w w w . r b o . o r g . b r
Original
Article
Study
on
the
relationship
between
the
thickness
of
the
anterior
cruciate
ligament,
anthropometric
data
and
anatomical
measurements
on
the
knee
夽
Victor
Marques
de
Oliveira,
Gabriel
Carmona
Latorre,
Alfredo
dos
Santos
Netto,
Rafael
Baches
Jorge,
Guinel
Hernandez
Filho,
Ricardo
de
Paula
Leite
Cury
∗FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15May2015 Accepted1June2015
Availableonline6February2016
Keywords:
Knee
Anteriorcruciateligament Anatomy
Magneticresonanceimaging
a
b
s
t
r
a
c
t
Objectives:Toascertainthicknessmeasurementsontheanteriorcruciateligament(ACL)in itsmiddlethirdonmagneticresonanceimaging(MRI)scansandtoassesswhetherthereis anyassociationbetweenvariationsinligamentthicknessandpatients’heightsandages, alongwithvariationsintheanatomicalmeasurementsontheknee.
Methods:MRIscanson48kneeswereevaluated.Theanteroposteriorsizeofthefemoral condyles,interepicondylardistance,intercondylardistanceandanteroposteriorand medio-lateralthicknessesofthe ACLweremeasured.Itwasassessedwhether therewasany statisticalrelationshipbetweenACLthicknessandthepatients’age,heightorother mea-surementsevaluated.
Results:ThemeanthicknessofthemiddlethirdoftheACLwas4.5mminthesagittalplane and4.3mminthefrontalplane.TheanteroposteriorthicknessoftheACLinitsmiddlethird hadapositiverelationshipwiththesizeofthelateralcondyle.Themediolateralthickness oftheACLinitsmiddlethirdhadapositiverelationshipwiththesizeofthelateralcondyle andwiththeintercondylardistanceintheaxialplane.Therewasnorelationshipbetween thethicknessoftheACLandthepatients’ageorheight.
Conclusion:ThethicknessoftheACLpresentedpositiveassociationswiththesizeofthe lateralfemoralcondyleandtheintercondylardistance.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedintheDepartmentofOrthopedicsandTraumatology,IrmandadedaSantaCasadeMisericórdiadeSãoPaulo,São Paulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.dePaulaLeiteCury).
http://dx.doi.org/10.1016/j.rboe.2016.01.013
Estudo
da
relac¸ão
entre
a
espessura
do
ligamento
cruzado
anterior,
os
dados
antropométricos
e
as
medidas
anatômicas
do
joelho
Palavras-chave:
Joelho
Ligamentocruzadoanterior Anatomia
Imagemporressonância magnética
r
e
s
u
m
o
Objetivo: Obterasmedidasdaespessuradoligamentocruzadoanterior(LCA)emseuterc¸o médioemexamesderessonânciamagnéticaeavaliarseexisteassociac¸ãoentreavariac¸ão daespessuradoligamentocomaalturaeaidadedospacientes,bemcomocomasvariac¸ões dasmedidasanatômicasdojoelho.
Métodos: Foramavaliadososexamesderessonânciamagnéticade48joelhos,aferidasas medidasdotamanhoanteroposteriordoscôndilosfemorais,distânciainterepicondilar, dis-tânciaintercondilareasespessurasanteroposterioremediolateraldoLCAeavaliamosse existerelac¸ãoestatísticaentreaespessuradoLCAeaidadeouaalturadospacienteseas demaismedidasavaliadas.
Resultados: Amédiadaespessuranoterc¸omédiodoLCAfoide4,5mmnoplanosagital e4,3mmnoplanofrontal.AespessuraanteroposteriordoLCAnoseuterc¸omédiotem relac¸ãopositivacomotamanhodocôndilolateral.AespessuramediolateraldoLCAno seuterc¸omédiotemrelac¸ãopositivacomotamanhodocôndilolateralecomadistância intercondilarnoplanoaxial.Nãoencontramosrelac¸ãoentreaespessuradoLCAeaidade ouaalturadospacientes.
Conclusão:AespessuradoLCAapresentaumaassociac¸ãopositivacomotamanhodocôndilo femorallateraleadistânciaintercondilar.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Reconstructionoftheanteriorcruciateligament(ACL)isone ofthesurgicalproceduresmostfrequentlyperformedwithin orthopedists’clinicalpracticeanditsresultsarewell estab-lishedintheliterature.1–6 Lackofsuccessinreconstructing the ligament is relatedto poor positioning ofthe tunnels, non-treatmentofassociatelesionsandproblemsrelatingto fixationandincorporationofthegraft,alongwith inappropri-aterehabilitationprotocols.7
Recently,Magnussenetal.8correlatedthediameterofthe graft usedwithfailure ofACLreconstruction. According to theseauthors, grafts with diameters less than or equal to 8mm had ahigherrepeated tear ratethan did grafts with diametersgreater than 8mm. Thus,the authors suggested thatreconstructionsshouldbeperformedwithgraftsof min-imumthickness9mm.
Despitetheadvantagerelatingtousinggraftsthatareas thickaspossible,complicationsinstandardizingthis charac-teristicmayleadtoadisproportionate increaseintheratio betweencontentandcontainmentstructureintheknee.This may generate pain, limitation ofthe range ofmotion and increasedriskoffailureofthereconstruction.7,9
Investigationofparametersthatenableindividualized sur-gical planning may improve the efficacy of treatment and diminishtheriskofintercurrencesduringtheintraoperative period.Factors predicting the graft that should beused in reconstructingtheligamentareamongtheseparameters Eval-uationofthemorphologyoftheACLanditsrelationshipwith theanthropometricdataandwiththeotherstructuresofthe kneemayprovideguidanceofgreaterprecisionandlowerrisk
inchoosingthethicknessofthegrafttobeusedinligament reconstructionsurgery.10
The aims of this study were to obtain thickness mea-surementsfromthemiddlethirdoftheACL,usingmagnetic resonanceimaging(MRI)examinations,andtoassesswhether therewasanyassociationbetweenthevariationinligament measurementsandpatients’heightandage,andalsoin rela-tiontovariationsinanatomicalmeasurementsontheknee.
Methods
Thiswasaretrospectivestudythathadbeenapprovedbythe ResearchEthicsCommitteeofSantaCasadeSãoPaulo. Forty-eightMRIexaminationsonthekneesofpatientswhowere beingfollowedupattheKneeGroupoutpatientclinicofSanta CasadeSãoPaulowereevaluated.Therewere25examinations onwomenand23onmen,andtheywereperformedbetween JanuaryandDecember2013.
The ages and heights of the patients examined were recorded.For the heightmeasurements, thepatients stood againstastadiometerinanerectmanner,witharmsextended alongthesidesofthebodyandheadraised,withoutwearing shoes.Thepatients’meanagewas44.3yearsandtheirmean heightwas1.70m.
Patients with skeletal immaturity, previous surgery or degenerativealterationsinthekneeswereexcluded.
Fig.1–Anteroposteriorsizeofthefemoralcondyles.
saturation, using the following parameter: TE 1642, TE 30; matrix 512×256; FOV 16×16; slice thickness 3.5mm; and sliceinterval0.3mm.Theimageanalysisandmeasurements onall the parameters needed, andtheir correlations, were performedonworkstationsusingtheAgfaPACS/RISsystem. Thiswas done bytworadiologists who were specialists in radiologyofthemusculoskeletalsystem,whoanalyzedthe imagestogether,simultaneously.
ThefollowingmeasurementswereobtainedfromtheMRI:
- Anteroposterior size of the medial and lateral femoral condyles,obtainedfromthePD-weightedsequenceinthe sagittalplane(Fig.1).
- Interepicondylar distanceobtainedfromthe PD-weighted sequenceintheaxialplane(Fig.2).
Fig.2–Interepicondylardistanceintheaxialplane.
Fig.3–Intercondylardistanceintheaxialplane.
- Intercondylar distance obtained from the PD-weighted sequenceintheaxialplane(Fig.3).
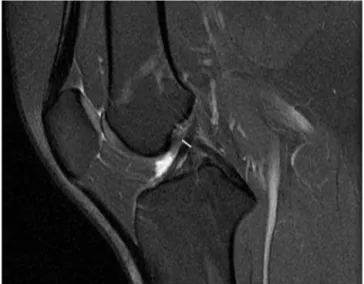
- AnteroposteriorthicknessoftheACLobtainedfromthe PD-weightedsequenceinthesagittalplane,bymeansoflinear measurementinitsmiddlethird,perpendiculartothelong axisoftheligamentfibers(Fig.4).
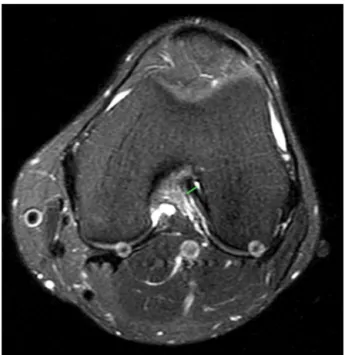
- Mediolateral (transverse) thickness of the ACL obtained fromthePD-weightedsequenceintheaxialplane,bymeans oftransverselinearmeasurementsinitsmiddlethird, tak-ingthegreatestdiameteroftheligamentfibers(Fig.5).
Theresultswereorganizedbymeansoftablesandgraphs, and were thensubjected tostatistical teststoanalyze and validatetheresultsfromthisstudy.
Fig.5–MediolateralthicknessoftheACLintheaxialplane.
To perform the general descriptive analysis, the mean, standarddeviation,minimumvalue,medianandmaximum valueofeachofthemeasurementswerecalculated.
Tocomparethethicknessmeasurementsfromthemiddle thirdoftheACLwiththeothermeasurementsofthisstudy, Pearson’scorrelationcoefficient wasused. Thesignificance levelusedwas5%(p-value≤0.05).
The SPSS® software (Statistical Package for the Social Sciences,version13.0;Chicago,IL,USA)wasusedforthe sta-tisticalanalysis.
Results
ThemeanthicknessinthemiddlethirdoftheACLwas4.5mm inthesagittalplane(range: 3.1–7.2mm)and4.3mminthe frontalplane(range:2.9–6.2mm).
The mean size of the lateral femoral condyle was 62.2mm (range:48.1–74.7mm),while themean sizeofthe medialfemoralcondylewas55.7mm(range:43.2–67.4mm). The mean interepicondylar distance was 77.8mm (range: 61.8–91.7mm).Themeanintercondylardistancewas21.7mm, rangingfrom15.8to30mm(Table1).
ItwasseenthattheanteroposteriorthicknessoftheACL initsmiddlethirdhadapositiverelationshipwiththesize ofthelateralcondyle.Wedidnotfindanyotherstatistically significantassociationinvolvingtheanteroposteriorthickness
oftheACL(Table2).
ItwasobservedthatthemediolateralthicknessoftheACL initsmiddlethirdhadapositiverelationshipwiththesizeof thelateralcondyleandwiththeintercondylardistanceinthe axialplane.Wedidnotfindanyotherstatisticallysignificant associationinvolving themediolateralthicknessofthe ACL
(Table3).
Wedidnot findany relationshipbetweenthe thickness ofthe ACL and the patients’ ages orheights. However,we observedatendencytowardapositiverelationshipbetween theanteroposteriorthicknessoftheACLandheight(p=0.054), butwithoutstatisticalsignificance.
Discussion
Overrecentdecades,inattemptstodiminishthefailurerates from ligamentreconstruction, differentstudies have evalu-atedaspectsoftheanatomyoftheACL5,11 andthe various surgicaltechniquesusedforligamentreconstruction.2–7
Magnussen et al.8 demonstrated that there was an inverselyproportionalrelationshipbetweenthethicknessof the graft used in ligament reconstruction and the risk of repeatedtearing.Inthislight,westudiedthethicknessofthe ACLinitsmiddlethird,bymeansofMRIexaminations,andwe evaluatedtheexistenceofrelationshipsbetweenthese mea-surementsandthevaluesforkneestructuresandthepatients’ agesandheights.
In our study,we found that the mean thickness of the middlethirdoftheACLwas4.3mminthefrontalplaneand 4.5mminthesagittalplane,usingMRI.Intheliterature,we foundconflictingresultsrelatingtothethicknessofthe mid-dlethirdoftheACL.Kupcziketal.12foundameanthicknessof 4.8mmusingMRIexaminations,whileAndersonetal.13found ameanfrontalthicknessof4.75mminwomenand5.6mmin men,andameansagittalthicknessof7.6mminwomenand 8.7mminmen.Thisdifferenceshowsthedifficultyin obtain-ing ACLmeasurementsfrom MRIexaminations,duetothe complexmorphologyoftheligamentandtheinfluenceofthe leveloftheslicestudiedonthemeasurementobtained.
Rezendeetal.9demonstratedthatanarrowintercondylar distancewasapredisposingfactorforACLinjury.Wefound apositiverelationshipbetweenthemediolateralthicknessof
Table1–Generaldescriptiveanalysisforthenumericalvariables.
Variable Mean Median Deviation Minimum Maximum
Age(years) 44.3 45.5 16.8 16.0 78.0
Height(meters) 1.7 1.7 0.1 1.5 1.9
Anteroposteriorsizeoflateralcondyle(mm) 62.2 61.2 5.4 48.1 74.7 Anteroposteriorsizeofmedialcondyle(mm) 55.7 55.4 5.2 43.2 67.4
Axialinterepicondylardistance(mm) 77.8 78.3 6.6 61.8 91.7
Axialintercondylardistance(mm) 21.7 21.7 3.0 15.8 30.0
MediolateralACLthickness(axial)(mm) 4.3 4.3 0.8 2.9 6.2
Table2–RelationshipbetweenanteroposteriorACLthickness(sagittal)andeachofthevariables.
Comparisons Coefficientofcomparison p-Value
AnteroposteriorACLthickness(sagittal)versusheight 0.280 0.054
AnteroposteriorACLthickness(sagittal)versusage 0.60 0.683
AnteroposteriorACLthickness(sagittal)versusanteroposteriorsizeofmedialcondyle 0.147 0.320 AnteroposteriorACLthickness(sagittal)versusanteroposteriorsizeoflateralcondyle 0.398 0.005 AnteroposteriorACLthickness(sagittal)versusinterepicondylardistance(axial) 0.265 0.069 AnteroposteriorACLthickness(sagittal)versusintercondylardistance(axial) 0.036 0.809
Table3–RelationshipbetweenmediolateralACLthickness(axial)andeachofthevariables.
Comparisons Coefficientofcomparison p-Value
MediolateralACLthickness(axial)versusheight 0.113 0.444
MediolateralACLthickness(axial)versusage 0.085 0.565
MediolateralACLthickness(axial)versusanteroposteriorsizeofmedialcondyle 0.040 0.786 MediolateralACLthickness(axial)versusanteroposteriorsizeoflateralcondyle 0.346 0.017 MediolateralACLthickness(axial)versusinterepicondylardistance(axial) 0.265 0.069 MediolateralACLthickness(axial)versusintercondylardistance(axial) 0.299 0.039
theACLinitsmiddlethirdandtheintercondylardistancein theaxialplane.Therearedivergencesintheliterature
regard-ingdepictionsoftherelationshipbetweenACLmorphology
and the morphology of the intercondylar region. Muneta
etal.14studied16kneesfromcadaversanddidnotfindany relationshipbetweenthewidthoftheintercondylarfossaand themorphologyoftheACL.Charltonetal.15andDienstetal.16 observedapositiverelationshipbetweenthevolumeofthe intercondylarfossaandtheapproximatevolumeoftheACL withintheintercondylarfossa,throughusingMRI examina-tionsonhealthyknees.Andersonetal.13reportedthatthesize oftheACLdidnotpresentadirectrelationshipwiththesize oftheintercondylarfossa,whileStijaketal.,17inastudyon cadavers,observedthatthethicknessoftheACLhadapositive correlationwiththeintercondylardistanceonlyamongmales. Apositiveassociation wasfoundbetweenthethickness oftheACLinitsmiddlethird,bothinthefrontalandinthe sagittalplane,andthesizeofthelateralfemoralcondyle.We didnotfindanystudiesintheliteratureevaluatingthese rela-tionships,butitisplausibletoexpectthatknees ofgreater diameterwillhavegreaterdimensionsforalloftheir anatom-icalstructures,andnotjusttheACL.
Nostatisticallysignificantrelationshipwasfoundbetween thethicknessoftheACL andage.Wealsodidnotfindany statistically significant relationship between the thickness ofthe ACLand thepatients’ heights,althoughtherewas a tendencytowardapositiverelationshipbetweenthe antero-posteriorthicknessoftheACLandheight,butwithp=0.054. Brownetal.18 studied414kneesbymeansofMRI examina-tionsandfoundapositivecorrelationbetweenthelengthof theACLandthepatients’heights.Thisassociationis espe-ciallyimportantwhentheACLreconstructionisdoneusinga graftfromthepatellartendon.Thoseauthorsdidnot evalu-ateanyassociationsinvolvingthethicknessoftheACL.Chan etal.19evaluatedthethicknessoftheflexortendons (semi-tendinosusandgracilis)usingMRIandthroughobservation during the operation, with regard to whether there might be any association between these measurements and the patients’heights.Theyfoundapositiveassociationbetween
the patients’ heights and the thickness of the flexor ten-donsonlythroughtheintraoperativedata.Noassociationwas foundbetweenheightandtendonthicknessthroughMRI.This findingraisesthequestionofwhetherthepatients’heights have apositiverelationshipwith thethickness ofthe liga-mentperse.Inourinvestigationoftheliterature,wedidnot findanystudiesthathadevaluatedthisassociation.Although our study didnotfind any association betweenACL thick-nessandheight,wefoundapositivetendency.Astudywith alargersamplewouldpossibleprovetheexistenceofsuchan association.
Thelimitationofthepresentstudywasthatthe measure-mentofmorphologicalstructuresbymeansofMRIpresented adiscrepancyinrelationtomeasurementsmadeon cadav-ers.However,itisshownintheliteraturethatthisdifference inmeasurementsdoesnotinterferewiththeanalysisandthe conclusionsreachedfromthesedata.20Anotherpointwasthe difficultyinestablishingarelationshipbetweenthefindings ofthestudyandtheproblemswithinclinicalpractice,such aswhattherelationshipisbetweenmeasurementsobtained fromthemiddlethirdoftheACLandthesizeofthegraftused inreconstructingtheACL.Thisoccurredbecausethe measure-mentsweremadeintwoplanes(axialandsagittal)but the ACLisathree-dimensionalhelicoidstructure,whichmakesit difficulttoestablishanexactgeometricrelationshipbetween theseparameters.
Conclusion
ThemeanthicknessoftheACLinitsmiddlethirdwas4.5mm intheanteroposteriorplaneand4.3mminthemediolateral plane.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. NoyesFR,MatthewsDS,MooarPA,GroodES.The
symptomaticanteriorcruciate-deficientknee.PartII:the
resultsofrehabilitation,activitymodification,andcounseling
onfunctionaldisability.JBoneJointSurgAm.
1983;65(2):163–74.
2. AlmA,GillquistJ.Reconstructionoftheanteriorcruciate
ligamentbyusingthemedialthirdofthepatellarligament.
Treatmentandresults.ActaChirScand.1974;140(4):289–96.
3. SeverinoNR,CamargoOPA,AiharaT,CuryRPL,OliveiraVM,
NishiharaC.Utilizac¸ãodoparafusoBoneMulchna
reconstruc¸ãodoligamentocruzadoanteriorcomtendõesdos
músculossemitendinosoegrácil.RevBrasOrtop.
2001;36(3):79–83.
4. CamanhoGL,ViegasAC.Avaliac¸ãodareconstruc¸ãodo
ligamentocruzadoanteriorempacientescomidadeacimade
45anos.RevBrasOrtop.2001;36(1/2):37–40.
5. HwangMD,PieferJW,LubowitzJH.Anteriorcruciateligament
tibialfootprintanatomy:systematicreviewofthe21st
centuryliterature.Arthroscopy.2012;28(5):728–34.
6. CamanhoGL,CamanhoLF,ViegasAC.Reconstruc¸ãodo
ligamentocruzadoanteriorcomtendõesdosmúsculos
flexoresdojoelhofixoscomEndobutton.RevBrasOrtop.
2003;38(6):329–36.
7. KamathGV,RedfernJC,GreisPE,BurksRT.Revisionanterior
cruciateligamentreconstruction.AmJSportsMed.
2011;39(1):199–217.
8. MagnussenRA,LawrenceJT,WestRL,TothAP,TaylorDC,
GarrettWE.Graftsizeandpatientagearepredictorsofearly
revisionafteranteriorcruciateligamentreconstructionwith
hamstringautograft.Arthroscopy.2012;28(4):526–31.
9. RezendeMU,CamanhoGL,SoltoAR,HernandezAJ.Estenose
dointercôndilocomofatorpredisponenteàlesäodo
ligamentocruzadoanterior.RevBrasOrtop.1994;29(5):276–80.
10.HofbauerM,MullerB,MurawskiCD,vanEckCF,FuFH.The
conceptofindividualizedanatomicanteriorcruciate
ligament(ACL)reconstruction.KneeSurgSportsTraumatol
Arthrosc.2014;22(5):979–86.
11.PieferJW,PflugnerTR,HwangMD,LubowitzJH.Anterior
cruciateligamentfemoralfootprintanatomy:systematic
reviewofthe21stcenturyliterature.Arthroscopy.
2012;28(6):872–81.
12.KupczikF,SchiavonMEG,SbrissiaB,FávaroRC,ValérioR.
Enxertoidealparaligamentocruzadoanterior:correlac¸ãoem
ressonânciamagnéticaentreLCA,isquiotibiais,tendão
patelaretendãoquadríceps.RevBrasOrtop.2013;48(5):
441–7.
13.AndersonAF,DomeDC,GautamS,AwhMH,RennirtGW.
Correlationofanthropometricmeasurements,strength,
anteriorcruciateligamentsize,andintercondylarnotch
characteristicstosexdifferencesinanteriorcruciate
ligamenttearrates.AmJSportsMed.2001;29(1):
58–66.
14.MunetaT,TakakudaK,YamamotoH.Intercondylarnotch
widthanditsrelationtotheconfigurationand
cross-sectionalareaoftheanteriorcruciateligament.A
cadaverickneestudy.AmJSportsMed.1997;25(1):69–72.
15.CharltonWP,StJohnTA,CiccottiMG,HarrisonN,Schweitzer
M.Differencesinfemoralnotchanatomybetweenmenand
women:amagneticresonanceimagingstudy.AmJSports
Med.2002;30(3):329–33.
16.DienstM,SchneiderG,AltmeyerK,VoelkeringK,GeorgT,
KramannB,etal.Correlationofintercondylarnotchcross
sectionstotheACLsize:ahighresolutionMRtomographic
invivoanalysis.ArchOrthopTraumaSurg.2007;127(4):
253–60.
17.StijakL,Radonji´cV,Nikoli´cV,Blagojevi´cZ,Aksi´cM,Filipovi´c
B.Correlationbetweenthemorphometricparametersofthe
anteriorcruciateligamentandtheintercondylarwidth:
genderandagedifferences.KneeSurgSportsTraumatol
Arthrosc.2009;17(7):812–7.
18.BrownJA,BrophyRH,FrancoJ,MarquandA,SolomonTC,
WatanabeD,etal.Avoidingallograftlengthmismatchduring
anteriorcruciateligamentreconstruction:patientheightas
anindicatorofappropriategraftlength.AmJSportsMed.
2007;35(6):986–9.
19.ChanKW,KaplanK,OngCC,WalshMG,SchweitzerME,
ShermanOH.Usingmagneticresonanceimagingto
determinepreoperativeautograftsizesinanteriorcruciate
ligamentreconstruction.BullNYUHospJtDis.
2012;70(4):241–5.
20.NgAW,LeeRK,HoEP,LawBK,GriffithJF.Anteriorcruciate
ligamentbundlemeasurementbyMRI.SkeletalRadiol.