w w w . r b o . o r g . b r
Original
article
Effects
of
platelet-rich
plasma
on
lateral
epicondylitis
of
the
elbow:
prospective
randomized
controlled
trial
夽
Evandro
Pereira
Palacio
∗,
Rafael
Ramos
Schiavetti,
Maiara
Kanematsu,
Tiago
Moreno
Ikeda,
Roberto
Ryuiti
Mizobuchi,
José
Antônio
Galbiatti
FaculdadedeMedicinadeMarília,Marília,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17February2015
Accepted31March2015
Availableonline13January2016
Keywords:
Platelet-richplasma
Tendinopathy
Tenniselbow
a
b
s
t
r
a
c
t
Objective:Toevaluatetheeffectsofplatelet-richplasma(PRP)infiltrationinpatientswith
lateralepicondylitisoftheelbow,throughanalysisoftheDisabilitiesoftheArm,Shoulder
andHand(DASH)andPatient-RatedTennisElbowEvaluation(PRTEE)questionnaires.
Methods:Sixtypatientswithlateralepicondylitisoftheelbowwereprospectively
random-izedandevaluatedafterreceivinginfiltrationofthreemillilitersofPRP,or0.5%neocaine,
ordexamethasone.Forthescoringprocess,thepatientswereaskedtofillouttheDASH
andPRTEEquestionnairesonthreeoccasions:onthedayofinfiltrationand90and180days
afterwards.
Results:Around 81.7% of the patients who underwent the treatment presented some
improvementofthesymptoms.Thestatisticaltestsshowedthattherewasevidencethat
thecureratewasunrelatedtothesubstanceapplied(p=0.62).Therewasalsointersection
betweentheconfidenceintervalsofeachgroup,thusdemonstratingthattheproportionsof
patientswhosesymptomsimprovedweresimilarinallthegroups.
Conclusion:Atasignificancelevelof5%,therewasnoevidencethatonetreatmentwasmore
effectivethananother,whenassessedusingtheDASHandPRTEEquestionnaires.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
夽
WorkdevelopedintheDepartmentofOrthopedics,TraumatologyandSportsandExerciseMedicine,FaculdadedeMedicinadeMarília
(FAMEMA),Marília,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](E.P.Palacio).
http://dx.doi.org/10.1016/j.rboe.2015.03.014
Efeitos
do
plasma
rico
em
plaquetas
na
epicondilite
lateral
do
cotovelo:
estudo
prospectivo,
randomizado
e
controlado
Palavras-chave:
Plasmaricoemplaquetas
Tendinopatia
Cotovelodotenista
r
e
s
u
m
o
Objetivo: Avaliarosefeitosdainfiltrac¸ãodoplasmaricoemplaquetas(PRP)empacientes
comepicondilitelateraldocotovelo(ELC) pelaanálisedosquestionários Deficiênciado
Brac¸o,OmbroeMão(Dash)eAvaliac¸ãodoPacientePortadordoCotovelodeTenista(PRTEE).
Métodos: Foramrandomizadoseavaliadosprospectivamente60pacientes,apósreceberem
infiltrac¸õesdetrêsmililitrosdePRP,ouneocaína0,5%,oudexametasona.Paraoprocesso
depontuac¸ão,ospacientesforamconvidadosapreencherosquestionáriosDashePRTEE
emtrêsocasiões:nodiadainfiltrac¸ão,90e180diasapós.
Resultados: Dospacientessubmetidosaotratamento,81,7%apresentarammelhoriados
sintomas.Ostestesestatísticosdemonstraramqueháevidênciasdequeataxadecura
nãoestárelacionadacomasubstânciaaplicada(p=0,62).Houvetambémintersec¸ãodos
intervalosdeconfianc¸adecadagrupo,comdemonstrac¸ãodequeasproporc¸õesdepacientes
cujossintomasmelhoraramforamsemelhantesemtodososgrupos.
Conclusão: Emumníveldesignificânciade5%,nãohouveevidênciadequeumtratamento
foimaiseficazdoqueaoutro,quandoavaliadospelosquestionáriosDashePRTEE.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Todososdireitosreservados.
Introduction
Lateral epicondylitis ofthe elbow isa disease that mainly
affectsindividualswhomakerepetitivemovementswiththeir
wrists and/or fingers.1 The name “tennis elbow” does not
correspondtothereality.Althougharound40–50%oftennis
playerspresentthisdisease,especiallythosewhohavebeen
practicingthis sport forlongertimes,2 thisgroup accounts
foronly 5% ofthe total number of individuals affected.3,4
Althoughtheterm “lateralepicondylitisofthe elbow”may
alsobeinappropriate,giventhatthispathologicalcondition
doesnotinvolveatrulyinflammatoryprocess,butrather,a
degenerativeprocess,5–8itwillbeusedinthisstudybecause
ithasbeenwidelydisseminatedintheliterature.
Thisinjurypredominantlyinvolvestheoriginoftheshort
radialextensor muscle of the carpus, inwhich microtears
developasaresultofexcessiveandabnormaluse,with
for-mationofimmaturerepairtissue.5
Thesymptomsoflateralepicondylitisoftheelboware
gen-erallyself-limitedandmayvaryindurationfromafewweeks
tomonths.However,insomecases,thereisnospontaneous
resolutionofthe symptoms, and this invariably leadsto a
chroniccondition.9,10Italsohastobeborneinmindthat
lat-eralepicondylitisoftheelbowisassociatedwithlongperiods
offwork,whichgivesrise tohighsocialsecuritycostsand
substantiallossofprofessionalproductivity.11–14
There isrelatively little evidencebased on good-quality
clinicalstudiestosupportthevariousformsoftreatmentfor
lateral epicondylitisofthe elbowthat havebeen described
in the literature. The treatment options range from
rela-tiverest inassociationwithimmobilization,physiotherapy,
application of botulinum toxin, acupuncture, shockwave
therapy,use oforalnon-steroidal anti-inflammatorydrugs,
steroid injections and, most recently, use of platelet-rich
plasma.15–20Surgicalproceduresareonlyrecommendedwhen
thesymptomslastformorethansixmonthsand/orifother
non-surgicaltreatmentoptionshavefailed.5,17,20
Giventhehighincidenceofthisdisease,theexpenditure
thatresultsfromitstreatmentand,especially,thelackof
con-sensusinthedifferentdatabasesavailableandinparticular
theBrazilianorthopedicdatabases,weproposedthepresent
study.Itsaimwastoprospectivelycomparetheresultsfrom
threedifferentoptionsfortreatinglateralepicondylitisofthe
elbow,usingtheDASHandPRTEEquestionnaires,whichhave
recentlybeentranslatedandvalidatedforuseinPortuguese.
Material
and
methods
Participantsandstudydesign
TheprotocolforthisstudywasapprovedbytheEthics
Com-mitteeforResearchInvolvingHumanBeings,underno.453/12.
All the patients or theirguardians agreed toparticipatein
thestudythroughsigningafreeandinformedconsent
state-ment,afterhavingbeengivendetailedinformationaboutthe
contentandformofthestudy.
Thesamplesizewasdeterminedbeforestartingthestudy.
The˛andˇrisks(respectively5%and20%)andthevariability
ofthevariables(p1=0.2andp2=0.63)weretakenintoaccount,
andaminimumnumberof20participantspergroupwasthus
determined.
BetweenFebruary2012andFebruary2014,72consecutive
patientswithlateralepicondylitisoftheelbowwereselected
for the study. The inclusion criteria were a minimum age
of18years andpositivefindings fromtwoofthefollowing
clinical tests: Cozen, Mill, Gardnerand Maudsley. The
fol-lowing patients were excluded: those who had undergone
who presentedother diseases inthe upperlimbs(such as
posteriorinterosseousnervesyndromeand/orcarpaltunnel
syndrome): patients with systemic diseases (such as
dia-betesmellitus,hypothyroidismand/orrheumatoidarthritis);
pregnant patients; and lastly, patients using contraceptive
drugs.10,11 Ultrasoundexaminationswereperformedonlyto
documentthecasesandformanimagedatabase.Through
applying the criteria, 60 patients were included in this
study.
Instruments
Theinstrumentsmostusedformeasuringthefunctionality
anddegreeofimpairmentofpatients’ elbowregionarethe
DisabilitiesoftheArm,ShoulderandHand(DASH)
question-naireandthePatient-RatedTennisElbowEvaluation(PRTEE).
Both of these instruments have been validated for use in
Portuguese.TheDASHquestionnairemeasuresthe
incapac-ity of the upper limb as a single unit, always from the
patient’s perspective.12,14,15 On the other hand, the PRTEE
wasdevelopedsolelytoevaluatelateralepicondylitisofthe
elbow.
Both questionnaires were applied to all the patients at
threedifferenttimes:onthedayofinfiltration(DASH-0and
PRTEE-0),90daysafterwards(DASH-90andPRTEE-90)and180
daysafterwards(DASH-180andPRTEE-180).
Blindingandrandomizationprocess
Withtheaimofensuringgreaterreliabilityfortheresultsand
greater investigativepower forthe study,itwas decidedto
instituteaprocessoftripleblinding.
Therandomization process consisted of the method of
sealedopaqueenvelopes.21,22Theallocationgroupwasstated
insideeachenvelope:groupA(n=20;5%neocaine),groupB
(n=20;dexamethasone)andgroupC(n=20;PRP).
Preparationandapplicationofplatelet-richplasma
ThePRPusedinthisstudywasobtainedasrecommendedby
Vendraminet al.23 60mlofbloodthat hadpreviouslybeen
takenfromeachpatientwasdividedbetweensix10mltubes
thatcontainedsodium citrate.Thesetubes werethen
sub-jectedtotwocyclesofcentrifugation,underforcesof400g
and800g,for10min.
Twothirdsoftheoriginal volume(platelet-poorplasma)
wasdiscardedinthismethod.Onlyonethirdoftheoriginal
bloodsampleconsistedofPRP(Fig.1).
Fingerpressurewasappliedlocallytothepatientssothat
theycouldidentifytheregionofgreatestpain(Fig.2).Before
placementofsterileocularfields,asepsisandantisepsis
pro-cedureswereperformedusingchlorhexidine.Thepatientsin
groupAthenunderwentlocalinfiltrationof3mlof0.5%
neo-caine;groupBreceivedinfiltrationof3mlofdexamethasone
acetate;andgroupCreceivedinfiltrationof3mlof
platelet-richplasma.Allthesyringeswerecoveredwithadoublelayer
ofaluminumfoil,fortheinfiltrationprocedure,byaperson
whowasunconnectedtothestudy.
Fig.1–Preparationoftheplatelet-richplasma.
Fig.2–Identificationoftheinfiltrationsite(circled)andthe posteriorinterosseousnerve(PIN).
Statisticalanalysis
To perform the statistical calculations, the software used
comprised SigmaStat® 3.5 (Systat Software Inc., 2006) and
Minitab®version15(MinitabInc.,2007),Thesignificancelevel
wastakentobe5%(p<0.05).
The variables were analyzed by means of descriptive,
parametric and nonparametric statistical tests in a fully
randomized model.Theparametric option was usedwhen
the variable presented Gaussian behavior (Student’s t test
andANOVA).Ifthedistributionwasnon-Gaussian,the
non-parametricoptionwasindicated(Mann–WhitneyUtestand
Fisher’s exact test).The mean values, standard deviations,
medians,frequencies,percentagesand95%confidence
90
80
70
60
50
40
30
20
10
Group C Group B
Group A
Age (years)
Fig.3–Agesofthepatientsinthegroups(Kruskal–Wallis; p=0.99).
Results
TheagesingroupArangedfrom22to85years(mean:47.9;
95%CI:42.2–53.6years);ingroupBtherangewasfrom19to
61years(mean:46.2;95%CI:41–51.5years);andingroupCit
wasfrom26to61years(mean:46.6;95%CI:41.6–51.6years)
(Kruskal–Wallis;p=0.99)(Fig.3).
Inallthreegroups,thescoreintheDASH-90questionnaire
waslowerthanthescoreinDASH-0,althoughthemaximum
valuesfoundinDASH-90weregreaterthanthoseinDASH-0.
Thisdiscrepancycanbeexplainedbythescoresattributedto
asinglepatient,which reached75.8 and80.8 pointsinthe
DASH-0 and DASH-90questionnaires,respectively.
Further-more,anotherparticipanthadalowerscoreinDASH-0(34.2)
thaninDASH-90(37.5).Forthesamereasons,slightlyhigher
standarderrorvaluescanbeseeninDASH-90thaninDASH-0
Table1–ScoresfromtheDASH-0questionnairesinthe threegroups.
Group Minimum score
Maximum score
Median Mean Standard error
A 25.0 73.3 49.2 49.7 3.0
B 15.0 75.8 40.4 44.3 4.4
C 22.5 82.5 40.8 45.7 3.8
Table2–ScoresfromtheDASH-90questionnairesinthe threegroups.
Group Minimum score
Maximum score
Median Mean Standard error
A 0.8 71.7 10.2 16.6 3.8
B 0.0 80.8 12.1 19.8 4.9
C 1.7 79.2 5.0 10.7 4.0
Table3–ScoresfromthePRTEE-0questionnairesinthe threegroups.
Group Minimum score
Maximum score
Median Mean Standard error
A 18.0 82.5 52.5 51.7 4.4
B 17.0 83.5 35.8 42.9 4.3
C 24.5 88.5 37.0 47.1 4.9
Table4–ScoresfromthePRTEE-90questionnairesinthe threegroups.
Group Minimum score
Maximum score
Median Mean Standard error
A 1.5 80.0 9.5 15.5 3.9
B 0.0 85.0 12.8 21.8 5.5
C 0.5 91.5 6.5 13.0 4.7
Table5–DifferencebetweentheDASH-0andDASH-90 questionnaires(scores≥15).
Group n % Standarderror 95%CI
A 20 90.0 6.8 [68.3–98.8]
B 20 65.0 10.9 [40.8–94.6]
C 20 90.0 6.8 [68.3–98.8]
(Tables1and2).ThevaluesfromtheDASH-180questionnaires
weretakentobezeroinallthreegroups.
InrelationtothePRTEEquestionnaire,itwasnotedthatin
allthreegroups,thescoresrelatingtoPRTEE-90werelower
than those of PRTEE-0. However, the maximum scores in
groupsBandCwerehigherinPRTEE-90thaninPRTEE-0.This
discrepancycanbeexplainedbythescoresofasingle
par-ticipant who reached65.5 points(PRTEE-0)and 85.0 points
(PRTEE-90),bothingroupB;andanotherpatientwhoreached
scoresof83.0(PRTEE-0)and91.5(PRTEE-90),bothingroupC.
Itisalsoimportanttonotethatanotherfiveindividuals
pre-sentedhigherscoresinPRTEE-90(twoingroupA,twoingroup
BandoneingroupC)(Tables3and4).Thevaluesfromthe
PRTEE-180questionnairesweretakentobezeroinallthree
groups.
Table5showstheabsolutequantity(n)andproportion(%)
ofthepatientswhoreportedachievingsomeimprovementin
symptoms,asdemonstratedbyadifferencegreater thanor
equalto15points(binomialdistribution)betweenthe
DASH-0andDASH-90questionnaires.ThevaluesfromthePRTEE-180
questionnairesweretakentobezeroinallthreegroups.
Overall,81.7%ofthepatientshadsomeimprovementin
their symptoms. In groups Aand C,there were reportsof
improvementin90%ofthecasesandingroupBthe
propor-tionwas65%(p=0.62).INotherwords,therewasevidencethat
theproportionofcarewasunrelatedtothesubstanceused,at
thesignificancelevelof5%.Moreover,theconfidenceintervals
correlatedbetweenthegroups,whichshowsthatthe
propor-tionofimprovementofsymptomswasthesameinthethree
groups.
InordertoconfirmtheresultsfromtheDASH
question-naires, the proportions ofimprovementwere matches and
comparedusingStudent’sttest.ForthepairingsA/BandB/C,
theproportionswerestatisticallythesame(p=0.56),andalso
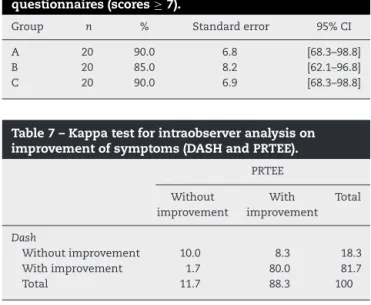
Table6–DifferencebetweenthePRTEE-0andPRTEE-90 questionnaires(scores≥7).
Group n % Standarderror 95%CI
A 20 90.0 6.8 [68.3–98.8]
B 20 85.0 8.2 [62.1–96.8]
C 20 90.0 6.9 [68.3–98.8]
Table7–Kappatestforintraobserveranalysison improvementofsymptoms(DASHandPRTEE).
PRTEE
Without improvement
With improvement
Total
Dash
Withoutimprovement 10.0 8.3 18.3
Withimprovement 1.7 80.0 81.7
Total 11.7 88.3 100
ImprovementofthesymptomsinthePRTEEquestionnaire wasdefinedasadifferenceinscoresbetweenthe question-nairesgreaterthanorequalto7points.Inthisstudy,90%of theparticipantsingroupsAandCreportedachieving improve-ments, as did 85% in group B. The test of independence betweenthe groups did notpresent statistical significance (p=0.85)(Table6).InthesamewayasintheDASH
question-naire,therewasevidencethattheproportionthatachieveda
curedidnotdependonthesubstanceused,atthesignificance
levelof5%.
Once again, in order to confirm the results from the
PRTEEquestionnaires,theproportionsofimprovementwere
matchedandcomparedusingStudent’sttest.Inrelationtothe
pairingsA/B,B/CandA/C,theproportionswerestatistically
thesame(p=0.66).
Table7showstheresultsfromthe kappatest, for
inter-observeragreementrelatingtothequestionnairesthatwere
applied.Itcould be seenthat there wassubstantial
agree-mentbetweenthetwoquestionnaires(p=0.6).Inrelationto
theinternalconcordanceofthe questionnaires,Cronbach’s
alphatestshowed thattherewas consistencybetweenthe
questionnaires(p=0.8).
Discussion
Visualanaloguescales(VAS)forassessingpainarethemost
commonly used method for measuring painful conditions
becausetheyarequicklyandeasilyapplied.However,using
VASpresents practicallimitations withinclinical scenarios,
giventhatmostpatientsreport thattheyhavedifficulty in
translatingthephysicalintensityoftheirpainintoascalein
millimeters.20
SeveralmechanismsofactionforPRPhavebeendescribed
in the literature. In principle, these explain the clinical
improvementoftheparticipantsinthisstudy:thelocal
hemo-staticactionofthesubstanceduringthepostoperativeperiod,
alongwithitsinfluenceonosteogenesisandsoft-tissue
heal-ing,especiallymusclehealing.11Thereisalsothehypothesis
thatautologousbloodinjectionshaveadirectinfluenceonthe
cascadeofinflammationandcauseanearlystarttorecovery
ofthedegeneratedtissue.10
Local infiltration ofcorticosteroids, which is considered
by many surgeons to be the best option for treating
lat-eral epicondylitisofthe elbow,hasbeen questioned.Some
authors have suggestedthat the improvementobservedin
thesepatientsonlyhaspartialandtemporaryefficacy.16
Althoughsomeauthors12 havereportedthatapplication
of PRP is the most promising method for treating lateral
epicondylitis oftheelbow,the present studyproduced
dis-couragingresultsfromprospectiveanalysisontwodifferent
validated assessmentscales,inrelationtothe increasingly
fashionableuseofPRP.Therewasnostatisticallysignificant
differencebetweentheformsoftreatmentoverthe180days
offollow-up ofthe patients(Tables5and 6).Moreover,the
improvementinsymptomsseenoverthecourseofthestudy
periodwasshowntobestatisticallythesame forthethree
substances(Table7).
However, it isimportant toemphasize that whenmore
thantwoperitendinousinfiltrationsareapplied,some
unde-sirablesideeffectssuchaslocalnecrosis,tissueatrophyand
tendontearingmayoccur.1,8,13Thesemaybetherealreason
why medicalprofessionalsprefer toapplyPRP, rather than
corticosteroids.
Conclusion
Thisstudy didnotsupplyany statisticalevidencethat PRP
mightprovidebetterresultsthantreatmentwith
corticoste-roidsorlocalanesthetic,intreatinglateralepicondylitisofthe
elbow.
On the other hand, there was statistical agreement
between the DASH and PRTEE scales. The
Portuguese-languageversionsofbothquestionnaireswereshowntobe
effectiveforevaluatingtheevolutionofthedisease.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Weare gratefultothe ResearchSupportFoundationofthe
StateofSãoPaulo(Fundac¸ãodeAmparoàPesquisadoEstado
deSãoPaulo,FAPESP),throughproceduralnos.2012/19254-0
and2012/19291-2,foritssupportindevelopingthisstudy.
r
e
f
e
r
e
n
c
e
s
1.MishraA,PavelkoT.Treatmentofchronicelbowtendinosis withbufferedplatelet-richplasma.AmJSportsMed. 2006;34(11):1774–8.
2.GruchowHW,PelletierD.Anepidemiologicstudyoftennis elbow:incidence,recurrence,andeffectivenessofprevention strategies.AmJSportsMed.1979;7(4):234–8.
4. LechO,PiluskiPCF,SeveroAL.Epicondilitelateraldocotovelo. RevBrasOrtop.2003;38(8):421–36.
5. NirschlRP,PettroneFA.Tenniselbow.JBoneJointSurgAm. 1979;61(6):832–9.
6. ReganW,WoldLE,CoonradR,MorreyBF.Microscopic histopathologyofchronicrefractorylateralepicondyliitis.Am JSportsMed.1992;20(6):746–9.
7. GeoffroyP,YaffeMJ,RohanI.Diagnosingandtreatinglateral epicondylitis.CanFamPhysician.1994;40:73–8.
8. FredbergU,Stengaard-PedersenK.Chronictendinopathy tissuepathology,painmechanisms,andetiologywitha specialfocusoninflammation.ScandJMedSciSports. 2008;18(1):3–15.
9. ShiriR,Viikari-JunturaE.Lateralandmedialepicondylitis: roleofoccupationalfactors.BestPractResClinRheumatol. 2011;25(1):43–57.
10.ThanasasC,PapadimitriouG,CharalambidisC, ParaskevopoulosI,PapanikolaouA.Plateletrichplasma versusautologouswholebloodforthetreatmentofchronic lateralelbowepicondylitis.AmJSportsMed.
2011;39(10):2130–4.
11.Walker-BoneK,PalmerKT,ReadingIC,CoggonD,CooperC. Occupationandepicondylitis:apopulation-basedstudy. Rheumatology(Oxf).2012;51(2):305–10.
12.BuchbinderR,RichardsBL.Islateralepicondylitisanew indicationforbotulinumtoxin?CanMedAssocJ. 2010;182(8):749–50.
13.RempelDM,HarrisonRJ,BarnhartS.Disordersoftheupper extremity.JAmMedAssoc.1992;267(6):838–42.
14.SilversteinB,AdamsD.Work-relatedmusculoskeletal disordersoftheneck,back,andupperextremityin WashingtonState,2005.Olympia,Washington:SHARP Program,WashingtonStateDepartmentofLaborand Industries;2007.
15.JohnsonGW,CadwalladerK,ScheffelSB,EpperlyTD. Treatmentoflateralepicondylitis.AmFamPhys. 2007;76(6):843–8.
16.SmidtN,vanderWindtDA,AssendelftWJ,DevilléWL, Korthals-deBosIB,BouterLM.Corticosteroidinjection, physiotherapy,orwait-and-seepolicyforlateralepicondylitis: arandomisedcontrolledtrial.Lancet.2002;359(9307): 657–62.
17.StrujisPAA,BosIBCK,vanTulderMW,vanDijkCN,Bouter LM,AssendelftWJJ.Costeffectivenessofbrace,
physiotherapy,orbothfortreatmentoftenniselbow.BrJ SportsMed.2006;40(7):637–43.
18.OlaussenM,HolmedalØ,LindbaekM,BrageS.Physiotherapy aloneorincombinationwithcorticosteroidinjectionfor acutelateralepicondylitisingeneralpractice:aprotocolfora randomised,placebo-controlled-study.BMCMusculoskelet Disord.2009;10:152.
19.GalvinR,CallaghanC,ChanWS,DimitrovBD,FaheyT. Injectionofbotulinumtoxinfortreatmentofchroniclateral epicondylitis:systematicreviewandmeta-analysis.Semin AthritisRheum.2011;40(6):585–7.
20.WongSM,HuiACF,TongP,YuE,WongLKS.Treatmentof lateralepicondylitiswithbotulinumtoxin:arandomized, double-blind,placebo-controlledtrial.AnnInternMed. 2005;143(11):793–7.
21.DoigGS,SimpsonF.Randomizationandallocation concealment:apracticalguideforresearches.JCritCare. 2005;20(2):187–91.
22.AltmanDG,SchulzKF.Statisticsnotes:concealingtreatment allocationinrandomisedtrials.BMJ.2001;323(7310): 446–7.