Revista da Sociedade Brasileira de Medicina Tropical 2 1 ( 3 ) : 1 2 3 - 1 2 9
,
J u l- S e t, 1 9 8 8 .M ALAR IA IN H U M A IT A CO U NT Y , STATE O F A M A Z O N A S , BRAZIL.
X I X - EV A LU A T IO N O F CLIN DA M Y C IN F O R TH E TR EA TM EN T OF
PA TIEN TS W ITH
P L A S M O D I U M F A L C I P A R U M
IN FE C T IO N
D o m i n g o s A lv e s M e i r a 1 , P a u lo C a m a r a M a r q u e s P e r e i r a 1 , J u s s a r a M a r c o n d e s - M a c h a d o 1 , R in a id o P o n c io M e n d e s 1 , B e n e d it o B a r r a v ie r a 1 , J o s é A n t o n io G . P ir o la 1 ,
M a r ia R e g in a C o t r im G u i m a r ã e s 1 , P a u lo R o b e r to C u r i
2
a n d R e n a t o P e d r o R o d r i g u e s 1 .A total o f 207 patients with malaria caused by Plasmodium falciparum were subm itted to 5 different treatment schedules with clindamycin fro m 1981 to 1984: A -89 patients were treated intravenously and orally, or intramuscularly and orally with 20 m g/kg/day divided into two daily applications fo r 5 to 7 days; B - 4 0 patients were treated orally with 20 m g/kg/day divided into two daily doses fo r 5 to 7 days; C - 2 7 p a tients were treated with 20 m g/kg/day intravenously or orally divided into two daily applications fo r 3 days; D - 1 6 patients were treated orally and/or intravenously with a single daily dose o f 20 to 40 m g/kg/day fo r 5 to 7 days; E - 35 patients were treated orally with 5 m g/kg/day divided into two doses fo r 5 days. Patients were examined daily during treatment and reexamined on the 7th, 24th, 21st, 28th and 35th day both clinically and parasitologically (blood test). Eighty three (40.1% ) had moderate or severe malaria,
and 97 (46.8% ) had shown resistance to chloroquine or to the combination ofsulfadoxin and pyrimethamine. The proportion o f cured patients was higher than 95% am ong p a tients subm itted to schedules A a n d B . Side effects were only occasional and o f low inten sity. Three deaths occurred (1.4%), two o f them involving patients whose signs and sym ptom s were already very severe when treatment was started. Thus, clindamycin proved to be very useful in the treatment o f patients with malaria caused by Plasmodium falciparum and we recommend schedule A fo r moderate and severe cases and B fo r initial cases.
Key-words: Malaria treatment. Plasmodium falciparum . Clindamycin.
Since the first report by Silva et al?1 in 1961 of the occurrence of Plasm odium falciparum resis tance to chloroquine in Brazil, this phenomenon has shown a tendency to increase2 4 5. The increase in number of rcsistnntPlasmodium falciparum strains to multiple drugs has reopened the question of the need to reevaluate the use of antibiotics in the treatment of malaria10 25 27. The search for new options in the treatment of severe malaria caused by Plasmodium falciparum has gained growing importance with the progressive increase of cases recorded since 19701518.
1. Departamento de Moléstias Infecciosas e Parasitárias, Dermatologia e Radiologia, Faculdade de Medicina, Cam pus de Botucatu - U NESP.
2. Departamento de Cirurgia, Faculdade de Medicina, Campus de Botucatu - UNESP.
Correspondence to: Domingos Alves M eira - Departamento de Moléstias Infecciosas e Parasitárias, Dermatologia e Ra diologia - Faculdade de Medicina de Botucatu - U N ESP - Caixa Postal 522 - 18610 - Botucatu - São Paulo - Brasil. Recebido para publicação em 14/12/87
Among the antibiotics used, special attention has been given to halogenate lincomycin derivati ves16 1 7 2 6 2 8 2 9 aiMj t o clindamycin13 7 8 2 2 2 4 2 8 ^ which have shown promise.
In a previous study24, we demonstrated the efficacy of clindamycin as the single antimalarial drug used in the treatment of patients infected with Plas modium falciparum . However, several points con cerning malaria treatment with clindamycin have not yet been fully elucidated. Among them, especially important are the slow elimination of parasitemia3 7 24 28 the repercussions of the severity of the disease and the relationship with patient origin21, i. e. whether or not the patient is from a natural endemic region.
M eira DA, Pereira PCM, Marcondes-Machado J, M endes RP, Barraviera B, Pirola JAG, Guimarães M RC , Curi PR, Rodrigues RP. M alaria in H um aita county, State o f Amazonas, Brazil. X IX -E v a lu a tio n o f clindamycin fo r the treatment o f patients with Plasmodium falciparum infection. Revista da Sociedade Brasileira de M edicina Tropical 21:123-129, Jul-Set, 1988
CASES A N D M ETHOD S
Sixty one, 97, 42 and 7 patients infected with Plasmodium falciparum were studied in the summers of 1981, 1982 and 1983 and in the winter of 1984, respectively. From 1981 to 1983, these patients were seen at the State of Amazonas Health Department Hospital and at the Outpatient Clinic of SUCAM, in Humaita, State o f Amazonas, Brazil, and in 1984 at the “Presidente Medici” Hospital, State of Rondonia, Brazil. Etiologic diagnosis of malaria and parasitemia counts were performed by the classical method23. All patients were submitted to complete clinical exami nation including epidemiologic data, physical exami nation and laboratory tests, before and after treatment, using a standard file card. Laboratory tests included hemogram, urinalysis, feces parasitology, and elec trocardiogram. Patients were classified according to severity of the disease, presence of associated disease, origin and previous plasmodium resistance to chlo- roquine and/or to treatment with combined sulfadoxin and pyrimethamine. The severity of the disease was determined by clinical and parasitologic parameters considering not only the intensity of asexual parasi temia, but also the presence or abscence of gametocy- tes19 20. W ith respect to origin, patients were divided into two groups: Amazonians, i.e. subjects bom in the Amazon Region, and non-Amazonians, i.e., migrants from other regions of the country who contracted the disease in Amazonia.
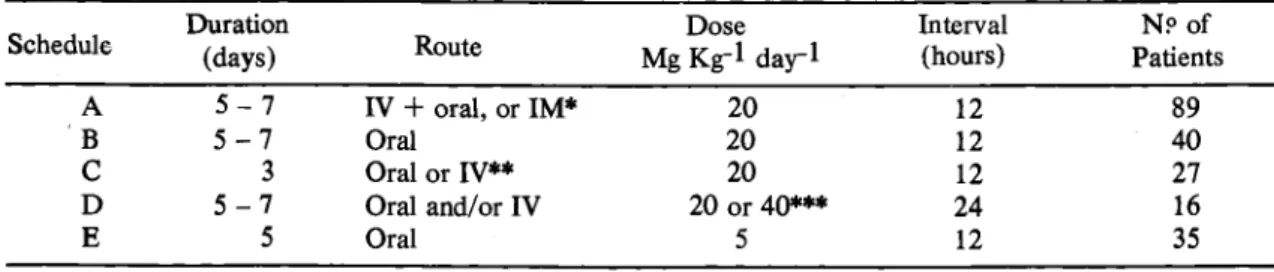
Table 1 shows the treatment schedules used for clindamycin. In schedules A, B and D , treatment lasted 7 days when important clinical manifestations still persisted or asexual parasitemia was positive on the 5th day. In schedules A, C and D, clindamycin was diluted in 150 ml of 5% glucose solution and admi nistered intravenously dropwise for 30 minutes. In schedule A, the oral route was usually utilized during the final period of treatment when the patient had improved and asexual parasitemia had decreased.
Table 2 shows patient distribution by age range and sex according to the treatment schedules used. One hundred and twenty six patients (61.2%) were white and 81 (39,8% ) nonwhite. The professions linked to exposure to infection were predominant, i.e., 105 (73.4%) of the 143 patients with a declared profession were laborers, rubber tree tappers, topo graphers and prospectors for gold and precious stones.
The roads that cross the region and which correspond to the areas of greatest transmission of malaria18 were reported as the probable site of con tagion by 168 patients (81.1%) who lived or worked there, while 18 patients (8.7%) were infected in Rondonia and 21 (10.2%) at indeterminate sites.
All patients were examinated daily and tested for parasitemia during treatment. These procedures were repeated up to the 7th day in 34 patients, and in 170 of them were also performed on the 14th (N = 54), 21st (N = 77), 28th (N = 34) and 35th (N = 5) day. These tests were repeated up to the day of death in the 3 fatal cases.
Cure was considered to have occurred when remission of clinical manifestations was observed, when asexual parasitemia was negative during the 7 days following the beginning of treatment and conti nued to be negative on the occasion of delayed controls.
The possible side effects attribuable to treat ment were observed.
Statistical Analysis
D ata were analyzed statistically by the X 2 test, by comparing the rates of success, and by the non- parametric test of Friedman11 14.
RESULTS
Analysis of the results showed a strong associa tion between treatment schedule and age range (p <
Table 1 -D istribution o f 2 0 7 patients infected with Plasmodium falciparum according to the schedule o f clin damycin treatment used
Schedule Duration(days) Route Mg Kg"l d a y lDose Interval(hours) PatientsN ? of
A 5 - 7 IV + oral, or IM* 20 12 89
B 5 - 7 Oral 20 12 40
C 3 Oral or IV** 20 12 27
D 5 - 7 Oral and/or IV 20 or 40*** 24 16
E 5 Oral 5 12 35
* S e v e n p a tie n ts w e re tre a te d I.M .;
** 2 0 p a tie n ts w ere tre a te d w ith c h lo ro q u in e c o m b in e d w ith c lin d a m y cin a t th e d o se o f 10 m g/kg, IM , o n th e 1s t d a y a n d a t th e d o se o f 7 m g k g '1 d a y '1 o n th e 2 ntl a n d 3 rc* d a y s b y th e o ra l ro u te a t 12 interv als;
*** 3 p a tie n ts re c eiv ed 4 0 m g kg"1 d a y -1 IV .
M e ira D A , P ereira P C M, M a r c o n d e s -M a c h a d o J, M e n d e s R P , B a rra v ie r a B , P ir o la J A G , G u im a r ã e s M R C , C u ri P R , R o d rig u e s R P . M a la r ia in H u m a ita co u nty, S ta te o fA m a z o n a s , B ra zil. X I X — E v a lu a tio n o fc lin d a m y c in f o r the tre a tm e n t o f p a tie n ts with P la sm o d iu m falc ip a ru m in fectio n . R e v is ta d a S o c ie d a d e B ra sileira d e M e d ic in a T r o p ic a l 2 1 : 1 2 3 - 1 2 9 , J u l-S e t, 1 9 8 8
T able 2 - D i s t r i b u t i o n o f p a t i e n t s w ith m a la r ia c a u s e d b y Plasm odium falciparum a c c o r d in g to a g e ra n g e s e x a n d tr e a tm e n t s c h e d u le
T reatm ent Schedule
Age Range
(years) Total
Sex
0 > 5 5 > 15 ( > 1 5 M ales F em ales
A 6 (0.07) 1 7 (0 .1 9 ) 66 (0.74) 89 75 (0.84) 1 4 (0 .1 6 )
B 12 (0.30) 1 4 (0 .3 5 ) 1 4 (0 .3 5 ) 40 33 (0.83) 7 (0 .1 7 )
C 0. (0.00) 0 (0.00) 2 7 (1 .0 0 ) 27 24 (0.89) 3 (0 .1 1 )
D 9 (0.56) 5 (0 .3 1 ) 2 (0 .1 3 ) 67 7 (0.44) 9 (0 .5 6 )
E 1 (0.03) 5 (0 .1 4 ) 29 (0.83) 35 29 (0.83) 6 (0.17)
T otal 28 (0.13) 41 (0.20) 1 3 8 (0 .6 7 ) 207 168 (0.81) 39 (0.19)
(A g e R an ge) X . = 7 0 .6 2 9 p < 0.001 c = 0.59
X ^ = 16.416 p < 0 .0 1 ( S e x ) c = 0.28
0.001; C = 0.59), with patients older than 15 years predominating in schedules A and E . In schedule B, all age ranges were equally distributed. A l l patients in schedule C were 15 years old or more. Finally, children predom inated in schedule D .
The association betw een patient sex and trea tm ent schedule was weak, since males predom inated in all schedules except schedule D , in which sex distribu tion was identical.
T able 3 shows that patients classified by clin dam ycin treatm ent schedule and by previous resis tance o f P la s m o d iu m f a lc ip a r u m to classical antim a- larial drugs, i. e., to chloioquine and to the combina tion of sulfadoxine and pyrim etham ine did n o t differ in distribution am ong the various treatm ent schedules. It should be em phasized th at 97 (46.8% ) patients were infected with a resistant plasm odium strain, 81 o f them (39.1% ) a t the Rj level and 16 (7.7% ) a t the R n and R m levels.
A nalysis of the results presented in T able 4 reveals that patient distribution by severity of the disease differed am ong the various treatm ent sche dules, with m ost m oderately and seriously ill patients being included in schedules A , B a n d D . In schedule A , 5 patients had the cerebral form o f the disease, 1 had acute renal failure, 2 showed peripheral failure and very intensive m alarial attacks, and 3 had jaundice. A m ong the patients in schedule B there was a one- month old baby, who probably had the congenital form of the disease. Among the patients in schedule D there was a large proportion o f subjects with the m oderate or severe form, including one with the cerebral form and another with jaundice, even though this group consis ted o f a small num ber o f patients. T he highest pro portion o f benign forms ocurred among patients in schedule E .
Table 5 shows distribution by region of origin with respect to the result obtained with each schedule of clindam ycin treatm ent. N o difference in patient proportion in each o f the schedules used was detected w hen A m azonians were com pared with individuals coming from other regions o f the country. A nalysis of the results also showed th at the proportion of cured subjects was statistically higher in schedules A and B. It should be pointed o u t th at 86 o f 89 patients (96.6% ) were cured in schedule A , and 39 o f 40 (97.5% ) were cured in schedule B. The proportion of cured subjects was lower in the remaining schedules, i.e. 80.0% for E , 70.4% for C and 50.0% for D .
The occurrence of negative asexual parasitem ia differed when the various clindam ycin schedules were compared. Statistically significant differences were observed only on the occasion o f the delayed controls performed between the 14th and 35th days (H = 38.241; p < 0.001) when parasitem ia was found to be negative only among patients subm itted to treatm ent schedules A and B. Positive asexual parasitem ia was detected in growing proportions among patients submitted to treatm ent schedules E , C and D , indicating that treatm ent failure occurred in these groups.
E ight of the 27 patients who were not cured by the treatm ent received were subm itted to further treatm ent with clindamycin. Three o f them had been subm itted io schedule C , 2 to schedule E and 1 to schedule B. A fter further treatm ent, 4 patients were cured by schedule A , 2 by schedule B, and one by schedule D . T here was only one case o f treatm ent failure concerning a patient resubm itted to treatm ent schedule D .
M e i r a DA, P e r e i r a P C M , M a r c o n d e s -M a c h a d o J, M e n d e s R P , B a rra v ie r a B, P ir o la J A G , G u im a r ã e s M R C , C u ri P R ,
R o d rig u e s R P . M a la r ia in H u m a ita c o u nty, S ta te o f A m a z o n a s , B r a z il. X I X - E v a lu a tio n o f c lin d a m y c in f o r th e tr e a tm e n t o f p a tie n ts with P la sm o d iu m fa lcip aru m in fection. R e v is ta d a S o c ie d a d e B ra sile ira d e M e d ic in a T r o p ic a l 2 1 : 1 2 3 - 1 2 9 , J u l-S e t,
1 9 8 8
T able 3 -P a tie n t d is tr ib u tio n a c c o r d in g to sc h e d u le o f tr e a tm e n t w ith c lin d a m y c in a n d p r e v io u s r e s is ta n c e to c la s s ic a l a n tim a la r ia l d ru g s.
T reatm ent Previous Resistance
Schedule R j R j i + R m Other* Total R i + R n + R m
A. 3 2 (3 4 .8 3 ) 9 (6.88) 48 (4 6 .2 9 ) 89 0.46
B 1 6 (1 5 .6 5 ) 1 (3.09) 23 (21.26) 40 0.43
C 1 0 (1 0 .5 7 ) 2 (2.09) 1 5 (1 4 .3 4 ) 27 0.44
D 9 ( 6.26) 2 (1 .2 4 ) 5 ( 8.50) 16 0.69
E 1 4 (1 3 .7 0 ) 2 (2 .7 1 ) 1 9 (1 8 .5 9 ) 35 0.46
T otal 81 16 110 207 0.47
* Sensitive o r n o t tre a te d p re v io u sly p > 0 .5 0 X ^ - 5 .8 3 1
T able 4 - P a t i e n t d is tr ib u tio n a c c o r d in g to s c h e d u le o f tr e a tm e n t w ith c lin d a m y c in a n d s e v e r ity o f th e c lin ic a l f o r m o f th e d is e a s e
T reatm ent Schedule
Clinical form
Total Proportion of
M oderate + Severe M ild M oderate + Severe
A 4 0 (5 3 .3 1 ) 4 9 (3 5 .6 9 ) 89 0.55
B 28 (23.96) 1 2 (1 6 .0 4 ) 40 0.30
C 2 0 (1 6 .1 7 ) 7 10.83) 27 0.26
D 7 ( 9.58) 9 ( 6.42) 16 0.56
E 29 (20.97) 6 (1 4 .0 3 ) 35 0.17
Total 124 83 207
x \ = 2 1 .6 5 0 p < 0 . 0 0 1 c = 0 .3 2
T able 5 - P a tie n t d is tr ib u tio n a c c o rd in g to o rig in a n d re s u lt o f tr e a tm e n t w ith th e d iffe re n t c lin d a m y c in sc h e d u le s
A m azonians (A m ) N on-A m azoninans (N A m )
G eneral T otal T reatm ent
Schedule
Total
Cured
Total
Cured
Np Proportion Np Proportion
A 48 47 0.9792 41 39 0.9512 89
B 33 32 0.9697 7 7 1.0000 40
C 14 9 0.6429 13 10 0.7692 27
D 11 5 0.4545 5 3 0.60000 16
E 21 16 0.7619 14 12 0.8571 35
Total 127 109 0.8583 80 71 0.8875 207
Proportion o f cured: A m X N A m X 2 = 1 .3 7 8 ; p > 0 .8 0 A m = N A m
A x B x C x D x E X 2 = 3 8 .5 7 1 ; p < 0 .0 0 1 ( A = B ) > E > C > D
M e ir a D A , P ereira P C M , M a r c o n d e s -M a c h a d o J, M e n d e s R P , B a rra v ie r a B , P ir o la J A G , G u im a r ã e s M R C , C u r i P R , R o d rig u e s R P . M a la r ia in H u m a ita cou n ty, S ta te o f A m a z o n a s , B r a z il. X I X - E v a lu a tio n o f c lin d a m y c in fo r the tre a tm e n t o f p a tie n ts with P la sm o d iu m fa lcip aru m in fection . R e v is ta d a S o c ie d a d e B ra sileira d e M e d ic in a T r o p ic a l 2 1 : 1 2 3 - 1 2 9 , J u l-S e t,
1 9 8 8
schedule C; vomiting in 2 patients treated with sche dule B , and pain at the site o f injection in 2 submitted to schedule A by the intram uscular route. In none of these cases, how ever, was it necessary to discontinue treatment.
T hree patients (1.4% ) died during treatment. Two o f them were in serious condition at the time o f diagnosis. O f these, one was a 4-year old A m azonian child who had been ill for 3 days and had the cerebral form o f fulminating evolution. This child had suffered convulsions lasting 7 hours before treatm ent was started and was in a coma. She was submitted to schedule D for 2 days, b u t showed no im provem ent before she died. T he second was a 31-year old non- A m azonian male who had become ill 6 days before treatm ent was started and who was in acute renal failure. This patient was subm itted to schedule A for 5 days. Even though asexual parasitem ia was apprecia bly reduced by clindamycin, this patient developed acute renal failure and anuria up to his death which occurred on the 5th day of treatm ent. I t was not possible to tre a t his acute renal faillure because o f the lack of facilities for dialysis treatm ent a t H um aita at the time, and because transfer to another hospital in Porto Velho or in M anaus could not be arranged. The third was a 2-year old A m azonian child who had suffered a previous m alarial attack caused by P l a s
m o d iu m f a lc ip a r u m resistant (Rj) to chloroquine and
who showed the m oderate form of the disease a t the time o f diagnosis. This patient was initially treated by schedule B. O n the third day he becam e worse and fell into a coma. T he clindam ycin route was changed to the intravenous mode ( schedule A ) b u t the child continued in a com a and died on the fifth day.
D IS C U S S IO N
Clindam ycin (7-(S)-chloro-7-deoxylincomy- cin) has been extensively studied as an antibiotic indicated for the treatm ent of serious infections. This drug is active against G ram -positive aerobic bacteria and very active against G ram -positive and negative anaerobic bacteria. Clindam ycin inhibits bacterial protein synthesis and has both a bactericidal and bacteriostatic action. Experim ental and clinical stu dies have dem onstrated its activity in the treatm ent of hum an and anim al m alaria caused by resistant strains of P la s m o d iu m f a l c i p a r u m1 3 7 8 9 16 17 2 2 2 4 2 6 2 8 2 9
The present search for an ideal schedule for the treatm ent o f m alaria caused by P la s m o d iu m f a l c i
p a r u m using clindamycin as the sole antim alarial drug
was m otivated by the effectiveness of this treatment, taking into account some still no fully elucidated factors such as patient origin, severity o f clinical form, previous resistance o f the plasm odium to classical antim alarial drugs, and the tim e needed for asexual parasitem ia to become negative. The treatm ent sche dules used here differed in duration, administration
route, dose, and interval betw een doses. In this respect, schedule B differed from schedule A only in terms o f adm inistration route, which was exclusively oral in B.
Schedule C had the longest interval betw een doses, and schedule E the shortest dose. Thus, the patients were n ot assigned to a treatm ent schedule at random but on the basis o f criteria including severity of clinical form, absence of asexual parasitem ia1920, and the easier adm inistration o f the drug to children by the oral route. T his m ay explain the variation observed among the various treatm ent schedules and some preliminary factors such as age group, sex and severity of the disease. H owever, there was no difference among treatm ent groups in terms of previous resis tance to classical antim alarial drugs since the propor tions of the different levels of resistance were the same in each group. T he proportion of previous resistance to classical antim alarial drugs was higher than that reported by A lecrim et al3 and Rivera et al28.
Schedule A included the largest num ber of patients with the severe form o f the disease and with higher asexual parasitem ia and therefore was the schedule o f longest duration, o f shortest interval betw een doses and o f m ost prolonged intravenous clindam ycin adm inistration. Schedules D and B fol lowed A in terms o f proportion of severe forms o f the disease, while schedule E included the largest num ber of benign cases. Indeed, the low est clindamycin dose was used in schedule E .
The same proportion o f therapeutic efficacy was observed among non-A m azonians and A m azo- nians in all treatm ent schedules used. Thus, clinda mycin did n o t perform differently with respect to patient origin, though a difference m ay exist betw een patient origin and predisposition to m alaria21. The highest cure rates (> 95.0% ) occurred among patients treated with schedules A and B, and it should be emphasized th a t these grups included m ost o f the patients with severe forms o f m alaria. These results agree with those reported by A lecrim et a ll, C abrera et al7 and Rivera et al28, who used intravenously adm inistered clindamycin for 5 to 7 days at the dose of 20 m g/kg/day with 12-hour intervals betw een doses.
Patients treated with schedule E had lower cure rates (80.0% ), b ut the low est rates were observed among those on schedules C (70.3% ) and D (50.0% ).
It should be pointed out th at asexual parasitem ia was negative on the occasion o f delayed controls only in patients treated with schedules A or B.
M e ir a D A , P ereira P C M , M a r c o n d e s -M a c h a d o J, M e n d e s R P , B a rra v ie r a B , P ir o la J A G , G u im a r ã e s M R C , C u r i P R , R o d rig u e s R P . M a la r ia in H u m a ita c o u n ty, S ta te o f A m a z o n a s , B r a z il. X I X - E v a lu a tio n o fc lin d a m y c in fo r the tre a tm e n t o f p a tie n ts withP la sm od iu m falciparum in fection . R e v is ta d a S o c ie d a d e B ra sile ira d e M e d ic in a T r o p ic a l 2 1 : 1 2 3 - 1 2 9 , J u l-S e t,
1 9 8 8
Clindam ycin seems to ac t on P la s m o d iu m
f a lc ip a r u m b y inhibiting m itochondrial function or
synthesis12 13. O n the other hand, in vitro results reported by Seaberg et al30 suggest that the inhibition
o f P la s m o d iu m f a lc ip a r u m growth depends on time of
parasite exposure to clindamycin, so th at for 90.0 to 9 5.0% inhibition to occur, 72 hours of exposure to the drug are needed. In the present study the duration o f treatm ent in the m ost effective schedules (A and B) agrees with d ata reported by Seaberg et al30 and should not be considered as a factor discouraging the choice o f this antibiotic.
Side effects occurred only occasionally and were o f low intensity, so that treatm ent did not have to be discontinued in any case, as also reported by other authors3 7 N o n e of the patients treated with clindamycin showed symptoms o f the pseudomem branous colitis associated with C lo s tr id iu m d iffic ile6.
E ven though the three fatal cases were reported as treatm ent failures for d ata analysis purpose, it should be pointed out that two o f these patients were started on clindam ycin when their condition was already very serious. O ne o f them was in a coma and had been suffering generalized convulsions for more than 7 hours, and another showed acute renal failure and anuria, with local conditions not permitting dialy sis. Both patients were first seen when they were in a pre-agonic and irreversible condition.
Finally, the present results perm it us to suggest that clindamycin can be indicated for the treatm ent of patients with m alaria caused b y P la s m o d iu m f a l c i
p a r u m resistant to classical antim alarial drugs. The
following two treatm ent schedules are recommended: 20 m g/kg/day oral clindam ycin divided into two doses at 12-hour intervals for 5 to 7 days for benign cases, and 20 m g/kg/day in two daily applications at 12-hour intervals by the intravenous or intram uscular route for 5 to 7 days for m oderate and severe cases.
R E S U M O
D e 1981 a 1984, 207 doentes com m alária, causada pelo P la s m o d iu m f a lc ip a r u m , foram tratados com 5 esquem as de clindamicina: A - 89 doente tratados com 20 m g/kg/dia, pelas vias endovenosa e oral, ou intram uscular e oral, em duas aplicações diárias, durante 5 a 7 dias; B - 40 doentes tratados com 20 mg/kg/dia, por via oral, em duas tom adas diárias, durante 5 a 7 dias; C - 27 doentes tratados com 20 m g/kg/dia, por via oral ou endovenosa, em duas tom adas diárias, durante 3 dias; D - 16 doentes tratados com 20 a 40 m g/kg/dia, por vias oral, e/ou, endovenosa, em um a única dose diária, durante 5 a 7 dias; E - 35 doentes tratados com 5 m g/kg/dia, por via oral, em duas doses diárias, durante 5 dias. O s doentes foram examinados, diariamente, durante o tratamento e reexam inados no 7.°, 14.°, 28.° e 35.° dias, tanto pelo
exam e clínico, quanto pelo parasitológico de sangue. O itenta e três (40,1% ) tinham m alária m oderada ou grave e 97 (46,8% ) tinham apresentado resistência à cloroquina, ou à associação sulfadoxina e pirim eta- mina. Os resultados m ostraram que a proporção de curados foi superior a 95% nos doentes tratados pelos esquemas A e B. O s efeitos colaterais observados foram ocasionais e de pequena intensidade. H ouve três casos de óbito (1,4% ), dois dos quais atendidos desde o inicio com quadro m uito grave. A clindam icina: portanto, m ostrou ser muito útil no tratam ento de doentes com m alária causada pelo P la s m o d iu m f a l
c ipa ru m ', recom enda-se o esquem a A p a ra os casos
moderados e o B para os benignos.
P a la v r a s - c h a v e s : T ratam ento da m alária. P l a s
m o d iu m f a lc ip a r u m . Clindamicina.
A C K N O W L E D G E M E N T S
W e wish to thank “ F undação Projeto R ondon” , the D irectory o f the A dvanced Cam pus, and H um aita SU C A M .
R E F E R E N C E S
1. A le cr im M G , D o u ra d o H , A le cr im W , A lbuqu erqu e
B C , W a n s sa E , W a n s sa M C T ratam en to d a m a la ria (P. f a lc ip a r u m )co m clin d am icin a. R e v ista d o In stituto d e
M ed ic in a T rop ical de S ã o P a u lo 23: 8 6 - 9 1 , 1 9 8 1 . 2 . A le cr im M G C , A le cr im W D , A lb u q u erq u e B C de,
D o u ra d o H V , W a n s sa M C . R e sistê n c ia “ in v iv o ” do P la s m o d iu m fa lc ip a r u m à a ss o c ia ç ã o su lfa m eto x a zo l m ais trim etoprin n a A m a z ô n ia B rasileira. R e v ista do In stituto d e M ed ic in a T rop ical d e S ã o P a u lo 24: (S u p l. 6): 4 8 - 5 1 , 1 9 8 2 .
3. A le cr im W D , A lb u q u erq u e B C , A le cr im M G C , D o u rado H . T ratam en to d a m alária (P. fa lc ip a r u m ) c o m clind am icina. II - E sq u e m a p o s o ló g ic o em cin co dias. R e v ista d o In stitu to d e M ed ic in a T rop ical de S ã o P a u lo 2 4 (S u p l. 6): 4 0 - 4 3 , 1 9 8 2 .
4 . A le cr im W D , D o u ra d o H , A le cr im M d a s G , P a sso s L F , W a n s sa E , A lbu qu erqu e B . R e sistê n c ia “ in v iv o ” d o P la s m o d iu m fa lc ip a r u m à a ss o c ia ç ã o su lfad oxina m ais pirim etam in a, a n ível d e R III, n o A m a z o n a s, Brasil. R e v ista d o In stitu to d e M ed ic in a T rop ical d e S ã o P au lo 2 4 (S u p l. 6): 5 2 - 5 3 , 1 9 8 2 .
5. A lm e id a N e t o J C , O liv eir a G S C , S am p aio J A A . R e sistê n c ia do P. fa lc ip a r u mà a ss o c ia ç ã o su lfam ídicos n a região C en tro -O este d o Brasil. D a d o s referentes ao estu d o de 1 0 4 p a cien tes. R e v ista de P a to lo g ia T rop ical de G o iá s 3: 3 8 5 - 3 9 3 . 1 9 7 2 .
6 . B oriello S P . C lo strid iu m d ifficile and g u t d ise a se . In: C S G o o d e (e d ) M icro b es and In fectio u s o f the gut.
S c ien tific P u b lica tio n s. D a te L ate 3 2 7 - 3 4 6 , 1 9 8 3 .
M e i r a D A , P e r e i r a P C M , M a r c o n d e s - M a c h a d o J , M e n d e s R P , B a r r a v i e r a B , P i r o l a J A G , G u i m a r ã e s M R C , C u r i P R , R o d r i g u e s R P , M a l a r i a in H u m a i t a c o u n ty , S t a t e o f A m a z o n a s , B r a z i l . X I X —E v a l u a t i o n o f c l i n d a m y c i n f o r t h e t r e a t m e n t o f p a t i e n t s w ith P la sm od iu m falciparum in f e c tio n . R e v i s t a d a S o c i e d a d e B r a s i l e i r a d e M e d i c i n a T r o p i c a l 2 1 : 1 2 3 - 1 2 9 , J u l - S e t 1 9 8 8
8. C lyd e D F , G ilm ar R H , M c C arthy V C . A n tim alaria l effects o f clin d a m y cin in m an. A m erica n Journal o f T rop ical M e d ic in e and H y g ie n e 24: 3 6 9 - 3 7 0 , 1 9 7 5 . 9 . D e H a a n R M , M e tz le r C M , Schellenb erg D , Van
den-b o sh W D . P h arm acock in etic stu d ies o f clin d am ycin ph osp hate. Journal o f C lin ical P h a r m a co lo g y 1 3 : 1 9 0 -2 0 9 , 1 9 7 3 .
10. D o u r a d o H . T erap êu tic a d a m alária c o m m in ociclin a. R evista B rasileira d e C lín ica e T erap êu tic a 2: 1 0 -1 2 , 1 9 7 3 .
11. F le is s JL . S tatistical m eth od s for rates and proportions. J o h n W ile y & S o n s, N e w York, 1 9 7 3 .
12. G ea r y T G , D iv o A A , J e n se n JB . A n in vitro a ss a y
sy stem fo r th e id en tification o f poten tial antim alarial drugs. Jou rnal o f P ara sito lo g y 6 9 : 5 7 7 - 5 S 3 , 1 9 8 3 . 1 3 . G ea r y T G , J e n se n J B . E ffe c ts o f an tib iotics o n P l a s
m o d iu m f a l c i p a r u m in vitro. A m e ric a n Journal o f T rop ical M ed ic in e an d H y g ie n e 3 2 : 2 2 1 - 2 2 5 , 1 9 8 3 .
14. H o lla n d er M , W o lfe D A . N o n p aram etr ic S tatistical M eth od s. J o h n W ile y & S o n s, N e w York, 1 9 7 3 . 15. I E S - In fo rm a çõ es E p id em io ló g ic a s S U C A M . C a s o s
n otificad os d e m alária por área d e errad icação a lo n g o e curto p razo e por un id ad e. N ? 2 6 , d ezem b ro, 1 9 8 4 . 16. L ew is C . A n tip la sm o d ia l activ ity o f h alogen ate d
lin co m y c in an alogu es in P l a s m o d i u m f a l c i p a r u m in fecte d m ice . I n : A n tim icrob ia l A g e n ts and C h em o therap y, p. 5 3 7 - 5 4 2 , 1 9 6 7 .
17. L ew is C . A n tip la sm o d ia l activ ity o f 7-h alogen ated lin com ycin s. T h e Journal o f P ara sito lo g y 5 4 : 1 6 9 - 1 7 0 , 1968.
18. M eira D A , Curi P R , B arraviera B . M ala ria in H u m aita coun ty, A m a z o n a s S tate, Brazil. X X I X - S om e c o m parative ep id em io lo g ic asp ects in 1 9 7 6 ,1 9 7 9 and 1 9 8 3 . In: P ro c ee d in g s o f IV Japan -B ra zil S y m p o siu m on S c ien ce and T e c h n o lo g y S ã o P a u lo 2: 1 3 6 - 1 4 3 , 1 9 8 4 . 19. M eira D A , Cu ri P R , M a rco n d es J , M atsu ok a E S , F avrin M A , E l - K h ou ry A B , M o tta N G S . M ala ria at H um aita C ou n ty, A m a z o n a s S tate, B razil. X V I I -Im m une resp on se in patients w ith P l a s m o d i u m f a l c i p a r u m ac cording to g a m eto cy tes. R e v ista d o In stituto de M ed ic in a T rop ical d e S ã o P a u lo 2 7 : 2 2 9 - 2 3 7 ,1 9 8 5 .
2 0 . M eira D A , M a rco n d es J , B arraviera B , P ereira P C M , R u i P , C u ry P R . M a la ria a t H u m a ita C ou n ty, A m a z on as S tate, B razil. X V I - G a m e to c y te s an d lym p h o c y te s stu died in p atien ts w ith P l a s m o d i u m f a l c i p a r u m . R e vista d o In stitu to d e M ed ic in a T rop ical d e S ã o P a u lo 2 4:(S u p l. 6): 3 2 - 3 9 , 1 9 8 2 .
2 1 . M eira D A , P elleg rin o Jún ior J, M a rco n d es M a ch a d o J, Tsuji K , M atsu o k a E S , H a id a E , E l K h ou ry A B .
F re q u en cy o f hu m an leu k o cy te antigen (H L A ) in pa tients w ith m alaria an d in the general p op u lation o f H u m aita c ou n ty, A m a z o n a s S tate, B rasil, R ev ista da S o cied a d e B rasileira d e M ed ic in a T rop ical 20: 1 5 3 -1 5 8 , 1 9 8 7 .
2 2 . M iller L H , G le w R H , W y le r D J , H ow ard W A , C ollin s W E , C o n ta c o s P G , N e v a F A . E v a lu a tio n o f clin d a m y cin in com b in ation w ith quinine a g ain st m ulti drug-resistant strains o f P l a s m o d i u m f a l c i p a r u m . A m e rican Journal o f T ro p ica l M ed ic in e and H y g ie n e 23: 5 6 5 - 5 6 9 , 1 9 7 4 .
2 3 . O P A S - M a n u a l de D ia g n ó s tic o M ic ro scó p ic o d a M a laria. P u b lic a ç ã o C ie n tífic a nP 2 7 6 , p. 1 0 9 , 1 9 7 5 . 2 4 . P ereira P C M , M a rco n d es J , B arraviera B , M eira D A ,
M en d es R P , V ad ileti C , S og a y a r R , R u i P . M alá ria n o m u n icíp io d e H u m aitá, E s ta d o d o A m a z o n a s. X I I I -U s o da clin d a m icin a n o tratam ento de d o en tes c o m in fe cç ã o ca u sa d a p e lo P l a s m o d i u m f a l c i p a r u m . R e vista d o In stitu to d e M ed ic in a T rop ical d e S ã o P a u lo 24: (S u p l. 6): 1 6 -2 3 , 1 9 8 2 .
2 5 . P eters W . C h em oth erap y o f m alaria. In: Julius P . K reier, (e d ) M ala ria. V o l. 1, A c a d e m ic P re ss, p. 1 4 5 -2 8 3 , 1 9 8 0 .
2 6 . P o w ers K G , J a c o b R L . A c tiv ity o f tw o chlorinated lin co m y cin an alogu es again st ch loroq u in e resisten t fa l ciparum m alaria in o w l m on k eys. In: A n tim icrob ia l A g e n ts and C h em oth erap y 4 9 - 5 3 , 1 9 7 2 .
27 . R ieck m an n K H , P o w e ll R D , M cN a m a r a J V , W ille rso n Jr D , K a s s L , F risc h e r H , C a r so n P E . E ffe cts o f tetracyclin e again st ch loroq u in e-resistan t and ch loro quine se n sitiv e P l a s m o d i u m f a l c i p a r u m . A m erica n J o u m a l o f T rop ical M ed ic in e and H y g ie n e 2 0 : 8 1 1 - 8 1 5 , 19 7 1 .
2 8 . R iv era D G , Cabrera, B D , L ara N T . T rea tm en t o f falciparum m alaria w ith c lin d am ycin . R e v ista d o In sti tut» d e M ed ic in a T ro p ica l de S ã o P a u lo 2 4 (S u p l. 6): 7 0 -7 5 , 1 9 8 2 .
2 9 . S ch im id t L H , H arrison J , E llis o n R , W o rcester P . T h e activ ities o f ch lorin ated lin co m y c in d eriv atives again st in fection s with P l a s m o d i u m c y n o m o l g i in M a c a c a m u l l a t t a . A m e ric a n jo u rn a l o f T rop ical M ed ic in e and H y g ie n e 19: 1 -1 1 , 1 9 7 0 .
3 0 . Seaberg L S , P arq uette A R , G lu zm a n IY , Phillips-Jr. G W , B rod ask y T F , K rogstad D J . C lin d am ycin activ ity against ch loroq u in e resistan t P l a s m o d i u m f a l c i p a r u m . Journal o f In fectio n s D is e a s e s 150: 9 0 4 - 9 1 1 , 1 9 8 4 .