissection.15Crawfordetal.describedtheincisionthat
hadbeenconceptualizedbyGiannestrasandisknownasthe Cincinnatirouteinhomagetotheplacewheretheyworked.16
Inthisstudy,adoubleroutewasused(oneposteromedialand theother,lateral)inthegreatmajorityofthepatientsandthe Cincinnatiroutewasusedinthefeetthatpresentedan equi-nuscomponentoflessthan30◦;inthismanner,therewasno
difficultyinclosingtheskin.
Someauthorshaveemphasizedtheimportanceofusing an appropriatesurgical technique, withthe use oftendon resectionratherthansimplestretching,andthiswasalsoour
Fig.1–Patientwithmyelodysplasia,presentingstiff clubfootbeforeoperationconsistingofPMLR+talectomy.
preference.1,4,12Throughdoingthis,werebalancedtheforces
actingonthefootandavoidedrecurrence.
Posteromediallateralreleaseisdonetotreatclubfootand broadcapsulotomyisimportant,alongwithtendonrelease withresection,asalreadymentioned.2,3
Another pointcitedintheliteratureiscorrectionofthe rotationofthetalus.12Inourstudy,therewasanincreasein
theKiteangleinalltheradiographicallydocumentedfeetthat evolvedsatisfactorilyandwhichdidnotundergotalectomy, whichindicatestheimportanceofthistechnicaldetail.
Talectomy is a procedure that has been performed for a long time in orthopedic practice, with reports dating back to1608,from Fabricus.10 Many authors havereported
good resultsfrom this technique for surgicaltreatment of myelodysplasticequinovarusfoot.6,7,10,17,18
Someauthorshavehighlightedtheimportanceofcorrect positioningofthecalcaneusintalectomizedcases.Wealso believe that a poorly positioned calcaneus may lead toan unsatisfactoryresult,althoughwedidnotprovethis statis-ticallyinpourstudy,probablybecauseofthesmallsample size.13,19
Fig.2–Patientwiththeabilitytowalkwithinthecommunity,withmyelodysplasticclubfootwithalesioninthe dorsolateralskin(theweight-bearingareaofthisfoot).
ofthemidfootandforefoot.Therefore,itdoesnotprovidefull correctionofthedeformitiesandincreasesthepossibilityof recurrence.
Thesurgicalcorrectionofthedeformitieswasstartedin thehindfootbymeansoftendonandcapsulereleases(PMLR). Whenthesewereinsufficientforcompletecorrectionofthe deformityofthehindfoot,talectomywasperformed. Adduc-tion deformities of the forefoot were corrected by means of capsule and ligament release. When these procedures wereinsufficientforfullcorrection,shorteningofthelateral columnwasused. Therefore, intraoperativeevaluationand knowledgeofthepathologicalanatomyofthedeformitiesis extremelyimportant,sincethesurgicalproceduresare per-formedonlyasrequired.20
Thirty-onecasesunderwentposteromediallateralrelease inassociationwithtalectomyand38withouttalectomy,and 36ofthesefeet(52.1%)underwentshorteningofthelateral column.Wefoundarateofsatisfactoryresultssimilartothat oftheliteraturethroughtheseprocedures.
Figs. 3 and 4 show illustrative cases of the corrections achievedthroughthesurgicalprocedures.
Complicationsintreatingthisdeformityfrequentlyoccur, asalreadyhighlightedbyotherauthors.1,3,5,8Duringthe
post-operativefollow-up, complicationsoccurred in49.2%ofthe cases,ascanbeseeninChart2.
Valgusdeformitywasoneofthemainlong-term compli-cationsand we attribute this to the wide-ranging releases thatwereperformed,includingofthesubtalarinterosseous ligament. There is controversy regarding whether release of this ligament should be performed, even if only partially.21,22
Itwasnotourobjectivetoevaluatefunctionallevel, defor-mities in other segments of the body or gait prognosis, althoughthereisastudyintheliteraturethatcorrelated defor-mityinkneeflexionandsurgicalcorrectionofclubfootamong patientswithmyelodysplasiaandarthrogryposis.7
Table3showsthat,accordingtotheFisherexacttest,the calculatedstatisticalp-valuewas0.0004*andthatthe resid-ual deformitiespresent onlyappeared infrequentlyamong thesatisfactoryresults.Thus,presenceofresidual deformi-tiescorrelatedwithhigherratesofunsatisfactoryresults.This observationisextremelyimportantbecauseattheendofthe surgicalprocedure,ifanydeformitiesstillremaintobe cor-rected,theseshouldnotbeneglectedorelsetheremightbea riskofpoorresults.
Ourstudypresentsseverallimitations,startingwithits ret-rospectivecaseseriesdesign.
Itwasnotpossibletouseaseverityclassificationforthe feetthatweretreatedbecauseofinsufficientdatainthe med-icalfiles.However,fromthehighrateoftalectomyprocedures performed,itcanbeinferredthatdifficultyincorrectingthese feetwasencountered.
Anotherlimitationwasthattherewasnocorrelationwith thesepatients’functionallevel,giventhatpatientswhowere abletowalkmightbemorelikelytohaveunsatisfactoryresults becauseofthegreaterlikelihoodofskinlesionsthroughthe bodyweightborneonafootwithresidualdeformity,evenif thisweremild.
Fig.3–SamepatientasinFig.1,aftertheoperationonthestiffclubfootconsistingofPMLR+talectomy.
Fig.4–PatientwithmyelodysplasticfeetwhounderwentsurgicalcorrectionbymeansofPMLRattheageofninemonths. Goodevolution,withtheabilitytowalkwithinthecommunity,presentingplantigradefeetcompatiblewithbracersand withoutscars.Preoperativesituation(pre-op),secondyearaftertheoperationand17thyearaftertheoperation.
patientswithmyelodysplasiaandthatthesurgicalprocedure isextensive.Duringtheoperation,ifproceduressuchas talec-tomyandshorteningofthelateralcolumnbecomenecessary, theseshouldbeperformedduringthesameoperation,soas nottoleave residual deformitiesand thus todiminishthe possibilityofrecurrence.
Conclusion
Thesurgical treatment instituted in these myelodysplastic feetofpatientsfollowedupatourinstitutionwaseffectivein correctingthedeformities,withresultssimilartothosefound intheliterature.
– Postoperativecomplicationsoccurfrequently.
– Residualdeformityafterthesurgicalprocedureisafactor contributingtowardlackofsuccessintreatingthesefeet andthereforeshouldbeavoided.
– When posteromediallateralreleaseisperformedwithout talectomy,itseemstobeimportanttoopenupthe talocal-canealangle.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.FernandesAC.Malformac¸õesdotuboneural.In:HebertS, XavierR,PardiniJúniorAG,BarrosFilhoTEP(org.).Ortopedia etraumatologia:príncipioseprática.3rded.PortoAlegre: Artmed;2003.p.839–57.
2.MazurJM.Managementoffootandankledeformitiesinthe ambulatorychildwithmyelomeningocele.In:SarwakJF, editor.Caringforthechildwithspinabifida.OakBrook: AmericanAcademyofOrthopaedicSurgeon;2002. p.155–60.
3.SharrardWJ,GrosfieldI.Themanagementofdeformityand paralysisofthefootinmyelomeningocele.JBoneJointSurg Br.1968;50(3):456–65.
4.LindsethRE.Myelomeningocele.In:WoodW,LovellRB, WinterRT,editors.Morrissy:LovellandWinter’spediatric orthopaedics.4thed.Philadelphia:LippincottWilliams& Wilkins;1996.p.527–9.
5.TachdjianMO.Mielomeningocele.In:TachdjianMO,editor. Ortopediapediátrica.Traduc¸ãoAnaPaulaTedescoGabrieli. SãoPaulo:Manole;1995.p.1953–5.
6.FrischhutB,StöcklB,LandauerF,KrismerM,MenardiG.Foot deformitiesinadolescentsandyoungadultswithspina bifida.JPediatrOrthopB.2000;9(3):161–9.
7.SvartmanC,FucsPM,KertzmanPF,NishiRK,SoniJF, HaguiaraWJ.Talectomianotratamentodasdeformidades rígidasdospésnaartrogriposeesequelade
mielomeningocele.RevBrasOrtop.1993;28(4):453–7. 8.MenelausMB.Talectomyforequinovarusdeformityin
9. MenelausMB.Legandfootdeformities.In:MenelausMB, editor.Theorthopaedicsmanagementofspinabifidacystic. NewYork:Churchill-Livingstone;1980.p.92–104.
10.CooperRR,CapelloW.Talectomy.Along-termfollow-up evaluation.ClinOrthopRelatRes.1985;(201):32–5. 11.HsuLC,JaffrayD,LeongJC.Talectomyforclubfootin
arthrogryposis.JBoneJointSurgBr.1984;66(5):694–6. 12.CarvalhoNetoJ,DiasLS,GabrieliAP.Congenitaltalipes
equinovarusinspinabifida:treatmentandresults.JPediatr Orthop.1996;16(6):782–5.
13.DiasLS,SternLS.Talectomyinthetreatmentofresistant talipesequinovarusdeformityinmyelomeningoceleand arthrogryposis.JPediatrOrthop.1987;7(1):39–41.
14.GerlachDJ,GurnettCA,LimpaphayomN,AlaeeF,ZhangZ, PorterK,etal.EarlyresultsofthePonsetimethodforthe treatmentofclubfootassociatedwithmyelomeningocele.J BoneJointSurgAm.2009;91(6):1350–9.
15.TurcoVJ.Surgicalcorrectionoftheresistantclubfoot. One-stageposteromedialreleasewithinternalfixation:a preliminaryreport.JBoneJointSurgAm.1971;53(3):477–97. 16.CrawfordAH,MarxenJL,OsterfeldDL.TheCincinnati
incision:acomprehensiveapproachforsurgicalprocedures
ofthefootandankleinchildhood.JBoneJointSurgAm. 1982;64(9):1355–8.
17.SherkHH,AmesMD.Talectomyinthetreatmentofthe myelomeningocelepatient.ClinOrthopRelatRes. 1975;(110):218–22.
18.LegaspiJ,LiYH,ChowW,LeongJC.Talectomyinpatients withrecurrentdeformityinclubfoot.Along-termfollow-up study.JBoneJointSurgBr.2001;83(3):384–7.
19.SalomãoO,CarvalhoJuniorAE,FernandesTD,MarquesJ, IamuraM,FreitasRB.Astragalectomianotratamentodepés equinovaroscongênitos(PTC)inveteradoserecidivados.Rev BrasOrtop.1993;28(7):449–52.
20.SodréH,MestrinerLA,PintoJA,Lourenc¸oAF,AdamesMK. Tratamentocirúrgicodopétortoequinovarocongênito idiopático.Avaliac¸ãopós-operatóriade164pés.RevBras Ortop.1997;32(1):21–6.
21.AtarD,LehmanWB,GrantAD.Revisionsurgeryinclubfeet. ClinOrthopRelatRes.1982;(283):223–30.