13
Case R eport
REVISTA PAULISTA DE MEDICIN ABilate ral carotid body
paraganglioma: case re port
University Hospital of Universidade de São Paulo, São Paulo, Brazil
a b s t r a c t
CO N TEX T: Surg ical treatment o f caro tid bo dy parag ang lio mas is a challeng e to the surg eo n because o f the larg e vasculariz atio n o f the tumo r, invo lvement o f the caro tid vessels and the clo se anato mical relatio nship with the cranial nerves.
CASE REPO RT: A 6 3 -year-o ld patient was submitted to resectio n o f two caro tid bo dy parag ang lio ma tumo rs fo und in the rig ht-side and left-side caro tid bo dies at the bifurcatio n o f the co mmo n caro tid ar-teries. Two surg eries were perfo rmed at different times and neither o f them presented any mo rbidity. Arterio g raphy was fundamental fo r diag no sis o f the small, asympto matic tumo r o n the rig ht side.
DESIGN : Case Repo rt
KEY W O RDS: Caro tid bo dy. Parag ang lio ma. Cranial nerves.
• Erasmo Simão da Silva • Fábio Lambertini To z z i • Flávia Helena Matta de Paiva • G raz iela de Almeida Sukys
INTRODUCTION
Surgical treatment o f caro tid bo dy paraganglio -mas is a challenge to the surgeo n because o f the large vascularizatio n o f the tumo r, invo lvement o f the ca-ro tid vessels and the clo se anato mical relatio nship with the cranial nerves.
With the advance o f diagno sis and the impro ve-ment in surgical techniques fo r vascular resto ratio n and embo lizatio n, as well as the understanding o f bio -lo gical b ehavio r o f tumo rs, surgical treatment has develo ped and beco me safer.
CASE REPORT
A 63-years-o ld white male patient, with a his-to ry o f a painless mass o n the left side o f the neck during the preceding six mo nths. He denied having dysphagia, ho arseness, buzzing, headache, arterial hy-pertensio n crises and tachycardia, o r having similar cases amo ng relatives.
On ce rvical e xam inatio n, a m o tile , pulsatile mass, with no fremitus o r murmur, was o bserved o n the left side, next to the angle o f the mandible.
Co mputer to mo graphy revealed a 5.5 x 3.8 x 3.2 cm mass o n the bifurcatio n o f the left co mmo n caro tid artery. Arterio graphy demo nstrated a hypervascularized mass o ccupying and defo rming the left-side caro tid bi-furcatio n (Figure 1), as well as a small fo rmatio n in the regio n o f the right-side caro tid bifurcatio n (Figure 2). The pro visio nal diagno sis was bilateral caro tid bo dy paraganglio ma.
Surgical treatment was preferred. On the left
14
side, an o blique incisio n was made, fo llo wing the an-terio r bo rder o f the sterno cleido masto id muscle, and extended pro ximally to ward the masto id pro cess. Fo r ad e q uate e xp o sure , the d igastric and stylo hyo id muscles were sectio ned, and cranial iso latio n o f the hypo glo ssal nerve was do ne. The vagus nerve with its pharyngeal and laryngeal rami was identified. The subadventitial dissectio n technique was emplo yed and the external caro tid artery was ligated, fo r better expo sure o f the tumo r. There was no evidence o f neuro -lo gical deficit after the surgery.
Fo ur mo nths later the small mass o n the right side was resected. Diagno sis was co nfirmed by the histo lo gical analysis o f fragments o f bo th masses.
DISCUSSION
Caro tid bo dies are ellipso id, red-bro wn fo rma-tio ns, 5 to 7 mm in height by 2.5 to 4 mm in width, lo cated in the po sterio r face o f the co mmo n caro tid arte ry b ifurcatio n1 (as de scrib e d b y Vo n Halle r in
1743).2 Reigner3 acco mplished the first excisio n o f a
tumo r at this lo catio n in 1880, but witho ut the patient’s survival. In 1886, Maydl4
was successful in the resec-tio n, but the patient became hemiplegic and aphasic. In 1889, Albert5 succeeded in remo ving the tumo r.
The caro tid trigo ne co mprises the co mmo n ca-ro tid artery and its rami, the internal jugular vein and the vagus nerve. Amo ng the structures that may be invo lved by these tumo rs and o ught to be preserved during the surgical pro cedure are the hypo glo ssal nerve, the pharyngeal and superio r laryngeal rami o f the vagus nerve, the accesso ry nerve, the glo sso pha-ryngeal nerve, the mandibular ramus o f the facial nerve and the cervical sympathetic chain.
Caro tid bo dy tumo rs are rare. Five hundred pa-tients had been repo rted in the medical literature by 1972,6 six hundred by 19867 and o ne tho usand by 19888
(a prevalence o f 0.012% in auto psies).9
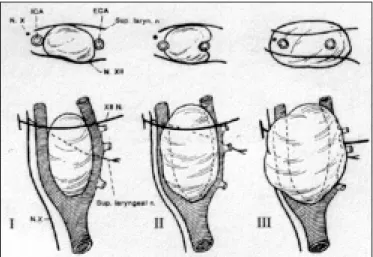
Shamblin et al10 classified these tumo rs acco
rd-ing to the degree o f invasiveness o f the arterial walls (Fig.3). Gro up I tumo rs are small and easily dissected in relatio n to the arterial wall; gro up II tumo rs are larger and adhered to the caro tid adventitia, thus present-ing difficulties in surgical resectio n; gro up III tumo rs are large and adhere intimately to the caro tid
adven-titia (the highest co mplicatio n rates are fo und within this gro up).11
There is no relatio nship between the histo lo gi-cal appearance o f the tumo r and its behavio r; that is, it is no t po ssible to make a histo lo gical differentia-tio n between slo w gro wing tumo rs and rapid, inva-sive o nes. The presence o f metastases in the lymph no des, o r in mo re distant o rgans12, 13 (1.7% to 50%)12,14,
demo nstrates the malignancy o f these tumo rs. Mo rbidity related to no n-resected tumo rs is sig-nificant and includes paralysis o f the cranial nerves, dysphagia, o bstructio n o f the airways and invasio n o f the base o f the skull.12
The spo radic fo rm is the mo st co mmo n o ne and abo ut 5% o f the cases are bilateral.9,15,16 The seco nd,
rarer o ne, is the familial fo rm, with a pattern o f auto -so mal, do minant inheritance, and abo ut 32% o f the
Table 1 - Pe riope rative complications of surgical re se ction for ce rvical paragangliomas
Authors Tim e periods N M orta lity (%) Cra nia l nerve dy sfunction (%) Periopera tive strok e (%)
Hallet Jr (Mayo Clinic) 1 4 1 9 3 5 to 1 9 6 5 7 0 6 4 6 2 3
1 9 6 6 to 1 9 7 5 4 6 2 3 0 9
1 9 7 6 to 1 9 8 7 3 7 0 4 0 2 .7
Leo netti (Illino is)1 9 1 9 8 8 to 1 9 9 5 1 6 0 5 0 0
Figure - Arteriogram of typical carotid body paraganglioma (left side).
15
cases are bilateral.6
Altho ugh asympto matic in the initial stages, 93% o f patients repo rt the presence o f a mass14 as the first
manifestatio n o f the disease. Other sympto ms, such as accelerated gro wth o f the mass (73%), headache o r neck pain (35%), buzzing, dizziness, ho arseness (8%), dysphagia (8%) and synco pe, o ccur in 75% o f the pa-tients. There is invo lvement o f the cranial nerves,
es-Figure 2 - Arteriogram of the little carotid body paraganglioma (right side).
Figure 3 - The classification of Shambin et al.10 of the difficulty of
surgical resection.
pecially the vagus and the hypo glo ssal,17 in 10% o f the
cases. Likewise, the cervical sympathetic chain and the glo sso pharyngeal nerve may also be attacked.14
Differential diagno sis includes branchial cysts, caro tid aneurysms, metastatic carcino mas, intravagal tumo rs, lympho mas and ecto pic thyro id.12 On clinical
examinatio n these tumo rs are lo cated belo w the angle o f the mandible and po sterio r to the anterio r bo rder o f the sterno cleido masto id muscle. They are mo tile in the lateral directio ns, but their relatio nship o f pro x-imity to the mandible limits their mo vements in the inferio r-superio r directio n. The presence o f fremitus and murmur in the regio n o f the caro tid bifurcatio n is no t co mmo n. A mass in the pharyngeal regio n may be the mo st frequent indicatio n (38%).18
Ultraso no graphy (co lo r-Do ppler) may co nfirm diagno stic suspicio ns o f tumo r presence. Co mputer to mo graphy sho ws a mass at the caro tid bifurcatio n and helps the analysis and detectio n o f invo lvement o f the cranial base, pharynx and jugular vein. Nuclear magnetic reso nance supplies even greater details o f in fo rm atio n o b tain e d fro m to m o g rap h y an d angio reso nance pro vides evidence o f tumo r irrigatio n and athero ma plaque at the caro tid bifurcatio n19
. Besides co nfirming the diagno sis (widening o f the caro tid bifurcatio n and hypervascularized mass; see Fig.1), arterio graphy detects the presence o f o c-clusive caro tid disease, the status o f intracereb ral blo o d circulatio n, tumo r irrigatio n and the presence o f small asympto matic co ntralateral tumo rs, as well as allo wing preo perative embo lizatio n.10 In this case
repo rted here, it was fundamental in the diagno sis o f the tumo r o n the right side.
Surgical treatment sho uld be perfo rmed o n the majo rity o f patients. Ho wever, the slo w gro wth o f these tumo rs and po o r surgical results in initial cases10,20 in
relatio n to mo rbidity and mo rtality led many surgeo ns to believe that surgical treatment carried to o many risks.
A significant decrease in death rates and vascu-lar accidents14 can be attributed to the impro vement
in vascular resto ratio n techniques, to subadventitial dissectio n o f the tumo r in relatio n to the arterial wall, bro ader incisio n fo r distal expo sure o f the internal caro tid, o ptical magnificatio n o f the o perative field, b ipo lar e le ctro caute rizatio n, m ultidisciplinary ap-pro aches, mo nito ring using electro encephalo graphy during the o peratio n, impro vement in anesthetic pro -cedures, intro ductio n o f heparin, early diagno sis and preo perative embo lizatio n.
Surgical results have impro ved in relatio n to the incidence o f cerebro vascular accidents and mo rtality.
16
Nevertheless, the high rate o f cranial nerve dysfunc-tio n causes co ncern, having reached 50% in so me cases19 (Table 1). The best results are repo rted fro m
tho se cases where a multidisciplinary appro ach was used,17 with a vascular surgeo n, head and neck
sur-geo n, and preo perative embo lizatio n.21
Restrictio ns o n embo lizatio n include situatio ns when there are tumo rs smaller than 3.0 cm o r very small nutrient arteries, the duratio n o f the examinatio n (fro m fo ur to six ho urs) and the likeliho o d o f cerebral embo li.
The majo rity o f autho rs have no t managed to find co nfirmatio n o f any benefits fro m radio therapy fo r surgically untreatable patients.10,12,15,18
Me tic ulo us surgic al te c hniq ue s, as we ll as kno wledge o f the anato my o f the regio n, are impo rtant issues fo r the decrease o f the incidence o f neuro -lo gical lesio ns during caro tid b o dy tumo r remo val surgery. Arterio graphy may detect small masses, thus co ntributing to early diagno sis o f these tumo rs.
1. Williams PL, Warwick R, Dyso n M, Bannister LH, edito rs. Gray’s An ato m y 35th e d . Lo n g m an , Lo n d o n : Ch u rc h ill Livin g s to n e ; 1989;8:1302-03.
2. Van Haller (1793). Cited in: Ko hn A. Die Paranganglien. Arch Mikr Anat 1903;62:263-8.
3. Riegner (1880). Cited in: Lahey FH, Warren KW. A lo ng-term appraisal o f caro tid bo dy tumo rs with remarks o n their remo val. Surg Gynec Obstet 1951;92:481.
4. Maydl (1886). Cited in: Byrne JJ. Caro tid bo dy and allied tumo rs. Am J Surg 1958;95:371.
5. Albert (1889). Cited in: Staats EF, Bro wn RL, Smith RR. Laryngo sco pe 1966;76:907.
6. Smith LL, Field FI. Management o f unco mmo n lesio ns affecting the extracranial vessels. In: Rutherfo rd RB, edito rs. Vascular Surgery 3rd ed. WB Saunders Co : Philadelphia; 1989:1441-50.
7. DuBo is J, Kelly W, McMenamin P, Macbeth A. Bilateral caro tid bo dy tumo rs managed with preo perative embo lizatio n: a case repo rt and review. J Vasc Surg 1997;5:648-50.
8. Liapis C, Go ugo lakis A, Karydakis V, Ve riko ko s C, Do ssaio to u B, Skandalakis P, Go gas J, Sechas M. Changing trends in management o f caro tid bo dy tumo rs. Am Surg 1995;61:989-93.
9. Rush Jr BF. Current co ncepts in the treatment o f caro tid bo dy tumo rs. Surgery 1962;52:679-81.
10. Shamblin WR, Remine WH, Sheps SG, Harriso n Jr EG. Caro tid bo dy tumo r: chemo decto ma. Am J Surg 1971;122:732-43.
11. Burihan MC, Albuquerque RGB, Nascimento JFB, Nasser F, Ingrud JC. Tumo r
REFERENCES
de co rpo caro tídeo : relato de do is caso s. Cir Vasc Ang 1997;13:13-18.
12. Meyer FB, Sundt Jr TM, Pearso n BW. Caro tid bo dy tumo rs: a subject review and suggested surgical appro ach. J Neuro surg 1986;64:377-85.
13. LaMuraglia GM, Fabian RL, Brewster DC, Spellman JP, Darling RC, Cambria RP, Abbo tt WM. The current surgical management o f caro tid bo dy paraganglio mas. J Vasc Surg 1992;15:1038-45.
14. Hallet Jr JW, No ra JD, Ho llier LH, J. Cherry Jr KJ, Pairo lero PC. Trends in neuro vascular co mplicatio ns o f surgical management fo r caro tid bo dy and cervical paraganglio mas: a fifty-year experience with 153 tumo rs. Surgery 1988;7:284-91.
15. De nt TL, Tho m p so n NW, Fry WJ. Caro tid b o d y tum o rs. Surge ry 1976;80:365-72.
16. Lees CD, Levine HL, Beven EG, Tucker HM. Tumo rs o f the caro tid bo dy: experience with 41 o perative cases. Am J Surg 1981;142:362-5.
17. Glenner GG, Grimley PM. Tumo rs o f the extra-adrenal paraganglio n system. In: Atlas o f Tumo r Patho lo gy, seco nd series, fasc 9. Washingto n, Armed Fo rces Institute o f Patho lo gy;1974.
18. Westbro o k KC, Guillamo ndegui OM, Medellin H, Jesse RH. Chemo decto ma o f the neck: selective management. Am J Surg 1972;124:760-6.
19. Leo netti JP, Do nzelli JJ, Litto o y FN, Farrell BP. Oto laryngo l Head Neck Surg 1997;117:111-5.
20. Martin CE, Ro senfeld L, McShwin B. Caro tid bo dy tumo rs: a 16-year fo llo w-up o f seven malignant cases. So uth Med J 1973;66:1236-43.
21. Ro binso n JG, Shagets FW, Beckett WC, Spies JB. A multidisciplinary appro ach to reducing mo rb idity and o perative b lo o d lo ss during resectio n o f caro tid bo dy tumo r. Surg Gyneco l Obst 1989;168:166-70.
r e s u m o
CO N TEX TO : O tratamento cirúrg ico do s parag ang lio mas de co rpo c a ro tíd e o é um d e sa fio p a ra o c irurg iã o d e vid o à a mp la vasculariz ação do tumo r, o envo lvimento co m o s vaso s caro tídeo s e a íntima relação anatô mica co m o s nervo s craniano s.
RELATO DE CASO : Um pa c iente de 6 3 a no s fo i sub metido à re sse c ç ã o d e d o is p a ra g a ng lio ma s, lo c a liz a d o s no s c o rp o s caro tídeo s do lado direito e esquerdo , junto às bifurcaçõ es das artérias caró tidas co muns. As cirurg ias fo ram em tempo s diferentes e ambas sem mo rbidade. Para o diag nó stico do tumo r pequeno do la d o d ire ito (a ssinto má tic o ) fo i fund a me nta l a a rte rio g ra fia diag nó stica.
PALAV RAS-CHAV E: Co rpo Ca ro tídeo . Pa ra g a ng lio ma . N ervo s craniano s.
Erasmo Simão da Silva. Assistant Pro fesso r in Human Structural To po graphy,
Department o f Surgery, Faculty o f Medicine o f Universidade de São Paulo , assistant do cto r at the University Ho spital o f Universidade de São Paulo . São Paulo , Brazil.
Fábio Lambe rtini Tozzi. Assistant do cto r at the University Ho spital o f Universidade de São Paulo . São Paulo , Brazil.
Flávia He le na Matta de Paiva. Under-graduate at the Faculty o f Medicine o f Universidade de São Paulo . São Paulo , Brazil.
Grazie la de Alme ida Sukys. Under-graduate student at the Faculty o f
Medicine o f Universidade de São Paulo . São Paulo , Brazil.
Source s of funding: No t declared
Conflict of inte re st: No t declared Last re ce ive d: 14 January 1999 Acce pte d: 3 February 1999
Addre ss for corre sponde nce : Erasmo Simão da Silva Rua Martins 96, Butantã
São Paulo /SP – Brasil – CEP 05511-000 E-mail: ersimao @ usp.br
p u b lis hin g in fo r m a t io n