w w w . r b o . o r g . b r
Original
Article
Body
mass
index
as
a
prognostic
factor
for
fracturing
of
the
proximal
extremity
of
the
femur:
a
case–control
study
夽
,
夽夽
Renato
Cavanus
Pagani
a,
Rodrigo
Ernesto
Kunz
b,∗,
Ricardo
Girardi
b,
Marcelo
Guerra
a,caUniversidadeLuteranadoBrasil(ULBRA),Canoas,RS,Brazil
bUniversityHospital,UniversidadeLuteranadoBrasil(ULBRA),Canoas,RS,Brazil cUniversidadeFederaldoRiodeJaneiro,RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19July2013 Accepted27August2013
Availableonline19September2014
Keywords:
Hipfracture Elderlyperson Bodymassindex
a
b
s
t
r
a
c
t
Objectives: Tocomparethebodymassindex(BMI)ofpatientswithfracturesintheproximal extremityofthefemurwiththeBMIofpatientswithoutanyprevioushistoryoffractures.
Methods:Weinvestigatedpatientsofbothsexes,aged65yearsorover,whowereadmitted toHospitalIndependência,HospitalBeneficênciaPortuguesaorULBRAUniversityHospital, betweenDecember2007andDecember2010,withhistoriesoflow-energytraumasuchas fallingfromastandingposition.Theseindividualswerecomparedwithpatientsofthesame agebutwithoutanyhistoryoffracturingoftheproximalextremityofthefemur(n=89),who wereattendedatthegeriatricsoutpatientclinicoftheSociedadePorto-AlegrensedeAuxílio aosNecessitados(SPAAN).
Results:Theagegroupofthepatientswithfracturesintheproximalextremityofthefemur rangedfrom65to96years(mean:77.58).Themaintypeoffracturewastrochanteric(47; 62.2%),followedbyfemoralneckfractures(27;36%).Amongthepatientswhopresentedon fracturingtheproximalextremityofthefemur,12%hadlowweight,62.7%normalweight, 24%overweight,and1.3%obesity.Amongthepatientswithoutanyhistoryoffractures, 5.6%presentedlowweight,43.8%normalweight,33.7%overweight,and9.8%obesity.Itwas observedthatthepatientswithfracturesintheproximalextremityofthefemur(n=75) presentedameanBMIof22.6,whilethepatientswithoutfracturespresentedameanBMI of25.5.
Conclusion: Thepatientsinthegroupwithfracturesweresignificantlytallerthanthosein thegroupwithoutfracturesandpresentedsignificantlylowerBMIthanthoseinthegroup withoutfractures.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:PaganiRC,KunzRE,GirardiR,GuerraM.Índicedemassacorporalcomofatorprognósticoparafraturada extremidadeproximaldofêmur:umestudodecaso-controle.RevBrasOrtop.2014;49(5):461–7.
夽夽
WorkdevelopedatHospitalIndependência,HospitalBeneficênciaPortuguesaandULBRAUniversityHospital,Canoas,RS,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](R.E.Kunz).
http://dx.doi.org/10.1016/j.rboe.2014.09.004
Índice
de
massa
corporal
como
fator
prognóstico
para
fratura
da
extremidade
proximal
do
fêmur:
um
estudo
de
caso-controle
Palavras-chave:
Fraturadequadril Idoso
Índicedemassacorporal
r
e
s
u
m
o
Objetivos: Compararoíndicedemassacorporal(IMC)depacientescomfraturada extrem-idadeproximaldofêmurcomoIMCdepacientessemhistóriapréviadefraturas.
Métodos: Investigamospacientesdeambosossexos,com65anosoumais,internadosno HospitalIndependência,noHospitalBeneficênciaPortuguesaenoHospitalUniversitário Ulbra,dedezembrode2007adezembrode2010,comhistóriadetraumadebaixaenergia, como,porexemplo,quedasdaprópriaaltura,emrelac¸ãoaospacientesdamesmaidade esemhistóriapréviadefraturasdaextremidadeproximaldofêmur(n=89)atendidosno servic¸oambulatorialdegeriatriadaSociedadePorto-AlegrensedeAuxílioaosNecessitados (Spaan).
Resultados: Afaixaetáriadospacientescomfraturadaextremidadeproximaldofêmur varioude65 a96anos(média:77,58).Oprincipal tipodefraturafoiatrocantérica(47; 62,2%),seguidadadocolodefêmur(27;36%).Entreospacientesqueapresentaramfraturada extremidadeproximaldofêmur,12%tinhambaixopeso,62,7%,pesonormal,24%,sobrepeso e1,3%,obesidade. Entreospacientessemhistória defratura,5,6%apresentarambaixo peso,43,8%,pesonormal,33,7%,sobrepesoe9,8%,obesidade.Verificou-sequeospacientes comfraturasdaextremidadeproximaldofêmur(n=75)apresentaramIMCmédiode22,6, enquantoospacientessemfraturasapresentaramIMCmédiode25,5.
Conclusão: Ospacientesdogrupocomfraturasãosignificativamentemaisaltosdoqueos dogruposemfraturaeapresentamIMCsignificativamenteinferioraodogruposemfratura. ©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Fracturesoftheproximalextremityofthefemurareamong thecommonesttraumaticinjuriestoday,notonlybecauseof theirhighincidenceintheelderlypopulationbutalsobecause oftheaccompanyingmorbidityandmortality.
Ithasbeenestimatedthattheincidenceofhipfractures willincreasedramaticallyoverthenext20years.Thisincrease willbemostevidentamongindividuals over the ageof85 years.1 Ithasalsobeenestimatedthatnine outofevery10 hipfracturesoccurinindividualsovertheageof65years.2 TheWorldHealthOrganization(WHO)haspredictedthatby theyear2050,theannualincidencewillbe6.26million.3
Fractures of the proximal extremity ofthe femur are a publichealthproblemworldwide.4,5 Inadditiontothehigh mortalityrate,thesepatientsrequireintensivemedicalcare andfunctionalrehabilitationoverlongperiods.6
They are associated with considerable functional inca-pacity, diminished independence and quality of life and, especially,decreasedlifeexpectancy.7,8
Fractures of the proximal extremity of the femur com-prise those of the head, neck, trochanteric region and subtrochantericregion.9
Itisobservedthatthesefracturesintheelderlypopulation are generallycaused bysmall and unintentionaltraumatic events,suchasfallingfromastandingposition,whichoccur through the debility resulting from senescence and also dependonextrinsicfactors.10Awell-documentedreporthas suggestedthatbodymassindex(BMI)isasignificant progno-sticfactorforhipfractures.
In thiscontext,fractures oftheproximal femurmaybe associated with lowBMI, which is considered to bea risk factor. Some authors have reported that the ideal BMI is 25–27.4kg/m2.Lowerindicesthan thisareconsidered tobe importantprognosticfactorsformortalityamongyoungand oldhospitalizedpatients.11
Itissuspectedthatobesityprovidesprotectionagainst frac-tures,butthemechanismsforsuchanassociationstillremain poorlyunderstood.12
Estrogenmayprotectagainsthipfracturesinvarious man-ners,byincreasingboneresistance,improvingneuromuscular function, modifying fat deposition and improving the vis-coelasticpropertiesofthesofttissues.13
Thepossiblehypothesesforthesituationofgreaterriskof hipfractureamongthinelderlypeopleinclude:theroleof adi-posetissueinproducingestrogen,whichreducestheriskof hipfractures;greaterweightincreasesthemechanicaltension on bonesandstimulates boneremodeling;and lowweight may beanindicatorordebilitatedhealth,whichinitselfis ariskfactorforfallsandfractures.
Materials
Thiswasacase–controlscientificstudyinwhich75patients whowerehospitalizedbetweenDecember2007andDecember 2010duetofracturingtheproximalextremityofthe femur wereassessed.
Thepatients were selected in accordance with the fol-lowing criteria: age greater than or equal to 65 years; diagnosis for hospitalization relating to fracturing of the proximal extremity of the femur; and presence of a his-toryoflow-energy trauma suchas fallingfrom a standing position.
The criteria for excluding patients were: the presence of pathological fractures, distal fractures and fractures of thefemoraldiaphysis;situationsofhigh-energytrauma;age under65years;presenceofspecificconditionsthat accentu-atebonemassloss;anduseofdrugsthatcausebonemass reduction.
Methods
Thepatientsstudiedwerecomparedwithagroupofpatients ofthesameagewhodidnothavefracturesoftheproximal femur(n=89)andwhowereattendedatthegeriatric outpa-tientserviceofSPAAN.
Datasuchasweightandheightwereascertainedfromthe medicalfilesorwere furnishedbythe patients,because of thedifficulty ofassessingtheseparameters among bedrid-den patients. Data such as age, sex, type of fracture (transtrochanteric,subtrochantericorfemoralneck)and frac-turemechanism(falling)wererecorded.
TheBMIwascalculated bydividingweight inkilograms byheightinmeters,squared.FourBMIcategorieswere cre-ated:lowweight(<18.5kg/m2);normalweight(18.5–25kg/m2); overweight(25–30kg/m2);andobese(>30kg/m2).
Thedata were analyzed bymeans of table,graphs and descriptivestatistics.Thefollowingstatisticaltestswere per-formed:
Chi-squaretestwasusedtoascertainwhethertherewas any significant association amongthe qualitative variables betweenthestudygroups(withandwithoutfractures),and,in relationtothegroupwithfracturesalone,toascertainwhether anyassociationexistedbetweenthetypeoffractureandthe othervariables;
Student’sttest wasusedtocompare mean age,height, weightandBMIbetweenthestudygroups(withandwithout fractures).
For allthe abovementioned tests, themaximum signifi-canceleveltakenwas5%(p≤ 0.05).Thesoftwareusedforthe statisticalanalysiswasSPSSversion10.0.
The data were stored in a specific database using the MicrosoftExcel2010forWindows®software.
Asearchforarticlesrelatingtothestudy topicwas con-ductedinelectronicfilingsystemssuchasPubmed,Lilacsand Scielo.
Properauthorization wasobtainedfrom theinstitutions fordatagatheringintheirfilingsystems,andtheprojectwas approvedbytheULBRAresearchethicscommitteeunder pro-tocolnumber2010-237H.
Results
Inthissection,theresultsrelatingtodatagatheredatthe insti-tutionsinvestigatedarepresentedanddiscussed(Table1).
Throughtheresultsfromthechi-squaretest,itwasfound thattherewerenosignificantassociationsinrelationtothe variablesofageandsexbetweenthegroups(withandwithout fractures).Inotherwords,therewasnorelationshipbetween occurrencesoffracturesandthesepatients’sexandage.This test aimsto ascertain whether any significant association existsbetweentwoqualitativevariables.Itissoughttofind outwhetheranypatientcharacteristicismorefrequentinone givengroupthaninanother.
Theagegroupofthepatientswithdiagnosesoffractures oftheproximalextremityofthefemurrangedfrom65to96 years,withameanof77.58.
Inrelationtosexamongthepatientswithfractures,itwas foundthat56(74.7%)werefemaleand19(25.3%)weremale (Fig.1andTable2).
ThroughtheresultsfromtheindependentStudent’sttest, it was found in comparison between the above variables thattheonespresentingasignificantdifferencebetweenthe groupswithandwithoutfractureswerethefollowing:
- Height:itwasobservedthatthepatientsinthegroupwith fracturesweresignificantlytallerthanthoseinthegroup withoutfractures;
- BMI:itwasobservedthatthepatientsinthegroupwith frac-turespresentedsignificantlylower BMIthan thoseinthe groupwithoutfractures(Table3).
TheStudent’sttestaimsatcomparingvaluescomingfrom twoindependentgroups.Itcomparesthevaluesineachgroup (inthiscase,withandwithoutfractures)withtheaimof ascer-tainingwhetherthereisanysignificant differencebetween thesevalues.
Throughtheresultsfromthechi-squaretest,itwasfound thattherewasasignificantassociationbetweenthevariable ofBMIclassificationandthegroup(withorwithoutfracture). Itwasobservedthatnormalweightwassignificantly associ-atedwiththegroupwithfractures,whilepatientswhowere overweightorobesewereassociatedwiththegroupwithout fractures.
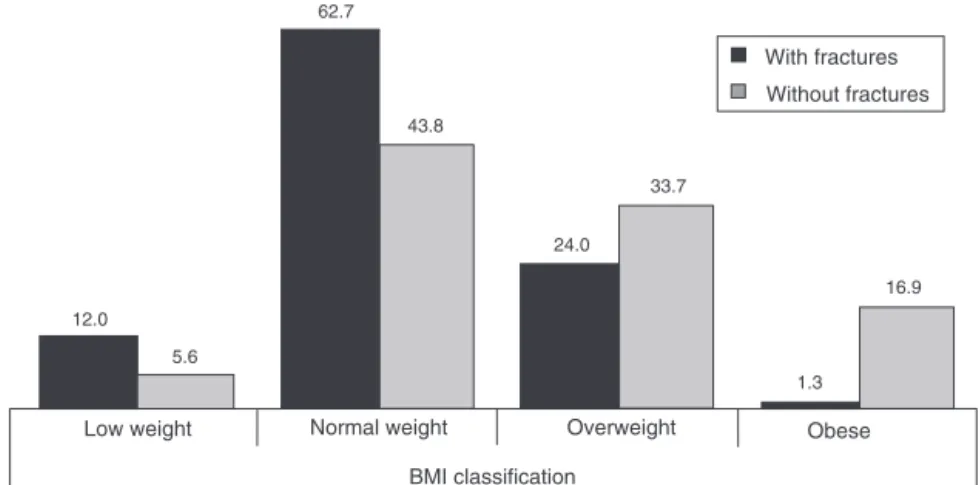
Amongthepatientswhopresentedfracturesofthe proxi-malextremityofthefemur,12%presentedlowweight,62.7% normal weight, 24% overweight, and 1.3% obesity. Among thepatientswithoutanyhistoryoffracturesoftheproximal extremityofthefemur,5.6%presentedlowweight,43.8% nor-malweight,33.7%overweight,and9.8%obesity.Itwasfound that the patients with fractures of the proximal extremity ofthefemur(n=75)presentedmeanBMIof22.6,whilethe patientswithoutfracturespresentedmeanBMIof25.5(Fig.2
andTable4).
Table1–Descriptionofthesampleinvestigatedaccordingtothevariablesofageandsexforthegroupswithfractures (n=75)andwithoutfractures(n=89).
Variable Category Group(%) Total pa
Withfractures Withoutfractures
Sex Female 74.7 62.9 68.3 0.107
Male 25.3 37.1 31.7
Age Upto70years 17.3 14.6 15.9 0.864
From71to80years 45.3 44.9 45.1
Over80years 37.3 40.4 39.0
Source:datagatheredin2011.
a pvalue(significancelevel).Forassociationstobeconsideredsignificant,thepvalueneededtobeamaximumof5%(p≤0.05).
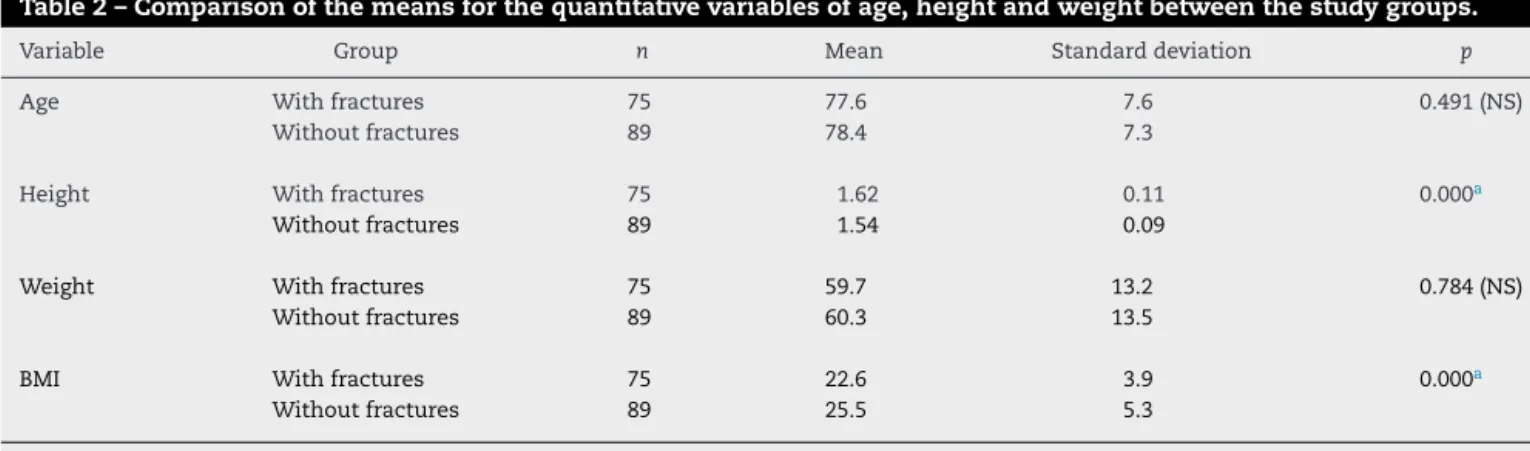
Table2–Comparisonofthemeansforthequantitativevariablesofage,heightandweightbetweenthestudygroups.
Variable Group n Mean Standarddeviation p
Age Withfractures 75 77.6 7.6 0.491(NS)
Withoutfractures 89 78.4 7.3
Height Withfractures 75 1.62 0.11 0.000a
Withoutfractures 89 1.54 0.09
Weight Withfractures 75 59.7 13.2 0.784(NS)
Withoutfractures 89 60.3 13.5
BMI Withfractures 75 22.6 3.9 0.000a
Withoutfractures 89 25.5 5.3
Source:datagatheredin2011.
NS,notsignificant.
a Significantatthesignificancelevelofp≤0.0001.
Themaintypesoffracturepresentedinthis studywere trochanteric(47cases;62.2%),femoralneck(27;36%)and sub-trochanteric(1;1.8%)(Fig.3).
Discussion
A total of 164 medical files were selected: 75 relating to patientsaged65yearsandoverwithadiagnosisoffracture
in the proximal extremity of the femur; and 89 relating to patients without a previous history of fractures of the proximalextremityofthefemur.
Theagesofthepatientswithadiagnosisoffractureinthe proximalextremityofthefemurrangedfrom65to96years, withameanof77.58.Thefracturecaseswerepredominantly intheagerangefrom71to80years(45.3%).VilasBôasJunior etal.14reportedthattheagerangefrom60to69yearswas theonemostaffected(36.64%).Rochaetal.15foundthatthe
62.9 74.7
Female
Sex
Male Up to 70 years From 71 to 80 years
Age
Over 80 years
25.3 37.1
17.3 14.6
45.3 44.9
37.3 40.4
With fractures
Without fractures
Fig.1–Descriptionofthesampleinvestigatedaccordingtothevariablesofageandsexforthegroupswithfractures(n=75 cases)andwithoutfractures(n=89cases).
Table3–DescriptionofthesampleinvestigatedaccordingtothevariableofBMIclassificationforthegroupswith fractures(n=75)andwithoutfractures(n=89).
BMIclassification Group(%) Total p
Withfractures Withoutfractures
Lowweight 12.0 5.6 8.5 0.003a
Normalweight 62.7 43.8 52.4
Overweight 24.0 33.7 29.3
Obese 1.3 16.9 9.8
Source:datagatheredin2011.
a Significantatthesignificancelevelofp≤0.01.ToperformthetestontheBMIvariable,thecategoriesofoverweightandobesityweregrouped.
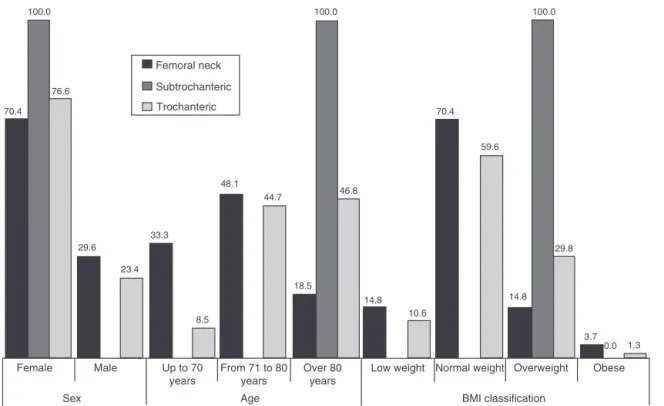
Table4–Comparisonofsex,BMIandageinrelationtothetypesoffracturethatoccurred,forthegroupwithfractures alone(n=75).
Variable Category Typeoffracture p
Femoralneck Subtrochanteric Trochanteric
Sex Female 70.4 100.0 76.6 0.693(NS)
Male 29.6 23.4
Age Upto70years 33.3 8.5 0.010a
From71to80years 48.1 44.7
Over80years 18.5 100.0 46.8
BMIclassificationb Lowweight 14.8 10.6 0.256(NS)
Normalweight 70.4 59.6
Overweight/obese 14.8 100.0 29.8
Source:datagatheredin2011.
NS,notsignificant.
a Significantatthesignificancelevelofp≤0.01.
b ToperformthetestontheBMIvariable,thecategoriesofoverweightandobesityweregrouped.
greatestincidenceoffracturesamongtheirelderlypatients wasintheagerange from71to80 years(27.99%).Benetos etal.13observedthataround80%ofthehipfracturesoccurred inwomenovertheageof70years.Amongthemen,50%were overtheageof70years.Themeanageatwhichhipfractures occurred was81 yearsamongwomenand 78years among men.
Inrelationtosex,wefoundthat56(74.7%)werefemaleand 19(25.3%)weremale.AccordingtoEisleretal.,16 ina sam-pleof571patientswithproximalfracturesofthefemur,the observedincidencewas86%amongfemalesand14%among males.Pereiraetal.17alsofoundthatfemoralfractureswere predominantly amongwomen.Espinoetal.18 reportedthat theincidenceoffracturesinwomenwas66%andthatitwas
12.0
5.6
62.7
43.8
24.0 33.7
1.3 16.9
With fractures
Without fractures
Low weight Normal weight Overweight Obese
BMI classification
Fig.2–DescriptionofthesampleinvestigatedaccordingtothevariableofBMIclassificationforthegroupswithfractures (n=75cases)andwithoutfractures(n=89cases).
100.0
76.6
70.4
29.6
23.4 33.3
48.1 44.7
8.5
18.5 46.8
14.8 10.6
70.4
59.6
14.8
3.7 0.0 1.3 29.8
100.0 100.0
Femoral neck
Subtrochanteric
Trochanteric
Female Male Up to 70
years
From 71 to 80 years
Age Sex
Over 80 years
Obese Overweight
Normal weight Low weight
BMI classification
Fig.3–Comparisonofsex,BMIandageinrelationtothetypesoffracturethatoccurred,forthegroupwithfracturesalone (n=75cases).
Source:Datagatheredin2011.
34%inmen.Aharonoffetal.19foundthattheincidenceamong womenwas78.6%.Ramalhoetal.20notedthatfemoral frac-turesoccurredpredominantlyamongwomen.Benetosetal.13 foundthattheincidenceofhipfractureswastwiceashigh amongwomenthanamongmen.
Themaintypesoffracturepresentedinthis studywere trochanteric fractures,with 47 cases (62.2%), femoral neck fractures,with27cases(36%)andsubtrochantericfractures, withonecase(1.8%).Intheliterature,trochantericfractures arepresentedasthemostfrequenttype.CunhaandVeado21 analyzed190 patients (142women and 48 men;mean age of79years)inthestateofMinasGeraiswhowere hospital-izedwith fracturesinthe proximalextremityofthe femur intheorthopedicwardoftheStatePublicServants’Hospital, amongwhomtheincidenceoftrochantericfractureswas50%, femoralneckfractures44%andsubtrochantericfractures6%. IN relation to BMI, the patients were divided into four categories: low weight (<18.5kg/m2), normal weight (18.5–25kg/m2), overweight (25–30kg/m2) and obese (>30kg/m2). Among the patients with proximal fractures ofthefemur,12%presentedlowweight,62.7%normalweight, 24%overweight,and1.3%obesity.Amongthepatientswithout anyhistoryofproximalfracturesofthefemur,5.6%presented lowweight,43.8%normalweight,33.7%overweight,and9.8% obesity.Itwasfoundthatthepatientswithfracturesofthe proximalextremityofthefemur(n=75)presentedmeanBMI of22.6,whilethepatientswithoutfractures(n=89)presented meanBMIof25.5.
Astudy conductedbyAlfaro-Achaetal.1 alsoconfirmed thattherewasaninverserelationshipbetweenbodyweight and theriskoffracturing oftheproximal extremityofthe
femur and reported that a 10% weight loss significantly increasedthe risk ofhip fracturesamongindividuals aged 65 yearsandover.DeLaetet al.22 foundasmalldifference inthe riskoffracturesamongtheir patients,inrelationto anincreaseinBMIoffiveunits, from25kg/m2 to30kg/m2, thedifferenceobservedwasa17%decreaseintheriskofhip fractures.InrelationtoanincreaseinBMIoftenunits,the differenceobservedwasa25%decreaseintheriskofhip frac-tures.AtthelowerextremityoftheBMIspectrum,achange offiveBMIunitsfrom25kg/m2to20kg/m2correspondedto doublingtheriskofhipfractures.Folsometal.23confirmed thattherewasaninverserelationshipbetweenBMIand occur-rencesofhipfractures.Youngetal.24reportedthatlowBMI wasariskfactorforhipfractures,whilehighBMIwasa pro-tectivefactor.Margolisetal.25foundanassociationbetween lowBMIorbodysizeandincreasedriskofhipfractures.White etal.26onlydemonstratedabenefitfromincreasedBMIamong women,whiletherewasnochangeinriskamongmen. Holm-bergetal.27reportedthatincreasedBMIwasprotectiveagainst hipfracturesinbothmenandwomen.
Conclusion
thefemur,whichdirectlyinfluenceelderlypeople’squalityof lifeandindependence,earlydetectionofriskfactorsisneeded inordertoselecttreatmentsbetter,diminishthemorbidity andmortalityratesandreducecosts.Thesefactureshavea directbearingonsociety’seconomicsituation,giventhatthey leadtobillionsofdollarsofexpenditureonmedicalcare.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. Alfaro-AchaA,OstirGV,MarkidesKS,OttenbacherKJ. Cognitivestatus,bodymassindex,andhipfractureinolder Hispanicadults.JAmGeriatrSoc.2006;54(8):1251–5.
2. HintonRY,SmithGS.Theassociationofage,race,andsex withthelocationofproximalfemoralfracturesintheelderly. JBoneJointSurgAm.1993;75(5):752–9.
3. WorldHealthOrganization.Preventionandmanagementof osteoporosis.Geneva:WHOTechnicalReportSeries;2003.
4. KannusP,NiemiS,ParkkariJ,PalvanenM,VuoriI,JarvinenM. HipfracturesinFinlandbetween1970and1997and
predictionsforthefuture.Lancet.1999;353(9155):802–5.
5. KannusP,ParkkariJ,NiemiS,PasanenM,PalvanenM, JarvinenM,etal.Preventionofhipfractureinelderlypeople withuseofahipprotector.NEnglJMed.2000;343(21):1506–13.
6. HannanEL,MagazinerJ,WangJJ,EastwoodEA,Silberzweig SB,GilbertM,etal.Mortalityandlocomotion6monthsafter hospitalizationforhipfracture:riskfactorsandrisk-adjusted hospitaloutcomes.JAMA.2001;285(21):2736–42.
7. KannusP,ParkkariJ,SievanenH,HeinonenA,VuoriI, JarvinenM.Epidemiologyofhipfractures.Bone.1996;18 Suppl.1:57S–63S.
8. RichmondJ,AharonoffGB,ZuckermanJD,KovalKJ.Mortality riskafterhipfracture.JOrthopTrauma.2003;17(1):53–6.
9. SchwartsmannCR,OliveiraGK,OliveiraRK,BoschinLC, MothesFC,SilvaRC.Averdadeirafraturadocolodofêmur. ActaOrthopBras.2000;8(3):108–11.
10.MunizC,ArnautA,YoshidaM,TrelhaC.Caracterizac¸ãodos idososcomfraturadefêmurproximalatendidosemhospital escolapúblico.RevEspac¸oSaúde.2000;8(2):33–8.
11.BerralFJ,MorenoM,BerralCJ,ContrerasMEK,CarpinteroP. Composic¸ãocorporaldepacientesacamadosporfraturasdo quadril.ActaOrtopBras.2008;16(3):148–51.
12.CunhaDF,CunhaSFC,PilotoPE,SantosNP,BarrosJW.Estado nutricionalerespostadefaseagudaempacientescom fraturadoterc¸oproximaldofêmur.RevBrasOrtop.1998;33(4): 321–4.
13.BenetosIS,BabisGC,ZoubosAB,BenetouV,SoucacosPN. Factorsaffectingtheriskofhipfractures.Injury.
2007;38(7):735–44.
14.Vilas-BôasAJr,VercesiAE,BodachneL,VialleLRG.Estudo epidemiológicodefraturasdefemurproximalemidosos. ActaOrtopBras.1996;4(3):122–6.
15.RochaMA,CarvalhoWS,ZanquetaC,LemosSC.Estudo epidemiológicoretrospectivodasfraturasdofêmurproximal tratadosnoHospitalEscoladaFaculdadedeMedicinado TriânguloMineir.RevBrasOrtop.2001;36(8):311–6.
16.EislerJ,CornwallR,StraussE,KovalK,SiuA,GilbertM. Outcomesofelderlypatientswithnondisplacedfemoralneck fractures.ClinOrthopRelatRes.2002;(399):52–8.
17.PereiraGJC,BarrretoAA,CurcelliEC,PereiraHDR,GériosJC, GalväoMPL,etal.Estudoepidemiológicoretrospectivodas fraturasdoterc¸oproximaldofêmurnaregiãodeBotucatu. RevBrasOrtop.1993;28(7):504–10.
18.EspinoDV,PalmerRF,MilesTP,MoutonCP,WoodRC,Bayne NS,etal.Prevalence,incidence,andriskfactorsassociated withhipfracturesincommunity-dwellingolderMexican Americans:resultsoftheHispanicEPESEstudy.Establish PopulationfortheEpidemiologicStudyfortheElderly.JAm GeriatrSoc.2000;48(10):1252–60.
19.AharonoffGB,DennisMG,ElshinawyA,ZuckermanJD,Koval KJ.Circumstancesoffallscausinghipfracturesintheelderly. ClinOrthopRelatRes.1998;348:10–4.
20.RamalhoAC,Lazaretti-CastroM,HauacheO,VieiraJG,Takata E,CafalliF,etal.Osteoporoticfracturesofproximalfemur: clinicalandepidemiologicalfeaturesinapopulationofthe cityofSaoPaulo.SaoPauloMedJ.2001;119(2):48–53.
21.CunhaU,VeadoMAC.Fraturadaextremidadeproximaldo fêmuremidosos:independênciafuncionalemortalidadeem umano.RevBrasOrtop.2006;41(6):195–9.
22.DeLaetC,KanisJA,OdenA,JohansonH,JohnellO,DelmasP, etal.Bodymassindexasapredictoroffracturerisk:a meta-analysis.OsteoporosInt.2005;16(11):1330–8.
23.FolsomAR,KushiLH,AndersonKE,MinkPJ,OlsonJE,Hong CP,etal.Associationsofgeneralandabdominalobesitywith multiplehealthoutcomesinolderwomen:theIowaWomen’s HealthStudy.ArchInternMed.2000;160(14):2117–28.
24.YoungY,MyersAH,ProvenzanoG.Factorsassociatedwith timetofirsthipfracture.JAgingHealth.2001;13(4):511–26.
25.MargolisDJ,KantorJ,SantannaJ,StromBL,BerlinJA.Risk factorsfordelayedhealingofneuropathicdiabeticfoot ulcers:apooledanalysis.ArchDermatol.2000;136(12):1531–5.
26.WhiteSC,AtchisonKA,GornbeinJA,NattivA,Paganini-Hill A,ServiceSK.Riskfactorsforfracturesinoldermenand women:TheLeisureWorldCohortStudy.GendMed. 2006;3(2):110–23.