SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Comparison
of
Puddu
osteotomy
with
or
without
autologous
bone
grafting:
a
prospective
clinical
trial
夽
Marcus
Ceregatti
Passarelli,
José
Roberto
Tonelli
Filho,
Felipe
Augusto
Mendes
Brizzi,
Gustavo
Constantino
de
Campos,
Alessandro
Rozim
Zorzi
∗,
João
Batista
de
Miranda
UniversidadeEstadualdeCampinas(Unicamp),DepartamentodeOrtopediaeTraumatologia,Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4August2016 Accepted7September2016 Availableonline14September2017
Keywords:
Knee Osteoarthritis Bonegraft Osteotomy
a
b
s
t
r
a
c
t
Objectives: Totestthehypothesisthatautologousiliacbonegraftsdonotenhanceclinical results anddonotdecrease complicationrates inpatientsundergoingmedial opening-wedgehightibialosteotomy.
Methods:Fortypatientsallocatedinarandomized,two-armed,double-blindedclinicaltrial wereevaluatedbetween2007and2010.Onegroupreceivedbonegraft,andtheothergroup wasleftwithoutfillingtheosteotomydefect.TheprimaryoutcomewastheKneeSociety Score.Radiographicmeasurementofthefrontalanatomicalfemoral-tibialangleandthe progressionofosteoarthritisaccordingtothemodifiedAhlbackclassificationwereusedas secondaryoutcomes.
Results:There wasnodifferenceinKSS scalebetweenthegraftgroup(64.4±21.8) and thegraftlessgroup(61.6±17.3;p=0.309).Therewasnodifferenceofanglebetweenthe femur andtibia inthefrontalplanebetweenthegroups(graft=184±4.6degrees, graft-less=183.4±5.1degrees;p=1.0),indicatingthatthereisnolossofcorrectionduetothe lackofthegraft.Therewassignificantaggravationofosteoarthritisinagreaternumberof patientsinagraftgroup(p=0.005).
Conclusion: Autologousiliacbonegraftdoesnotimproveclinicaloutcomesinmediumand long-termfollow-upofmedialopening-wedgehightibialosteotomyfixedwithafirst gen-erationPudduplateintheconditionsofthisstudy.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
PaperdevelopedatUniversidadeEstadualdeCampinas(UNICAMP),DepartamentodeOrtopediaeTraumatologia(DOT),Campinas, SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.R.Zorzi). http://dx.doi.org/10.1016/j.rboe.2017.09.001
Comparac¸ão
de
osteotomias
de
Puddu
com
ou
sem
enxerto
ósseo
autólogo:
estudo
clínico
prospectivo
Palavras-chave:
Joelho Osteoartrite Enxertoósseo Osteotomia
r
e
s
u
m
o
Objetivos: Avaliarahipótesedequeoenxertoósseoautólogodacristailíacanãomelhora oresultadoclínicoenãodiminuiaincidênciadecomplicac¸õesempacientessubmetidosà osteotomiadePuddu.
Métodos: Foramavaliados40pacientesalocadosdeformaaleatóriaemdoisgruposemum estudoclínicoduplocegoentre2007e2010.Umgruporecebeuenxertoósseoeooutrogrupo foideixadosempreenchimentodaosteotomia.Odesfechoprimáriofoiaescalaclínicada
KneeSociety(KSS).Amedidaradiográficadoânguloanatômicoentreofêmureatíbiano planofrontaleaprogressãodaosteoartritedeacordocomaclassificac¸ãomodificadade Ahlbackforamusadascomodesfechossecundários.
Resultados:Nãohouvediferenc¸adaescalaKSSnogrupocomenxerto(64,4±21,8)enogrupo semenxerto(61,6±17,3;p=0,309).Nãohouvediferenc¸adoânguloentreofêmureatíbia noplanofrontalentreosgrupos(comenxerto=184±4,6graus;semenxerto=183,4±5,1 graus;p=1,0),indicaquenãoháumaperdadecorrec¸ãopelafaltadoenxerto.Houvepioria daosteoartriteemumnúmeromaiordepacientesnogrupocomenxerto(p=0,005).
Conclusão: Oenxertoósseoautólogodacristailíacanãomelhorouoresultadoclínicoenão diminuiuaincidênciadecomplicac¸õesempacientessubmetidosàosteotomiadePuddu, fixadascomplaca-calc¸odeprimeiragerac¸ão,nascondic¸õesdesteestudo.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Theproximaltibialosteotomywithmedialopeningwedge, alsoknown asPuddu osteotomy,isaclassicalsurgical pro-cedureforthe treatment ofknee osteoarthritis,which has beenovershadowedbythedevelopmentofarthroplasty,but thathasresurgedduetotheincreasingnumberofcasesof osteoarthritisinyoungpatientsandnewsurgeries,suchas meniscaltransplantationandcartilagefillings,whichrequire adequatemechanicalalignmentofthelowerlimb.1Compared totheotherosteotomytechniques,themedialopeningofthe tibiahave asadvantagesthe less morbidaccessroute, the possibilityofeasy intraoperativeadjustmentofwedgesize, preservationofbonestock,correctionclosertotheapexof thedeformity,andeaseofassociationwithotherprocedures inasinglesurgicaltime,suchasreconstructionoftheanterior cruciateligament.1,2
Themaincriticismofthetechniqueofmedialopeningis thecreation ofacleftinthe metaphysealcancellous bone, which can progresswith complicationsof bone consolida-tionandthelossofcorrectionduetocleftcollapse.Theuse ofautologousbonegraftingoftheiliaccresthasbeen advo-cated sincethe beginning of this surgeryto prevent these complications.3,4Duetoitbeingapainfulprocedure, associ-atedwithseveralcomplications,bonesubstituteshavebeen developedtofillthecleft.However,autologousbonegrafting, duetoitsosteogenesis,osteoinductionandosteoconduction properties,remainsthegoldstandard.5
Theempiricalexperiencesuggeststhat,inopeningsofup to10mm,itispossibletoleavethecleftunfilled.Toconfirm thisobservation,thisteammadeashort-termevaluationof
theresultsofosteotomieswithandwithouttheadditionofa bonegraft,whichshowednodifferenceinthetimeof consol-idationaftersixmonthsoffollow-up.6Now,theobjectiveof thispaperisthelateevaluation,afteraminimumfollow-up offouryears,oftheclinicalandradiographicresultsobtained withorwithouttheadditionofthegraft.
Method
Subjects
Thestudysampleconsistedof46patientsundergoingPuddu osteotomy between 2007 and 2010, who were referred to surgicaltreatmentinauniversityhospitalafterfailureof non-surgicaltreatment.
Inclusioncriteria:
• Individualosteoarthritisofthemedialkneecompartment associatedwithvarusdeformity;
• Failureofnonsurgicaltreatment;
• Doublevarussecondarytochronicinstabilityofligament structuresoftheposterolateralcorner;
• AbilitytoreadandunderstandtheFreeInformedConsent Form (FIC), and agreement withthe participationin the research.
Exclusioncriteria:
Recruitment
Elegible (n = 48)
Allocated (n = 46)
Allocation
Follow-up
Analysis
Excluded (n = 2)
♦ Lack of inclusion criteria
(n = 1)
♦ Refused to participate (n = 0)
♦Other reasons (n = 1)
“With graft” (n = 23)
♦ Received a graft (n = 23)
♦ Did not receive a graft (n = 0)
“non-graft” (n = 23)
♦ Did not receive a graft (n = 23)
♦ Received a graft (n = 0)
Analyzed (n = 21)
♦ Excluded (n = 0)
Analyzed (n = 19)
♦ Excluded (n = 0) Lost to follow-up (n = 2)
Change of address and telephone number
Lost to follow-up (n = 4)
Change of address and telephone number
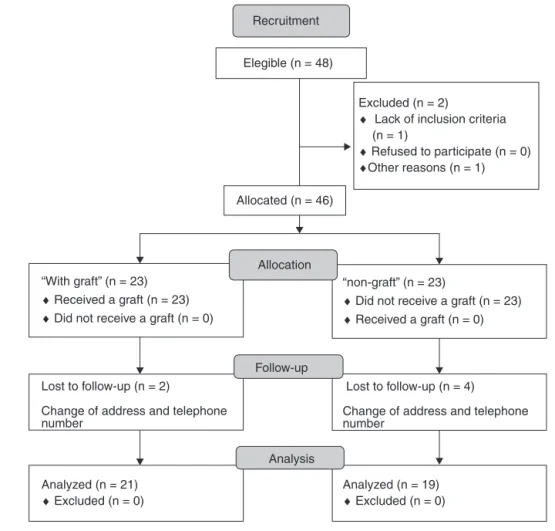
Fig.1–Studyconsortflowchart.
• Plannedcorrectionswithwedgeslargerthan12.5mm; • Previoussurgeriesintheaffectedknee;
• Previousinfectionsintheaffectedlimb;
• Paininthelateraloranteriorcompartmentsoftheaffected knee;
• Lateralmeniscusinjury;
• Severekneeosteoarthritis(grades4and5ofAhlback clas-sification).
ThestudywasapprovedbytheResearchEthicsCommittee (CEP679/2006)andregisteredintheplatformClinicalTrials.gov (NCT00786942).
Allocation
Forty-sixpatientswererandomlydivided,withtheuseofa software(www.random.org),intwogroupsof23individuals. Allofthemunderwentthesamesurgicalprocedure,except forthe placementornotofabonegraft.Afteraminimum follow-upoffouryears,40patientswereevaluated(Fig.1).
Masking
Theallocationwaskeptsecretwiththeuseofasealed enve-lope,openedonlyafteranestheticinductionbyanursethat wasnotinvolvedwiththestudy.Inaddition,inordertoensure
confidentialitybetweenpatientsandevaluators(double-blind study)ailiaccrestgraft washarvestedfrom allpatients.In the“withoutgraft”group,thebonewassealedundersterile conditionsandstoredinafreezer,withtheapprovalofCEP.
Intervention
Thevalgusosteotomyoftheproximaltibia,withmedial open-ing wedge, known inour setting asPuddu osteotomy, isa classicalandwell-establishedtechnique.2,3,7Inthisstudy,we used first-generation wedge-plate fixation.8,9 As previously stated,twogroupswererandomlycreated.Tokeepmasking, andtoavoidtheclinicalaggravationbiasduetoiliaccrestpain, thegraftwasharvestedinbothgroups.Theinterventionof thisstudywastheplacementofthegraft.Thecontrolgroup wasleftwithoutit.
Surgicaltechnique
All caseswere operatedbythesamesurgeon. Thedetailed descriptionofthetechniquehasalreadybeenmadeina pre-viouspublication.10
compartment(arthroscopictoilet).Atthattime,anursethat wasnotinvolvedintheresearchteamopenedtheenvelope withtheindicationofthepatient’sallocation.Inthecasesof the“no-graft”group,thebonewasvacuumpackedintriple polyamidepackagingandfrozeninaresearchlaboratory.At theendoftheprocedure,asuction drainwasplacedinall cases.
Postoperativeperiod
Thedrainwasalwaysremovedonthefirstdayaftersurgery. No type of immobilization was used and the limb active movement was stimulated on the first day after surgery. Therefore,nopharmacologicalprophylaxisforvenous throm-boembolismwasused. Tostandardizeloading,wechoseto leaveallpatientswithzeroloaduntiltheeighthweek(pair ofcrutches); gradual weight-bearing was started after this period.Allpatientshadthesamephysicaltherapyprotocol atthesamemedicalfacilitywheretheywereoperated.
After hospital discharge, the subjects were evaluated weeklyinanoutpatientclinic,bytworesearchersblindedto the allocation. Theradiographic evaluation wasperformed everyfifteendaysuntilconsolidation,whichwasdefinedby Solomonand Apleycriteria.11 Followingbonehealing, they wereevaluatedeverysixmonthsforthefirsttwoyears,and thenannually.
Outcomes
Thisstudy’smainoutcome wasthe clinicaland functional result ofthe Puddu osteotomy after atleast four years of follow-up,measuredbyKSS(KneeSocietyScore)scale.12 This scaleisdividedintwoparts:anobjectiveone,whichcanvary fromzerotoonehundred;andafunctionalone,thatcanvary fromzerotoonehundred.
Otheroutcomesusedwere:
• Correction obtained in the frontal plane, measured in frontal knee X-ray, with monopodal weight-bearing, throughthe angle formedbythe anatomical axisofthe femurandtibia13,14;
• Radiographic progression of knee osteoarthritis through modifiedAhlbackmethod15;
• Conversionofarthroplastyorosteotomyreview.
Statistics
Tocalculatethesamplesize,weconsideredasignificant clin-icaldifferencebetweenthe means ofthe twogroupsof20 points,with80%powerandsignificancewithalphalessthan 5%.
Datawerepresentedasmeanandstandarddeviation(SD) forcontinuousvariables,orasabsolutefrequencyfor categor-icalvariables.Allpvaluesreportedaretwo-tailed.Thelevel ofsignificancewassetat0.05.TheKolmogorov–Smirnovtest was appliedtodetermine if the datafollowed normal dis-tribution.The comparisonamongthecontinuous variables was made with Student’s t-test for independent samples, whentheparametricassumptionscouldbeobtained;inother cases,Mann–Whitneytestwasused.Amongthecategorical
Table1–Demographicdataoftheresearchsubjects.
Withgraft n=21
Withoutgraft n=19
p
Age(years) 49.7±9.5 49.1±9.2 0.801
BMI 29.0±4.9 28.2±6.6 0.204
Follow-up(months) 74.3±14.4 70.6±11.8 0.688 Wedgeplate(mm) 10.3±2.5 9.8±2.0 0.607
Ligamentlesion 12 10 0.328
Smokers 5 11 0.028a
BMI,bodymassindex.
a Significant.
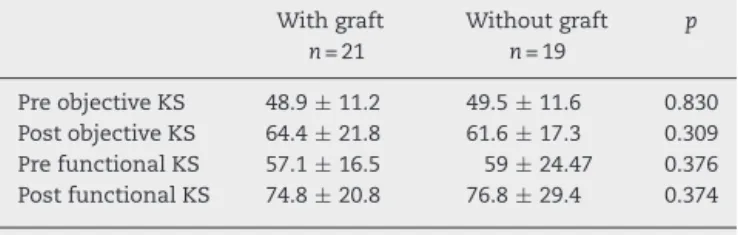
Table2–Resultofclinicalevaluationthroughobjective andfunctionalKSscales.
Withgraft n=21
Withoutgraft n=19
p
PreobjectiveKS 48.9±11.2 49.5±11.6 0.830 PostobjectiveKS 64.4±21.8 61.6±17.3 0.309 PrefunctionalKS 57.1±16.5 59±24.47 0.376 PostfunctionalKS 74.8±20.8 76.8±29.4 0.374
KS,Kneescore.
variables, Pearson’s chi-square test or Fisher’s test were applied.
All analyseswere performedwiththesoftwareIBMSPSS
Statistics,(version22.0Armonk,NY,IBMCorp.).
Results
Forty-sixpatientsweredividedintotwogroupsof23,atthe beginningofthestudy,forsurgery;40werenowavailablefor
this late assessment;21 from the bonegraft group and 19
from the non-graft group. Sixpatients were notfound.No
patientwasconvertedintototalkneearthroplastyatthistime.
Demographicdatadidnotshowdifferencesbetweengroups
regardingthemajorityofpossiblevariables,suchasage,body massindex(BMI),wedgesizeofthewedgeplateusedtomake thecorrection,presenceofassociatedligamentlesions.There
was agreater number ofsmokersinthe “non-graft”group
(Table1).
The primary outcome,objective KSscale, didnot show any difference betweenthe groups (Table2).KS functional scale did not show any differences between the groups either.
Limbalignmentinthefrontalplanewasmeasuredbythe femorotibial(FT)angle,insupportingX-rays.Theresultsare illustratedinFig.2.Therewasnodifferenceintheincidenceof correctionlossinthenon-graftgroup,asshownbythevalues obtainedinthefinalsegment(p=1.0).
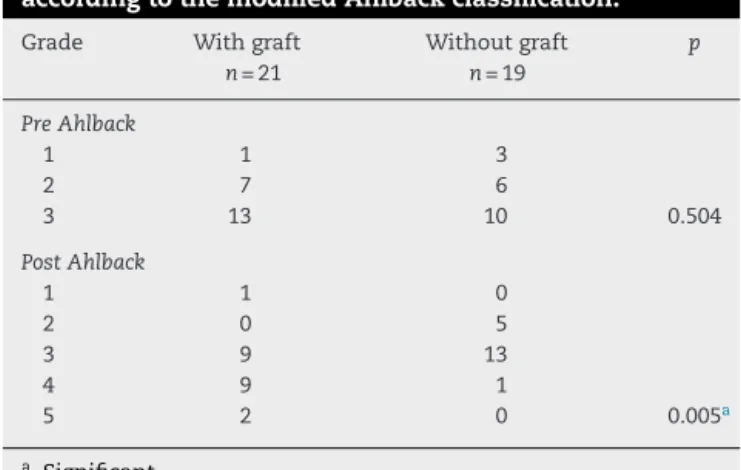
Table3showstheradiographicevolutionofosteoarthritis, accordingtothemodifiedAhlbackclassification.Thegroup “with graft” showed significant aggravation after surgery (p=0.005).
+ 7,5º + − 3,0
+ 5,4º + − 4,1
− 0,9º + − 4,0 neutral
Preop.
Without graft With graft
6m recent
− 4,5º + − 4,9
+ 4º + − 4,6
+ 3,4º + − 4,1
Fig.2–Progressionoftheangleformedbytheanatomical axesoffemurandtibiainradiographswithfrontalplane support.
Table3–Radiographicprogressionofosteoarthritis accordingtothemodifiedAhlbackclassification.
Grade Withgraft n=21
Withoutgraft n=19
p
PreAhlback
1 1 3
2 7 6
3 13 10 0.504
PostAhlback
1 1 0
2 0 5
3 9 13
4 9 1
5 2 0 0.005a
a Significant.
Discussion
Theresultofthisstudyshowedthattheadditionofautologous bonegraftoftheiliaccrestdidnotimprovethelateclinical outcomeofPudduosteotomiesanddidnotincreasetherisk ofcomplications,suchaslossofcorrectionandradiographic deteriorationofosteoarthritisofthekneewhencorrectionsof upto12.5mmareperformed.Inapreviouspaper,6thisteam hadalreadydemonstratedthelackofbenefitsinaddingthis typeofgraftforthehealingoftheosteotomy,buttherewas doubtaboutthepossibilityofcomplicationsorpooroutcome inalong-termfollow-up.
This finding is consistent with biological reasoning, becausethemetaphysealbone,contrarytocommonnotion, doesnotneedfullcontactifthereisrigidstability.16 Thisis achievedbymaintainingtheintegrityofthelateraltibial cor-tex,whichfunctionsasafulcrum,fromwhichformationof endostealcallustakesplace,whichprogressestothemedial sideoftheosteotomy.6,9,17
A recent systematic review with a meta-analysis that included25studiescorroboratesthisfinding.18However,the authorswarnaboutthefactthatonlyoneofthesestudies6has agrade1levelofevidence.Alltheother24arecaseseriesor
non-controlledcomparativestudies.Therefore,thereisaneed formoregoodqualityclinicalstudiestoclarifythesubject.
RegardingtheKSSscale,theposthocanalysisof statisti-calpowershowedthatthesamplesizeissufficienttodetect differencesof20pointsamongthemeans.Thereissome con-troversyoverthe valueoftheMinimalClinicallyImportant Difference(MCID)forthisscale.Althoughsomesmall differ-encessuchas5.9forobjectiveKS,and6.4forfunctionalKS havealreadybeencalculated,19anotherstudyindicatesthat theMCIDforKS-FSshouldbe34.5.20Wesubjectivelyadopted MCID as 20 in this study because we considered that the justificationforapainfulprocedure,suchastheremovalof autologousgraftfromtheiliaccrest,wouldrequireagreater effect(effectsize).InthissamplewefindalowCohen coeffi-cient(d=0.14).Thus,wethoughtthatalargersamplemight havesomescientificvaluebutnoclinicalapplicability.
Regarding the loss ofcorrection,we observedthat both groupshadprogressivelossofthecorrectionobtainedwith six monthsofsurgery inthis follow-up ofmorethan four yearsofduration,butthelosswasequalinbothgroups.As theevaluationswerealldoneonmonopodalweight-bearing radiographs,wedidnottakethemeasurementsonthe radio-graphsmadeimmediatelyafterthesurgery,whichhadtobe donewithoutweight-bearing,duetothepainandinabilityof thepatientstobeartheirweightatthatstage.Thus,itisnot possibletosayiftherewasalossintheperiodbetweensurgery andconsolidation.Thecorrectionangleinthefrontalplane, inthelong-termfinalevaluationofourstudy,issimilartothat reportedbyotherauthorsandiswithintherecommended tar-get(threetosixdegreesofvalgusbetweentheanatomicalaxes ofthefemurandthetibia).21
Regardingosteoarthritis,itisdifficulttofindabiological explanationforthemoremarkedprogressioninthe“graft” group.BecausethemodifiedAhlbackclassificationconsiders thesizeoftheposteriortibialosteophyteintheprofile radio-graphy,itcanbearguedthatthegraftmaysomehowstimulate osteophytegrowth,buttherearenodataintheliteratureto provethistheory.Anotherpossibleexplanationisthatsome hidden uncontrolled variable in this study hascaused this phenomenon.
Themainlimitationsofthis studyweretheinclusionof patientswithchronicligamentlesionsassociatedwithknee varusdeformity,alongwithpatientswithprimary osteoarthri-tis withastableknee, whichmay interferewiththeresult ofclinicalscales andsamplesize,whichwascalculatedfor theoutcomeofosteotomyconsolidation.However,sincethe requirementsfortheindicationofPudduosteotomyaremany, itisdifficulttoobtainasufficientsampleiftheinclusion crite-riainthestudyarefurtherrestricted.
Thisstudysupportstheideathat, inPudduosteotomies with anopeningof less than orequal to12.5mm, neither autologousbonegraftnorcostlybonesubstitutesoughttobe used.
Conclusion
osteotomy,fixedwithfirst-generationwedgeplates,in correc-tionsofupto12.5mm.Therefore,intheseconditions,weavoid itsusebecauseitisaprocedurethatincreasesthepatient’s painandmorbidity.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. AmendolaA,PanarellaL.Hightibialosteotomyforthe treatmentofunicompartmentalarthritisoftheknee.Orthop ClinNorthAm.2005;36(4):497–504.
2. BrinkmanJ-M,LobenhofferP,AgneskirchnerJD,StaubliAE, WymengaAB,vanHeerwaardenRJ.Osteotomiesaroundthe knee:patientselection,stabilityoffixationandbonehealing inhightibialosteotomies.JBoneJointSurgBr.
2008;90(12):1548–57.
3. HernigouP,MedevielleD,DebeyreJ,GoutallierD.Proximal tibialosteotomyforosteoarthritiswithvarusdeformity.Aten tothirteen-yearfollow-upstudy.JBoneJointSurgAm. 1987;69(3):332–54.
4. NoyesFR,MayfieldW,Barber-WestinSD,AlbrightJC, HeckmannTP.Openingwedgehightibialosteotomy:an operativetechniqueandrehabilitationprogramtodecrease complicationsandpromoteearlyunionandfunction.AmJ SportsMed.2006;34(8):1262–73.
5. DeLongWG,EinhornTA,KovalK,McKeeM,SmithW, SandersR,etal.Bonegraftsandbonegraftsubstitutesin orthopaedictraumasurgery.Acriticalanalysis.JBoneJoint SurgAm.2007;89(3):649–58.
6. ZorziAR,daSilvaHGPV,MuszkatC,MarquesLC,CliquetA,de MirandaJB.Opening-wedgehightibialosteotomywithand withoutbonegraft.ArtifOrg.2011;35(3):301–7.
7. DugdaleTW,NoyesFR,StyerD.Preoperativeplanningfor hightibialosteotomy:theeffectoflateraltibiofemoral separationandtibiofemorallength.ClinOrthopRelatRes. 1992;274(3):248–384.
8. GolovakhaML,OrljanskiW,BenedettoKP,PanchenkoS, BüchlerP,HenleP,etal.Comparisonoftheoreticalfixation stabilityofthreedevicesemployedinmedialopeningwedge hightibialosteotomy:afiniteelementanalysis.BMC MusculoskeletDisord.2014;15(1):230.
9.StaubliAE,JacobHA.Evolutionofopen-wedgehigh-tibial osteotomy:experiencewithaspecialangularstabledevice forinternalfixationwithoutinterpositionmaterial.Int Orthop.2010;34(2):167–72.
10.ZorziAR,ImamuraTF,PiedadeSR,MirandaJB.Osteotomia valgizantedatibiaproximalcomcunhaabertamedial. OrtopediaeTraumatologiaIlustrada.2011;2(3):79–86. 11.WadeR,RichardsonJ.Outcomeinfracturehealing:areview.
Injury.2001;32(2):109–14.
12.InsallJN,DorrLD,ScottRD,ScottWN.RationaleoftheKnee Societyclinicalratingsystem.ClinOrthopRelatRes. 1989;(248):13–4.
13.SpecognaAV,BirminghamTB,HuntMA,JonesIC,JenkynTR, FowlerPJ,etal.Radiographicmeasuresofkneealignmentin patientswithvarusgonarthrosis:effectofweightbearing statusandassociationswithdynamicjointload.AmJSports Med.2007;35(1):65–70.
14.SpecognaAV,BirminghamTB,DaSilvaJJ,MilnerJS,KerrJ, HuntMA,etal.Reliabilityoflowerlimbfrontalplane alignmentmeasurementsusingplainradiographsand digitizedimages.JKneeSurg.2004;17(4):203–10.
15.KeyesGW,CarrAJ,MillerRK,GoodfellowJW.Theradiographic classificationofmedialgonarthrosis.Correlationwith operationmethodsin200knees.ActaOrthopScand. 1992;63(5):497–501.
16.GiannoudisPV,EinhornTA,MarshD.Fracturehealing:the diamondconcept.Injury.2007;38Suppl4:S3–6.
17.StaubliAE,DeSimoniC,BabstR,LobenhofferP.TomoFix:a newLCP-conceptforopenwedgeosteotomyofthemedial proximaltibia–earlyresultsin92cases.Injury.2003;34 Suppl.2:B55–62.
18.HanJH,KimHJ,SongJG,YangJH,BhandareNN,Fernandez AR,etal.Isbonegraftingnecessaryinopeningwedgehigh tibialosteotomy?Ameta-analysisofradiologicaloutcomes. KneeSurgRelatRes.2015;27(4):207–20.
19.LeeWC,KwanYH,ChongHC,YeoSJ.Theminimalclinically importantdifferenceforKneeSocietyClinicalRatingSystem aftertotalkneearthroplastyforprimaryosteoarthritis.Knee SurgSportsTraumatolArthrosc.2016.Epubaheadofprint. 20.JacobsCA,ChristensenCP.Correlationsbetweenkneesociety
functionscoresandfunctionalforcemeasures.ClinOrthop RelatRes.2009;467(9):2414–9.
21.PipinoG,IndelliPF,TiganiD,MaffeiG,VaccarisiD.