Correspondência: Rua João Moura 627, cj 23 - Jardim América São Paulo - SP CEP: 05412-911
Summary
Objective. This study analyzed the relationship between clinical characteristics of endometriosis and Th1/Th2 immune response patterns.
MethOds. A prospective study was performed with 65 patients with endometriosis (Group A) and 33 without the disease (Group B). Measurement of IL 2, 4 and 10, TNF-alpha and IFN-gamma was carried out in peripheral blood and peritoneal luid.
Results. Serum TNF-alpha was higher in patients with endometriosis who had deep dyspareunia compared to controls (mean 4.5 pg/ml and 2.3 pg/ml, p<0.05). Among these patients (n=32), 65.5% had deep endometriosis. Patients with endometriosis and infertility had higher IL-2 concentrations in peritoneal luid than controls (mean 5.9 pg/ml and 0.2 pg/ml, p<0.05). Among these patients (n=22), 63.5% (n=14) had deep endometriosis. A higher concentration of IL-10 was also observed in patients with ovarian endometriosis when compared to those without this type of disease, as well as when compared to control group patients (mean 50pg/ml, 18.7pg/ ml and 25.7pg/ml, p<0.05).
cOnclusiOns. These results suggest that when speciic clinical data are associated with a higher production of certain cytokines, there is a Th1 response pattern that may be related to deep iniltrating endometriosis.
Keywords: Endometriosis. Allergy and Immunology.Cytokines.Th1 Cells.Th2 Cells.
th
1
and
th
2
iMMune
RespOnses
Related
tO
pelvic
endOMetRiOsis
seRgiO pOdgaec1*, jOãO antOniO dias juniOR2, chaRles chapROn3, RicaRdO ManOelde OliveiRa4, edMund chada baRacat5,MauRíciO siMões abRãO6 Trabalho realizado no Departamento de Obstetrícia e Ginecologia da Faculdade de Medicina da Universidade de São Paulo
1. Doutor em Ginecologia pela Faculdade de Medicina da Universidade de São Paulo – USP e Médico Assistente da Clínica Ginecológica do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo – HCFMUSP, São Paulo, SP
2. Pós-graduando pela Faculdade de Medicina da Universidade de São Paulo – FMUSP, São Paulo, SP
3. Professor Department de Gynécologie CHU Cochin- Sant Vincent de Paul, Université Descartes Paris V, Paris France, Paris, France 4. Patologista Clínico e Médico Chefe da RDO Diagnósticos, São Paulo, SP
5. Professor Titular da Disciplina de Ginecologia da Faculdade de Medicina da Universidade de São Paulo – FMUSP, São Paulo, SP
6. Professor Livre Docente pelo Departamento de Obstetrícia e Ginecologia da Faculdade de Medicina da Universidade de São Paulo – FMUSP, São Paulo, SP
intROductiOn
Endometriosis is characterized by the presence of endome-trial glands and/or stroma in extrauterine sites, principally in ovaries and uterosacral ligaments, and affects around 10-15%
of women during menacme1. Deep endometriosis is the more
aggressive form of this disease and it iniltrates the retrocervical area, posterior vaginal wall, rectosigmoid regions, ureters and bladder to a depth of more than 5 mm and may even involve pelvic lymph nodes2,3.
Various investigators have studied the role of the immuno-logical system in endometriosis, and several abnormalities have
been detected4. The principal line of current reasoning provides
an update on the menstrual relux theory5 by hypothesizing that
the endometrial cells penetrating the peritoneal cavity should
normally be swept out by the organism defense system since these cells do not belong to this site. However, in women with endometriosis, this mechanism could suffer a bias and the process of adequate cell removal would fail to occur, permitting implantation and development of these cells in the peritoneal cavity, leading to formation of the initial endometriotic foci6.
The Th1/Th2 imbalance hypothesis is based upon the concept that T helper lymphocytes are involved with two different
patterns of cytokine secretion7. Th1 cells stimulate production of
a Th2 overstated pattern is present in allergic diseases8.
In several clinical situations, depending on the
characteris-tics of each disease, such as AIDS9, cardiac10 and neurological
disorders11 and in human reproduction12, a certain type of Th1/
Th2 immune response pattern is predominant. Our previous results showed that endometriosis is a complex disease with co-existence of both responses since we observed an increase in Interferon-gamma and IL-10 in patients with endometriosis when
compared to a control group of patients without the disease13.
In deeply iniltrating endometriosis, the characteristics of cell immunity appear to predominate, with the action of cells, enzymes and cytokines provoking adhesion, iniltration and maintenance of the foci of ectopic endometrial tissue. In view of these indings, the present study brings the theory of Th1/Th2 balance to endometriosis by proposing to evaluate the predomi-nant pattern of Th1 over Th2 immune response in accordance with characteristics of the disease such as clinical status, staging and sites affected by endometriosis.
MethOds
Ninety-eight patients were consecutively included in a pros-pective study between January 2004 and November 2005 at the Endometriosis Clinic, Department of Gynecology at the Teaching Hospital of the University Of São Paulo School Of Medicine. The institution’s internal review board approved the study (Approval # 601/03), and all participants read and signed the informed consent form.
Clinical suspicion of endometriosis was based upon patient symptoms and included dismenorrhea, deep dyspareunia, chronic pelvic pain, infertility and cyclical alterations in bowel and urinary habits occurring only during menstruation. After physical exam, patients were submitted to transvaginal ultra-sound and MRI. According to the suspicion of presence of ovarian endometrioma, deep iniltrating lesions or if the patient had persistent pain or infertility, a surgical laparoscopic procedure was indicated. Laparoscopy was performed by the same surgeons (SP, MSA), all endometriotic tissue was resected for histological conirmation of the disease.
Once the surgical indication had been deined, 5 ml of peripheral blood were collected prior to initiating anesthesia procedures. Immediately after the lens was passed through the infraumbilical catheter, 2-10 ml of peritoneal luid were collected from the anterior and/or posterior cul-de-sac. There was no perito-neal luid in twelve patients during laparoscopy, peritoperito-neal lushing was not used to obtain luid samples and there was no gross blood
contamination. The material was frozen at -80oC and was only
thawed for cytokine measurement after all data had been collected. Patients were then divided into two groups: those with endo-metriosis (group A) and those without the disease (group B). Inclusion criteria for Group A were: 18-40 years of age, histologi-cally conirmed endometriosis, absence of autoimmune disease, eumenorrheic patients with menstrual cycles of 26-32 days and non-use of hormone therapy in the three months preceding surgical procedure. Inclusion criteria for Group B were identical to those for Group A except for absence of endometriosis, which was conirmed during surgery.
During the surgical procedure, patients with endometriosis had their disease classiied in stages I to IV in accordance with
the criteria of the American Society for Reproductive Medicine (Revised ASRM, 1996). However, for the purposes of statistical analysis, stages I and II were grouped together and referred to as initial stages, while stages III and IV were grouped together and referred to as advanced stages of the disease. Sites affected by the disease were deined according to the following criteria: for the disease to be considered peritoneal, foci had to be exclusively peritoneal without presence of the deep disease (retrocervical, posterior vaginal wall and rectosigmoid regions, ureters and bladder) or ovarian disease. Ovarian endometriosis was deined as the absence of deep disease irrespective of peritoneal foci, whereas in the deinition of deep endometriosis no restrictions were made with respect to the presence of peritoneal or ovarian disease.
Cytokine measurement
The cytokines analyzed in this study, tumor necrosis factor-alpha, interferon-gamma, interleukin-2, interleukin-4 and inter-leukin-10, were measured using a low cytometer (BD FACS -Calibur, Franklin Lakes, New Jersey, USA). The kit used for measuring cytokines was the BD Cytometric Bead Array (CBA), catalogue 551809, manufactured by Pharmingen, Becton Dickinson & Co. (San Diego, California, USA). All tests were carried out in accordance with the manufacturer’s instructions.
Statistical analysis
Categorical variables were analyzed using the Chi-square test and continuous quantitative variables were compared using the non-parametric Mann-Whitney test. Patients with endometriosis were classiied according to stage and site affected, and non-parametric analysis was carried out using the Kruskal-Wallis test. All statistical calculations were performed with the SPSS software program (SPSS Inc., USA) and the level of signiicance established was 5%.
Results
Ninety-eight women were analyzed, 65 with endometriosis (Group A) and 33 without the disease (Group B). Mean age of patients in Group A was 32.1 ± 5.4 years, not signiicantly different from that of patients in Group B, 32.9 ± 5.1 years.
Concerning clinical data, there was a statistical difference between the two groups: 64.6% and 49.2% of patients with endo-metriosis presented, respectively, dysmenorrhea and cyclic bowel symptoms, while 27.3% and 6.1% of patients without the disease presented these complaints. Among patients with endometriosis who complained of deep dyspareunia (n=32), 65.5% had DIE, while among those who did not have this symptom (n=33), 30.3% had deep endometriosis.
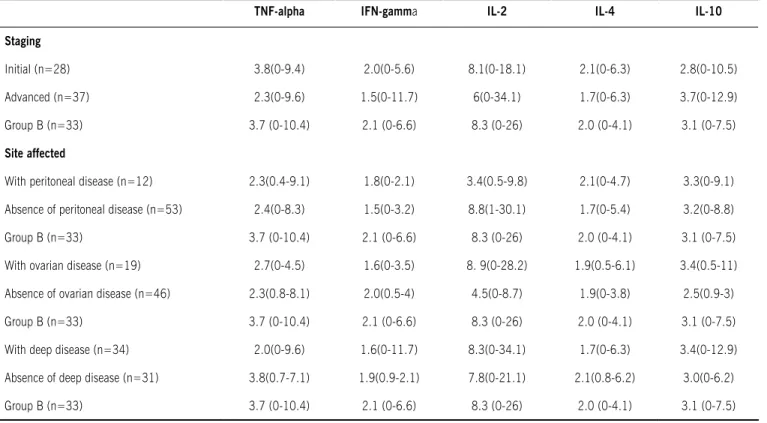
Table 2- Comparison of median (range) serum cytokine concentrations (pg/ml) between groups of patients with (a) and without (B) endometriosis according to staging (aSrm, 1996) and site affected by endometriosis.
TNF-alpha IFN-gamma IL-2 IL-4 IL-10
Staging
Initial (n=28) 3.8(0-9.4) 2.0(0-5.6) 8.1(0-18.1) 2.1(0-6.3) 2.8(0-10.5)
Advanced (n=37) 2.3(0-9.6) 1.5(0-11.7) 6(0-34.1) 1.7(0-6.3) 3.7(0-12.9)
Group B (n=33) 3.7 (0-10.4) 2.1 (0-6.6) 8.3 (0-26) 2.0 (0-4.1) 3.1 (0-7.5)
Site affected
With peritoneal disease (n=12) 2.3(0.4-9.1) 1.8(0-2.1) 3.4(0.5-9.8) 2.1(0-4.7) 3.3(0-9.1)
Absence of peritoneal disease (n=53) 2.4(0-8.3) 1.5(0-3.2) 8.8(1-30.1) 1.7(0-5.4) 3.2(0-8.8)
Group B (n=33) 3.7 (0-10.4) 2.1 (0-6.6) 8.3 (0-26) 2.0 (0-4.1) 3.1 (0-7.5)
With ovarian disease (n=19) 2.7(0-4.5) 1.6(0-3.5) 8. 9(0-28.2) 1.9(0.5-6.1) 3.4(0.5-11)
Absence of ovarian disease (n=46) 2.3(0.8-8.1) 2.0(0.5-4) 4.5(0-8.7) 1.9(0-3.8) 2.5(0.9-3)
Group B (n=33) 3.7 (0-10.4) 2.1 (0-6.6) 8.3 (0-26) 2.0 (0-4.1) 3.1 (0-7.5)
With deep disease (n=34) 2.0(0-9.6) 1.6(0-11.7) 8.3(0-34.1) 1.7(0-6.3) 3.4(0-12.9)
Absence of deep disease (n=31) 3.8(0.7-7.1) 1.9(0.9-2.1) 7.8(0-21.1) 2.1(0.8-6.2) 3.0(0-6.2)
Group B (n=33) 3.7 (0-10.4) 2.1 (0-6.6) 8.3 (0-26) 2.0 (0-4.1) 3.1 (0-7.5)
Table 1 - Comparison of median (range) serum cytokine concentrations (pg/ml) between groups of patients with (a) and without endometriosis (B) according to clinical status.
TNF-alpha IFN-gamma IL-2 IL-4 IL-10
Dysmenorrheaa
Group A (n=42) 2.6 (0-9.1) 1.7(0-5.6) 7.2(0-26) 2.0(0-6.3) 3.3(0-12.9)
Group B (n=9) 4.4(1.3-9.8) 2.4(1.3-3.5) 9.3(2.5-9.7) 3.0(0-4.1) 4.9(1.2-6.9)
Dyspareunia
Group A (n=32) 4.5*(0-9.6) 1.6(0-4.1) 7.6(0-23.3) 1.8(0-6.1) 3.0(0-6.1)
Group B (n=12) 2.3(1.3-3.5) 2 (0-6.6) 8.0(0-26) 2.9(1.2-3.5) 3.6(0-4.5)
Chronic pelvic pain
Group A (n=39) 2.0(0-8.1) 0.9(0-11.7) 6.1(0-34.1) 1.7(0.6-4) 3.2(0-12.1)
Group B (n=13) 3.5(2.1-10.4) 2.1(1.8-6.5) 9.7(2.8-9.9) 2.6(1.5-2.9) 3.0(1.2-3.9)
Infertility
Group A (n=22) 2.2(0-5.5) 1.7(1.1-5.2) 5.9(2.5-8) 1.7(0-6.1) 2.5(0-4.5)
Group B (n=8) 4.2(1.8-10.4) 1.8(1.3-6.5) 2.7(0-11) 2.0(1.2-4.1) 3.1(0-5.9)
Cyclical alterations in bowel habits
Group A (n=32) 2.3(1.1-9.5) 1.4(0-11.7) 6.1(1.3-8.2) 1.5(0.8-6.3) 3.6(0-12.5)
Group B (n=1) 6.2 2.8 8.1 2.2 2.6
Cyclical alterations in urinary habits
Group A (n=1) 2.3 0.8 4.6 1.4 2.8
Group B (n=0) - - - -
Comparison of median cytokine concentrations measured in peritoneal luid of patients evaluated, is shown in Table 3. Patients with endometriosis, who had infertility, had higher IL-2 levels than controls. Among all patients with infertility and endometriosis (n=22), 63.5% (n=14) were found to have DIE.
Comparing the characteristics of the disease between cases and controls in relation to cytokine measurements in peritoneal luid, higher IL-10 levels were found in cases of ovarian endo -metriosis in absence of deep disease, irrespective of the presence of peritoneal foci (Table 4).
discussiOn
Endometriosis is a disease with different facets. It probably starts from endometrial relux or cell metaplasia and provokes
pelvic pain and infertility or may cause no clinical symptoms14.
Participation of the immunological system in some of steps in this process is logical and agrees with current literature4. The humoral
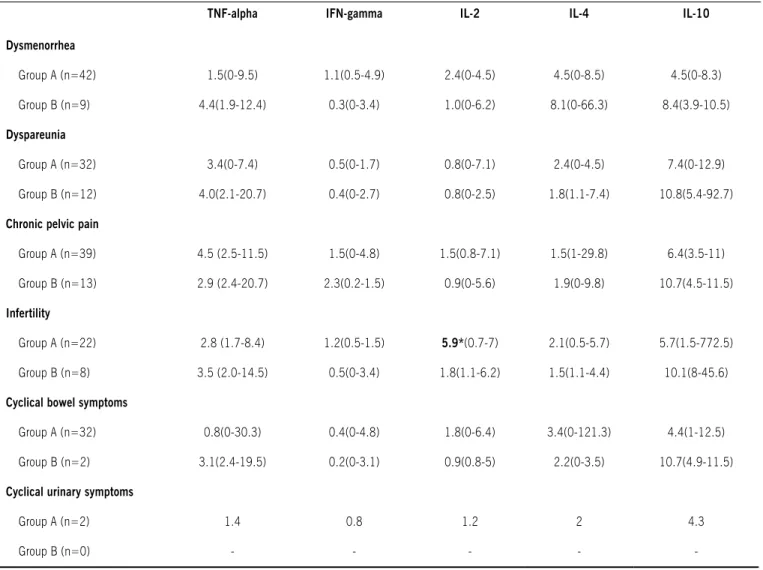
Table 3 - Comparison of median (range) cytokine concentrations measured in peritoneal luid (pg/ml) between groups of patients with (A) and without endometriosis (B) according to clinical status.
TNF-alpha IFN-gamma IL-2 IL-4 IL-10
Dysmenorrhea
Group A (n=42) 1.5(0-9.5) 1.1(0.5-4.9) 2.4(0-4.5) 4.5(0-8.5) 4.5(0-8.3)
Group B (n=9) 4.4(1.9-12.4) 0.3(0-3.4) 1.0(0-6.2) 8.1(0-66.3) 8.4(3.9-10.5)
Dyspareunia
Group A (n=32) 3.4(0-7.4) 0.5(0-1.7) 0.8(0-7.1) 2.4(0-4.5) 7.4(0-12.9)
Group B (n=12) 4.0(2.1-20.7) 0.4(0-2.7) 0.8(0-2.5) 1.8(1.1-7.4) 10.8(5.4-92.7)
Chronic pelvic pain
Group A (n=39) 4.5 (2.5-11.5) 1.5(0-4.8) 1.5(0.8-7.1) 1.5(1-29.8) 6.4(3.5-11)
Group B (n=13) 2.9 (2.4-20.7) 2.3(0.2-1.5) 0.9(0-5.6) 1.9(0-9.8) 10.7(4.5-11.5)
Infertility
Group A (n=22) 2.8 (1.7-8.4) 1.2(0.5-1.5) 5.9*(0.7-7) 2.1(0.5-5.7) 5.7(1.5-772.5)
Group B (n=8) 3.5 (2.0-14.5) 0.5(0-3.4) 1.8(1.1-6.2) 1.5(1.1-4.4) 10.1(8-45.6)
Cyclical bowel symptoms
Group A (n=32) 0.8(0-30.3) 0.4(0-4.8) 1.8(0-6.4) 3.4(0-121.3) 4.4(1-12.5)
Group B (n=2) 3.1(2.4-19.5) 0.2(0-3.1) 0.9(0.8-5) 2.2(0-3.5) 10.7(4.9-11.5)
Cyclical urinary symptoms
Group A (n=2) 1.4 0.8 1.2 2 4.3
Group B (n=0) - - - -
-* p<0.05
immune response may explain endometriosis in general terms, in
accordance with the characteristics of an autoimmune disease15.
Particularly, in more aggressive, iniltrating forms of the disease, there appears to be a predominant action of cell immunity, with cells, enzymes and cytokines provoking adhesion, iniltration and maintenance of the foci of ectopic endometrial tissue.
Deeply iniltrating endometriosis is a major issue in several studies related to this disease, including etiopathogenesis, clin-ical data, imaging methods and an intense clinclin-ical and surgclin-ical treatment debate 16,17,18,19,20,21 . There are still some topics that
have no consensus, such as the best imaging method for
diag-nosis of deep lesions (mainly bowel endometriosis)18,19 and the
best option for treatment of these lesions, due to the complication risk related to the more advanced surgical procedures20,21. It is
site affected by the disease, such as intestinal and urinary cyclic
alterations and deep dyspareunia, respectively22. Further, Chapron
et al. (2009) evaluated 500 patients with deep endometriosis and observed that presence of ovarian endometrioma can be a marker for severity of deeply iniltrating endometriosis and when the patient has severe dysmenorrhea, pain is probably due to deep lesions, mainly rectal iniltration, and not to the ovarian cyst23,24.
In this study, we have endeavored to identify the cytokine proile associated with Th1 and Th2 response that may predomi -nate in patients with endometriosis, and which would conirm participation of immunological alterations and encourage further research leading to new therapeutic modalities for the disease. The design of this study has its own limitations due to the vari-ability of cytokine concentrations as seen in the wide range of these measures and in the use of median values for statistical analysis of data. In addition, the different volume of peritoneal luid obtained from each patient is a factor that has to be consid -ered as in 12 patients there was no luid in the peritoneal cavity. We did not propose a peritoneal lush because mechanical infu -sion of any liquid and action involved in washing the peritoneal cavity could provoke local stress, “unbinding” molecules not spontaneously present in the peritoneal luid, as well as leading to a quick inlammatory response with alterations in the micro-environment under evaluation. These points could affect true results of cytokine concentration.
Our previous report analyzed this cytokine proile and showed that IFN-gamma and IL-10 increased signiicantly in the peritoneal luid of patients with endometriosis compared to those without endometriosis. However, there was a signiicant alteration of Th2:Th1 ratios in peritoneal luid of patients with endometriosis, with a predominance of IL-4 and IL-10, relecting a shift towards Th2 immune response despite increased IFN-gamma concentrations. These results allowed us to conclude that endometriosis is an inlammatory disease involving a possible
shift towards a Th2 immune response component13.
Analysis of the clinical status of groups in this study revealed a statistically signiicant difference with respect to patients with endometriosis, a higher percentage of those with dysmenorrhea and cyclical alterations in bowel habits compared to women without the disease. This agrees with the clinical proiles of the disease evaluated in Brazil25 and in other countries26,27,
where almost 90% of patients with endometriosis complained of dysmenorrhea and 40% reported cyclical alterations in bowel habits.
Comparison was made between the intensity of symptoms reported by patients and severity of the disease as diagnosed during surgical procedures. A direct correlation was observed, the more intense the symptoms, the more severe the disease. One example of this inding is that 65.5% of patients with endometriosis who reported deep dyspareunia had a deeply
Table 4 - Comparison of the median (range) cytokine concentrations measured in peritoneal luid (pg/ml) between groups of patients with (A) and without endometriosis (B) according to staging (aSrm, 1996) and site affected by endometriosis
TNF-alpha IFN-gamma IL-2 IL-4 IL-10
Staging
Initial (n=28) 3.3(0-13.2) 0.4(0-2.1) 1.5(0-7.1) 1.2(0-21.4) 18.7(0-78.1)
Advanced (n=37) 2.9(0-30.3) 0.6(0-4.9) 1.4(0-4.3) 2.1(0-121.3) 46.1(0-772.5)
Group B (n=33) 1.4 (0-20.7) 0 (0-3.4) 0 (0-6.2) 0 (0-66.3) 25.7 (3.2 -92.7)
Site affected
Peritoneal disease (n=12) 2.8(0-11.3) 1.1((0.5-2.9) 0.8(0-1.2) 2.0(0-121.3) 27.1(0-34.1)
Absence of peritoneal disease (n=36) 3.4(1.2-21.1) 0.9(0-1.2) 0.8(0.5-1.1) 1.6(0-12.1) 30.9(3.1-55.2)
Group B (n=33) 1.4 (0-20.7) 0 (0-3.4) 0 (0-6.2) 0 (0-66.3) 25.7 (3.2 -92.7)
Ovarian disease (n=19) 2.4(0-3.9) 2.2(0.5-1.8) 2.1(1.1-4.5) 1.7(0.5-4.3) 50*(5.4-772.5)
Absence of ovarian disease (n=24) 3.8(0.5-9.2) 0.7(0-4.9) 0.7(0-7.1) 2.0(0.9-11) 18.7(0-32.7)
Group B (n=33) 1.4 (0-20.7) 0 (0-3.4) 0 (0-6.2) 0 (0-66.3) 25.7 (3.2 -92.7)
Deep disease (n=34) 3.2(1.5-30.3) 2.9(0-4.9) 0.8(0-3.2) 2.0(1.1-23) 30.9(0-98.4)
Absence of deep disease (n=31) 2.4(0-7.1) 1.5(0.8-4.1) 1.4(0-1.9) 0.6(0-9.8) 25.5(2.2-57.3)
Group B (n=33) 1.4 (0-20.7) 0 (0-3.4) 0 (0-6.2) 0 (0-66.3) 25.7 (3.2 -92.7)
iniltrating form of the disease, and of those who did not report this symptom, only 30.3% had deep endometriosis. Fauconnier & Chapron (2005) reached similar conclusions and showed that, in cases of deep endometriosis, symptoms had some speciicity with the site affected by the lesion28.
In cases of greater extension of the disease, with adher-ences and signiicant anatomical distortion, the explanation for the symptomatology reported by patients has been credited to the inlammatory process that installs itself in the pelvis, with an increase in production of prostaglandins and lysosomal enzymes inducing ibrosis29. Alterations observed in this study
are in accordance with these data, since in patients with deep dyspareunia, there is an increased concentration of TNF-alpha, a cytokine that may be a marker of Th1 response, but may also be produced by other cell types in a non-speciic inlammatory response. Regardless of its origin, TNF-alpha is directly involved in the action of NK cells, cytotoxic T lymphocytes, VEGF secre-tion and metalloproteinase matrix enzymes, and also plays an important role in the apoptosis observed in sites of acute or chronic inlammation.
Patients in Group A reporting infertility had higher concentra-tions of IL-2 in peritoneal luid compared to patients in Group B. Analysis of patients in whom this increase occurred revealed that in 63.6% of the cases, deep endometriosis was detected. This type of disease generally impairs fertility more often than supericial endometriosis due to ibrotic processes that may affect the uterine tubes, essential organs in the process of spontaneous
fertilization30. The elevation of a pro-inlammatory citokyne such
as IL-2 in patients with deep endometriosis could be involved in the pathogenesis of infertility, but clearly further studies have to be made to conirm this hypothesis.
A single study involving IL-10 in cases of advanced disease showed an increase of this cytokine in the peritoneal luid of patients with this speciic type of endometriosis31. In the present
analysis, IL-10 was higher in the peritoneal luid of patients with ovarian endometriosis but not in those with the deep disease, irrespective of the presence of peritoneal lesions. Our previous results showed that IFN-gamma was higher in the peritoneal luid of patients with endometriosis compared to patients without the disease, and when analysis was made of these cases, it was found that 9 out of 13 patients (69.2%) who had increased levels
of IFN-gamma had deep endometriosis13.
Regarding staging of endometriosis, no statistically signiicant differences were found in our study about cytokine measurement and Th1 and Th2 response patterns. Increased concentrations of TNF-alpha have already been described in relation to advanced stages32, initial stages33 and in cases where no relation could be
perceived with the stage of endometriosis34. Concerning deep
endometriosis, statistical analysis showed no signiicant differ -ence in cytokine concentrations. Nevertheless, according to our indings, there appears to be a trend towards stronger participa -tion of Th1 response in these cases.
Results achieved in this study are coherent with those previ-ously published that allowed us to stress that endometriosis is a complex disease with an inlammatory behavior and a Th2 immune response component. IFN-gamma concentra-tions in the peritoneal luid were increased in patients with the
disease13. In the present study, TNF-alpha and IL-2 had higher
concentrations in endometriosis patients with dyspareunia and infertility when compared to patients without the disease. These cytokines, mainly IFN-gamma and IL-2, are related to Th1 immune response and almost 70% of patients that presented these results had DIE lesions
In conclusion, although there were no differences concerning Th1/Th2 immune response patterns in relation to the site of endo-metriotic lesions, information presented here suggests that, when speciic clinical data are associated with a greater production of speciic cytokines, there is a Th1 response pattern that may be associated with deeply iniltrating endometriosis.
acknOwledgMents:
The São Paulo State Foundation for the Support of Research (FAPESP) provided
inancial support for this study through grant 05/01218-3.
supORte FinanceiRO:
FAPESP 05/01218-3
Conlito de interesse: não há
ResuMO
RespOsta iMunOlógica th1 e th2 RelaciOnada à endOMetRiOse pélvica
ObjetivO. Este estudo analisa a relação entre as
caracterís-ticas clínicas da endometriose e os padrões da resposta imune Th1/Th2.
MétOdOs. Estudo prospectivo realizado com 65 pacientes
com endometriose (Grupo A) e 33 pacientes sem a doença (Grupo B). Foram realizadas avaliação no fluido peritoneal e sangue periférico de IL 2, 4 e 10, TNF-alfa e IFN-gama. A significância foi estabelecida em p < 0,05.
ResultadOs. TNF-alfa encontrava-se elevado em pacientes com
endometriose que apresentavam dispareunia de profundidade comparado com controle (média 4,5 pg/ml e 2,3 pg/ml, p< 0,05). Dentre essas pacientes (n=32), 65,5% apresentavam endo-metriose profunda. Pacientes com endoendo-metriose e infertilidade apresentavam concentrações maiores de IL-2 no fluido peritoneal quando comparadas com controle (média 5,9 pg/ml e 0,2 pg/ml, p< 0,05), sendo que neste grupo, 63,5% (n=14) apresentavam endometriose profunda. Foi observada também maior concen-tração de IL-10 nas pacientes que apresentavam endometriose ovariana quando comparadas às sem esse tipo de endometriose, assim como quando comparadas às pacientes do grupo controle (média 50pg/ml, 18,7pg/ml e 25,7pg/ml, p<0,05).
COnClusãO. Estes resultados sugerem que quando dados
clínicos específicos associam-se a uma produção elevada de certas citocinas, ocorre um padrão de resposta Th1 que pode
estar associado à endometriose profunda. [Rev Assoc Med Bras
2010; 56(1): 92-8]
ReFeRences
1. Eskenazi B, Warner ML. Epidemiology of endometriosis. Obstet Gynecol Clin North Am. 1997;24:235-58.
2. Chapron C, Chopin N, Borghese B, Foulot H, Dousset B, Vacher-Lavenu MC,
et al. Deeply iniltrating endometriosis: pathogenetic implications of the
anatomical distribution. Hum Reprod. 2006;21:1839-45.
3. Abrao MS, Podgaec S, Dias Jr JA, Averbach M, Garry R, Silva LF, et al. Deeply
iniltrating endometriosis affecting the rectum and lymph nodes. Fertil Steril.
2006;86:543-7.
4. Berkkanoglu M, Arici A. Immunology and endometriosis. Am J Reprod Immunol. 2003;50:48-59.
5. Sampson JA. Peritoneal endometriosis due to menstrual dissemination of endometrial tissue into the peritoneal cavity. Am J Obstet Gynecol. 1927;14:422-69.
6. Harada T, Iwabe T, Terakawa N. Role of cytokines in endometriosis. Fertil Steril. 2001;76:1-10.
7. Mosmann TR, Cherwinski H, Bond MW. Two types of murine helper T cell
clone: deinition according, to proiles of lymphokine activities and secreted
proteins. J Immunol. 1986;136:2348-57.
8. Benjamini E, Coico R, Sunshine G. Ativação e função dos linfócitos T e B. In: Benjamini E, Coico R, Sunshine G, editores. Imunologia . Rio de Janeiro:
Guanabara Koogan 2002. p.11-25.
9. Norris PJ, Rosenberg ES. Cellular immune response to human immunodei -ciency virus. AIDS. 2001;15(Suppl 2):S16-21.
10. Adler A, Levy Y, Roth A, Wexler D, Keren G, George J. Functional T-lymphocyte dichotomy in the peripheral blood of patients with unstable angina. Int J Cardiovasc Intervent. 2005;7:146-51.
11. Arumugam TV, Granger DN, Mattson MP. Stroke and T-cells. Neuromolecular Med. 2005; 7:229-42.
12. Kwak-Kim JY, Gilman-Sachs A, Kim CE. T helper 1 and 2 immune responses in relationship to pregnancy, nonpregnancy, recurrent spontaneous abortions and infertility of repeated implantation failures. Chem Immunol Allergy. 2005;88:64-79.
13. Podgaec S, Abrao MS, Dias Jr JA, Rizzo LV, Oliveira RM, Baracat EC.
Endo-metriosis: an inlammatory disease with a Th2 immune response component.
Hum Reprod. 2007, 22:1373-9.
14. Abrao MS, Neme RM, Carvalho FM, Aldrighi JM, Pinotti JA. Histological
classiication of endometriosis as a predictor of response to treatment. Int J
Gynaecol Obstet. 2003;82:31-40.
15. Nothnick WB. Treating endometriosis as an autoimmune disease. Fertil Steril. 2001;76:223-31.
16. Wang G, Tokushige N, Markham R, Fraser IS. Rich innervation of deep inil -trating endometriosis. Hum Reprod. 2009;24:827-34.
17. Podgaec S, Gonçalves MO, Klajner S, Abrão MS. Epigastric pain relating to menses can be a symptom of bowel endometriosis. Sao Paulo Med J. 2008; 126:242-4.
18. Goncalves MO, Dias JA Jr, Podgaec S, Averbach M, Abrão MS. Transvaginal
ultrasound for diagnosis of deeply iniltrating endometriosis. Int J Gynaecol
Obstet. 2009;104:156-60.
19. Guerriero S, Alcázar JL, Ajossa S, Pilloni M, Melis GB.. Three-dimensional sonographic characteristics of deep endometriosis. J Ultrasound Med. 2009;28:1061-6.
20. Vercellini P, Carmignani L, Rubino T, Barbara G, Abbiati A, Fedele L. Surgery for deep endometriosis: a pathogenesis-oriented approach. Gynecol Obstet Invest. 2009;68:88-103.
21. Stepniewska A, Pomini P, Bruni F, Mereu L, Ruffo G, Ceccaroni M, Scioscia M, Guerriero M, Minelli L. Laparoscopic treatment of bowel endometriosis in infertile women. Hum Reprod. 2009;24:1619-25.
22. Seracchioli R, Mabrouk M, Guerrini M, Manuzzi L, Savelli L, Frascà C, Venturoli
S. Dyschezia and posterior deep iniltrating endometriosis: analysis of 360
cases. J Minim Invasive Gynecol. 2008;15:695-9.
23. Chapron C, Pietin-Vialle C, Borghese B, Davy C, Foulot H, Chopin N. Associated
ovarian endometrioma is a marker for greater severity of deeply iniltrating
endometriosis. Fertil Steril. 2009;92:453-7.
24. Chopin N, Ballester M, Borghese B, Fauconnier A, Foulot H, Malartic C, Chapron C. Relation between severity of dysmenorrhea and endometrioma. Acta Obstet Gynecol Scand. 2006;85:1375-80.
25. Abrao MS, Podgaec S, Izzo CR, Melo PV, Porto RC, Ramos LO, et al. Peril
epidemiológico e clínico da endometriose - análise de 180 casos. Rev Bras Ginecol Obstet. 1995;17:779-84.
26. Hemmings R, Rivard M, Olive DL, Poliquin-Fleury J, Gagne D, Hugo P, et al. Evaluation of risk factors associated with endometriosis. Fertil Steril. 2004; 81:1513-21.
27. Perry R. Endometriosis: a gynaecological and colorectal disease. N Z Med J. 2005;118(1217):U1535.
28. Fauconnier A, Chapron C. Endometriosis and pelvic pain: epidemiolo-gical evidence of the relationship and implications. Hum Reprod Update. 2005;11:595-606.
29. Thomson JC, Redwine DB. Chronic pelvic pain associated with autoimmunity
and systemic and peritoneal inlammation and treatment with immune modi
-ication. J Reprod Med. 2005;50:745-58.
30. Darai E, Marpeau O, Thomassin I, Dubernard G, Barranger E, Bazot M. Fertility after laparoscopic colorectal resection for endometriosis: preliminary results. Fertil Steril. 2005;84:945-50.
31. Tabibzadeh S, Becker JL, Parsons AK. Endometriosis is associated with
altera-tions in the relative abundance of proteins and IL-10 in the peritoneal luid.
Front Biosci. 2003;8:a70-8.
32. Richter ON, Dorn C, Rosing B, Flaskamp C, Ulrich U. Tumor necrosis factor alpha secretion by peritoneal macrophages in patients with endometriosis. Arch Gynecol Obstet. 2005;271:143-7.
33. Pizzo A, Salmeri FM, Ardita FV, Sofo V Tripepi M, Marsico S. Behaviour of
cytokine levels in serum and peritoneal luid of women with endometriosis.
Gynecol Obstet Invest. 2002;54:82-7.
34. Iwabe T; Harada T; Terakawa N. Role of cytokines in endometriosis-associated infertility. Gynecol Obstet Invest. 2002;53(Suppl 1):19-25.