w w w . r b o . o r g . b r
Original
article
Are
the
good
functional
results
from
arthroscopic
repair
of
massive
rotator
cuff
injuries
maintained
over
the
long
term?
夽
Alberto
Naoki
Miyazaki
∗,
Pedro
Doneux
Santos,
Luciana
Andrade
da
Silva
∗,
Guilherme
do
Val
Sella,
Sérgio
Luiz
Checchia,
Alexandre
Maris
Yonamine
FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12February2015 Accepted19February2015 Availableonline30December2015
Keywords: Rotatorcuff
Arthroscopy/method Evaluationstudies
a
b
s
t
r
a
c
t
Objective:Toevaluatewhetherthegoodandexcellentfunctionalresultsfromarthroscopic repairofmassiverotatorcufftearsaremaintainedoverthelongterm.
Methods:Fromthesampleofthestudyconductedbyourgroupin2006,inwhichwe evalu-atedthefunctionalresultsfromarthroscopicrepairofmassiverotatorcufftears,35patients werereassessed,8yearsafterthefirstevaluation.Theinclusioncriteriawerethatthese patientswithmassiverotatorcufftearsoperatedbymeansofanarthroscopictechnique, whoparticipatedinthepreviousstudyandachievedgoodorexcellentoutcomesaccording totheUCLAcriteria.Patientswhoseresultswerenotgoodorexcellentinthefirstevaluation accordingtotheUCLAcriteriawereexcluded.
Results:Amongthe35patientsreassessed,91%ofthemcontinuedtopresentgoodand excellentresults(40%excellentand51%good),while3%presentedfairresultsand6%poor results.Thetimeintervalbetweenthefirstandsecondevaluationswas8yearsandthe minimumlengthoffollow-upsincetheimmediatepostoperativeperiodwas9years(range: 9–17years),withanaverageof11.4years.
Conclusion:Thegoodandexcellentresultsfromarthroscopicrepairofmassiverotatorcuff tearsweremostlymaintained(91%),withthesameleveloffunctionandsatisfaction,even though8yearshadpassedsincethefirstassessment,withafollow-upperiodaveraging11.4 years.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedintheDepartmentofOrthopedicsandTraumatology,FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo (DOT-FCMSCSP),SãoPaulo,SP,Brazil.
∗ Correspondingauthors.
E-mails:[email protected](A.N.Miyazaki),[email protected](L.A.daSilva). http://dx.doi.org/10.1016/j.rboe.2015.12.009
Os
bons
resultados
funcionais
do
reparo
artroscópico
das
lesões
extensas
do
manguito
rotador
mantêm-se
em
longo
prazo?
Palavras-chave: Bainharotadora Artroscopia/método Estudosdeavaliac¸ão
r
e
s
u
m
o
Objetivos: Avaliarseosbonseexcelentesresultadosfuncionaisdoreparoartroscópicodas lesõesextensasdomanguitorotadorsemantêmemlongoprazo.
Métodos: Apartirdaamostradotrabalhofeitopornossogrupoem2006,noqualavaliamos os resultadosfuncionaisdoreparoartroscópicodaslesõesextensasdomanguito rota-dor, foram reavaliados 35 pacientes, totalizando oito anos após a primeira avaliac¸ão. Critériosdeinclusão:pacientescomlesãoextensadomanguitorotadoroperadospor téc-nicaartroscópicaqueparticiparamdotrabalhoanteriorequeobtiverambonsouexcelentes resultadossegundooscritériosdaUCLA.Critériosdeexclusão:pacientesquenãoobtiveram resultadobomouexcelentesegundooscritériosdaUCLAnaprimeiraavaliac¸ão.
Resultados: Dos35pacientesreavaliados,91%mantiveram-secombonseexcelentes result-ados(40%excelentes,51%bons),3%regularese6%ruins.Ointervalodetempoentrea primeiraeasegundaavaliac¸ãofoideoitoanos,otempodeseguimentomínimodesdeo pós-operatórioimediatofoidenoveanos,variouentrenovee17anoscommédiade11,4. Conclusão: Osbonseexcelentesresultadosdoreparoartroscópicodaslesõesextensasdo manguitorotadormantiveram-seemsuamaioria(91%)comomesmoníveldefunc¸ãoe satisfac¸ãomesmoapósoitoanosdesuaprimeiraavaliac¸ão,totalizandotempode segui-mentocommédiade11,4anos.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Rotator cuffinjuries are considered tobe oneofthe com-monestdiseasesoftheshoulder.1Theirincidenceisgreatest amongwomenintheagegroupbetween55and60years1and theymayhaveeithertraumaticordegenerativeorigin.2,3They canbeclassified accordingto theirsizeassmall,medium, large or extensive.4 When small injuries are not properly treated,theymayevolvetoextensiveinjuriesthatarea chal-lengetotreat,evenforexperiencedsurgeons.
Whensurgery isindicatedfortreating extensiverotator cuffinjuries,thisinvolvesgreattechnicalcomplexitybecause ofthepoorqualityand/orretractionofthetendon,whichadds difficultytotherepair.5–8
Throughimprovementsinarthroscopictechniques,ithas becomepossibletotreattheseinjurieslessinvasively,without aggression to the deltoid musculature. Earlier rehabilita-tion and alower complication ratehave thusalso become possible.9–12 Despite thehigh rerupturerate,13 arthroscopic repairofextensiverotator cuffinjuriesleadstogood func-tionalresultswithahighsatisfactionrate.14–16
However,itneedstobeaskedwhetherthesegoodresults wouldbemaintainedoverthelongterm.Intheliterature,the numberofstudiesshowinggoodresultsfromthistechnique, withlong-termfollow-up,remainssmall.5,13,17
In2006,ourgroupevaluated61casesofextensiverotator cuff injuries that underwent arthroscopic repair. Accord-ing to the UCLA criteria, 89% of the results were good or excellent.14,18
Withthe aimofmaking along-termassessment ofour clinicalresults8yearsaftertheoperations,weproposed to
reevaluatethesame groupofpatientsthatweevaluatedin 2006,toascertainwhethertheresultshadbeenmaintained.
Sample
and
methods
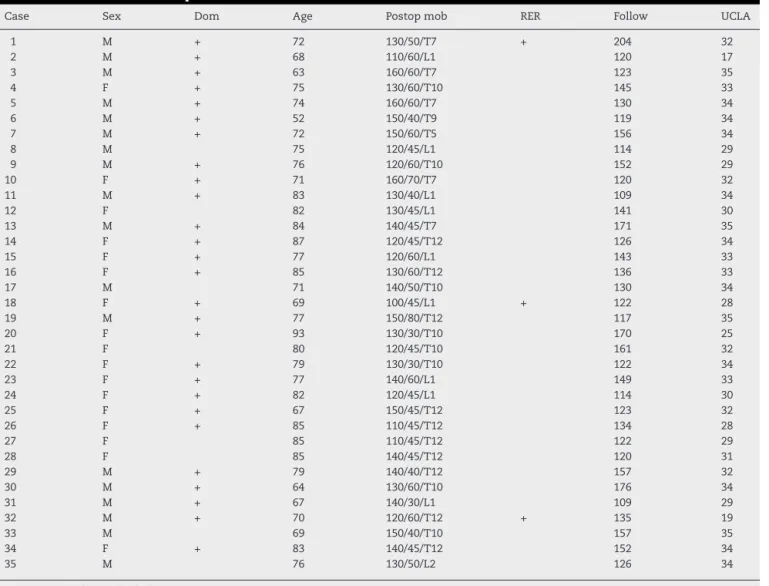
InAugust2006,ourinstitution’sshoulderandelbowsurgery group evaluated the resultsfrom treating 61 patients with extensive rotator cuff injuries who had undergone opera-tionsusinganarthroscopictechnique.14Fromthatgroup,the patientswhoseresultsweregoodorexcellentwereselectedin ordertoassesswhethertheseresultsweremaintained8years later.Therefore,theinclusioncriteriawerethatthepatients neededtohavepresentedextensiverotatorcuffinjuriesthat weretreatedarthroscopicallyandwereincludedinthe previ-ousstudy,andthattheresultsobtainedweregoodorexcellent accordingtotheUCLAcriteria.18Patientswhoseresultswere notgoodorexcellent atthefirstevaluationandthosewho could notbecontactedforthe reevaluationwere excluded. Withthesecriteria,outoftheinitialgroupof61patients,53 whohadbeen classifiedashavinggoodorexcellentresults wereincludedinthepresentstudy.Amongthese,itwasonly possibletoreevaluate35.Thesampleloss(18patients;33%) wascomposedof15patientswhocouldnotbelocated,two deathsandonepatientwhorefusedtotakepartinthe inves-tigation(Table1).
Thelengthoftime betweenthefirstevaluationand the reevaluationwas8years.Theminimumlengthoffollow-up sincethepostoperativeperiodwas9years,witharangefrom 9to17years(meanof11.4years)(Table1).
Table1–Clinicaldataonthepatients.
Case Sex Dom Age Postopmob RER Follow UCLA
1 M + 72 130/50/T7 + 204 32
2 M + 68 110/60/L1 120 17
3 M + 63 160/60/T7 123 35
4 F + 75 130/60/T10 145 33
5 M + 74 160/60/T7 130 34
6 M + 52 150/40/T9 119 34
7 M + 72 150/60/T5 156 34
8 M 75 120/45/L1 114 29
9 M + 76 120/60/T10 152 29
10 F + 71 160/70/T7 120 32
11 M + 83 130/40/L1 109 34
12 F 82 130/45/L1 141 30
13 M + 84 140/45/T7 171 35
14 F + 87 120/45/T12 126 34
15 F + 77 120/60/L1 143 33
16 F + 85 130/60/T12 136 33
17 M 71 140/50/T10 130 34
18 F + 69 100/45/L1 + 122 28
19 M + 77 150/80/T12 117 35
20 F + 93 130/30/T10 170 25
21 F 80 120/45/T10 161 32
22 F + 79 130/30/T10 122 34
23 F + 77 140/60/L1 149 33
24 F + 82 120/45/L1 114 30
25 F + 67 150/45/T12 123 32
26 F + 85 110/45/T12 134 28
27 F 85 110/45/T12 122 29
28 F 85 140/45/T12 120 31
29 M + 79 140/40/T12 157 32
30 M + 64 130/60/T10 176 34
31 M + 67 140/30/L1 109 29
32 M + 70 120/60/T12 + 135 19
33 M 69 150/40/T10 157 35
34 F + 83 140/45/T12 152 34
35 M 76 130/50/L2 126 34
Source:Hospital’smedicalfiles.
M,male;F,female;Dom,dominantside;Postopmob,postoperativemobility;RER,rerupture;Follow,follow-upinmonths.
arangefrom52to93years.Thedominantsidewasaffected in28cases(80%).Amongtheinjuries,30(85%)resultedfrom traumaorphysicalforceontheshoulder(Table1).
Amongthe 35 patients, 27 (77%)had injuriesthat fully or partially compromised the insertion of the tendon of thesubscapularismuscle,alongwithinjurytothe tendons ofthesupraspinatus and infraspinatus.Acromioplastywas performedon 30 patients(85%) and resectionofthe distal extremity oftheclavicle onseven(20%). In relationtothe longheadofthebicepsbrachii,tenotomyfollowedby tenode-siswasperformedin14cases,tenotomyaloneinfivecases andthetendonwasnotinthebicipitalgrooveinanotherfive cases.
Inallthepatients,suturingofthelesionwasperformedby meansofanchors.Thenumberofanchorsusedrangedfrom twotofive,withameanofthree.Thenumberofstitchesused rangedfrom fivetoten,withameanofseven.In31cases, tendon-to-tendonstitcheswere alsoused, inordertobring theedgesofthelesiontogether,beforesuturingtothebone. Ameanoftwotendon-to-tendonstitcheswasused,witha rangefromonetofourstitches.
Between May and October 2014, all the patients were reassessedclinicallybymeansoftheUniversityofCalifornia atLosAngeles(UCLA)method,18andtheirjointmobilitywas reevaluatedusingtheparametersdescribedbyHawkinsand Bokos19(Table1).
Toevaluatewhetherthegroupofpatientsstudiedwas dif-ferenttothegroupofpatientslost(around33%ofthesample), wecomparedthevariablesofsex,ageanddominancebetween thetwogroupsinordertodiminishthebiasintheresults.To comparethevariablesofsexanddominance,Fisher’sexact testwasused,andtocomparethemeanages,Student’sttest wasused.Theassumptionofequalvarianceswasmade,given thattheadherenceofagetonormaldistributioninthetwo groupswastestedbymeansoftheAnderson–Darlingtestand equalityofvariancebytheFtest.
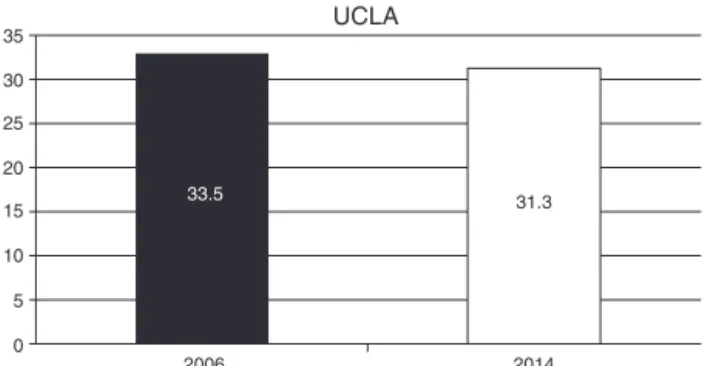
35
30
25
20
15
10
5
0
2006 2014
31.3 33.5
UCLA
Fig.1–FunctionalevaluationaccordingtotheUCLA criteria:changeinmeanvaluesfrom2006to2014.
excellentgroupandafairandpoorgroup,Fisher’sexacttest ofindependencewasused.
Allthetestswereperformedwithasignificancelevelof5% (p≥0.05).
Thisstudywasapprovedbyourhospital’sethicscommittee underthenumberCAAE3091491.4.4000.5479.
Results
Invalidatingthe sample,the group withoutfollow-up was composed of 18 patients and the group investigated was composedof35patients.Therewasnodifferenceinthe distri-butionsofsex(p=0.773)ordominance(p=0.464)betweenthe twogroups.Makingtheassumptionsthattherewas adher-encetonormaldistributionforthevariableofageinthetwo groups(p=0.619andp=0.631)andthattherewasequalityof variance(p=0.569),Student’sttestdidnotrejectthe hypoth-esis ofequalitybetweenthe mean ages ofthe twogroups (p=0.162).Thus,thesamplewasconsideredtobevalidated.
Inreassessingthese35patientsusingtheUCLAcriteria,18 we obtained a mean score of 31.31 (range: 17–35) (Fig. 1; Table1).Wefoundthat40%oftheresultswereexcellent,51% good,3%fairand6%poor.WorseningoftheUCLAresult18was onlyobservedin9%ofthecases.Themeanrangeofmotion was132◦ forelevation(range:100–160◦),50◦ forlateral rota-tion (range: 30–70◦)and T10 formedialrotation (range: T7 toL2). Rerupturewasobservedinthreecases:twopatients whomaintainedgoodorexcellentresultsandonewho pre-sentedworsening(Table1).Thepatientswhohadundergone acromioplastypresentedbetterresultsaccordingtotheUCLA criteria18thanthoseofpatientswhohadnotundergonethis procedure(p=0.02).
Discussion
Intheliterature,wefoundsomestudiesonarthroscopicrepair ofextensiverotatorcuffinjurieswithshort-termresultsthat wereencouraging.JonesandSavoie16 retrospectively evalu-ated50casesoflargeandextensiveinjuriesthatwererepaired usinganarthroscopictechniquewithameanlengthof follow-upof32months.Theyobtainedasatisfactionrateof98%and meanscoreof32.7usingtheUCLAmethod,and88%oftheir patientswereclassifiedashavinggoodorexcellentresults.16
Bennett15 evaluated 37 caseswithamean follow-upof3.2 years,inwhich78%oftheinjurieswerecompletelyrepaired, andobtainedameanASESscoreof77forinjuriesof postero-superiorpatternand85forinjuriesofanterosuperiorpattern. In2009,wepublishedaseriesof61casesofextensiverotator cuffinjurieswithameanfollow-upof36monthsandfound that89%oftheresultsweregoodorexcellent,accordingtothe UCLAmethod.14,18
Morerecently,Denardetal.5conductedalong-term evalu-ationon126caseswithaminimumfollow-upof5yearsand meanof8.2yearsandfoundthat78%oftheresultsweregood orexcellent,accordingtotheUCLAmethod.Wefoundthat 91% ofthe resultsthathad been considered tobegood or excellentaccordingtotheUCLAmethodweremaintained.18 Ourresultsalsoshowedfavourableoutcomesfromusingthe arthroscopictechnique,andshowedthatthegoodand excel-lentresultsweremaintained,evenforlongtimesafterthefirst evaluation.
In relation tomobility, no significant diminution of the rangeofmotionwasobserved,eitherforelevationorforlateral and medialrotation.Nodifferenceregardingthefunctional resultswasobservedincomparing traumaticand nontrau-matic causes ofthe injuries. Thenumber ofanchors used did notinfluence the results and neitherdid the different approachesusedforthelongheadofthebiceps.
Thepatientswhounderwentacromioplastyachieved bet-terresultsaccordingtotheUCLAmethod,18inrelationtothose whodidnotundergothisprocedure(p=0.029).Thiswasvery likelybecause thelattercaseswere ofgreaterseverity and the surgeondecidednottoperformacromioplastybecause ofthe high probabilityofrerupture.20 Wefound thatthere wasworseningofthefunctionalresultsinonlythreepatients, andtheexplanationsforthismayhavebeenthefactthatone ofthemwasalong-termsmoker(case2),anotherpracticed sportsfrequently(case32)andthethirdsufferedworsening ofpreexistingcomorbidities(case20).Wefoundthatinsome studies,socialhabitssuchassmokingandoccupational activ-itieshadanegativeinfluenceontendonhealing.21
Thenumberofcasesofrerupturediagnosedinthepresent study wasvery small, which was discordant with findings intheliterature.Thiswasprobablybecausewedidnot rou-tinelyperformmagneticresonanceimagingontheshoulders of asymptomatic patients.22 However, like Gerber et al.,23 Jost etal.,24and Melladoetal.,25 webelievethatrerupture ofrepairedtendonsisnotnecessarilyassociatedwithpoor clinical results.Thiswasseeninourcase1,whichdespite reruptureobservedonshouldermagneticresonanceimaging, continuedtopresentanexcellentfunctionalresult(Table1).
Onelimitingfactor ofthepresent studywasourlossof 33%ofthesample,whichmayhaveledtosomeformofbias intheresults.However,wetooktheprecautionofcomparing thesamples(studiedversuslost)throughstatisticaltestsand observedthattherewasnoheterogeneitybetweenthesetwo groups.
Conclusion
Amongthegroupof35patientswithgoodorexcellentresults fromthearthroscopicrepair,mostofthem(91%)maintained the same leveloffunction and satisfactionover the entire period,withameanof11.4years.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. WhiteJJ,TitchenerAG,FakisA,TambeAA,HubbardRB,Clark DI.Anepidemiologicalstudyofrotatorcuffpathologyusing TheHealthImprovementNetworkdatabase.BoneJointJ. 2014;96-B(3):350–3.
2. FukudaH.Partialthicknessrotatorcufftears:amodernview onCodman’sclassic.JShoulderElbowSurg.2000;9(2):163–8. 3. SorensenAK,BakK,KrarupAL,ThuneCH,NygaardM,
JorgensenU,etal.Acuterotatorcufftear:dowemissthe earlydiagnosis?Aprospectivestudyshowingahigh incidenceofrotatorcufftearsaftershouldertrauma.J ShoulderElbowSurg.2007;16(2):174–80.
4. DeOrioJK,CofieldRH.Resultsofasecondattemptatsurgical repairofafailedinitialrotatorcuffrepair.JBoneJointSurg Am.1984;66(4):563–77.
5. DenardPJ,JiwaniAZ,LädermannA,BurkhartSS.Long-term outcomeofarthroscopicmassiverotatorcuffrepair:the importanceofdouble-rowfixation.Arthroscopy. 2012;28(7):909–15.
6. GerberC,KrushellRJ.Isolatedruptureofthetendonofthe subscapularismuscle:clinicalfeaturesin16cases.JBone JointSurgBr.1991;73(3):389–94.
7. KoesterMC,DunnWR,KuhnJE,SpindlerKP.Theefficacyof subacromialcorticosteroidinjectioninthetreatmentof rotatorcuffdisease:asystematicreview.JAmAcadOrthop Surg.2007;15(1):3–11.
8. NhoSJ,YadavH,ShindleMK,MacgillivrayJD.Rotatorcuff degeneration:etiologyandpathogenesis.AmJSportsMed. 2008;36(5):987–93.
9. GartsmanGM,KhanM,HammermanSM.Arthroscopicrepair offull-thicknesstearsoftherotatorcuff.JBoneJointSurg Am.1998;80(6):832–40.
10.JostB,PfirrmannCW,GerberC,SwitzerlandZ.Clinical outcomeafterstructuralfailureofrotatorcuffrepairs.JBone JointSurgAm.2000;82(3):304–14.
11.TauroJC.Arthroscopicrotatorcuffrepair:analysisof techniqueandresultsat2-and3-yearfollow-up. Arthroscopy.1998;14(1):45–51.
12.ChecchiaSL,DoneuxPS,MiyazakiAN,FregonezeM,SilvaAL, IshiM,etal.Avaliac¸ãodosresultadosobtidosnareparac¸ão artroscópicadaslesõesdomanguitorotador.RevBrasOrtop. 2005;40(5):229–38.
13.GalatzLM,BallCM,TeefeySA,MiddletonWD,YamaguchiK. Theoutcomeandrepairintegrityofcompletely
arthroscopicallyrepairedlargeandmassiverotatorcufftears. JBoneJointSurgAm.2004;86(2):219–24.
14.MiyazakiAN,FregonezeM,DoneuxPS,SilvaLA,PintoECM, OrtizRT,etal.Lesõesextensasdomanguitorotador: avaliac¸ãodosresultadosdoreparoartrocópico.RevBras Ortop.2009;44(2):148–52.
15.BennettWF.Arthroscopicrepairofmassiverotatorcufftears: aprospectivecohortwith2-and4-yearfollow-up.
Arthroscopy.2003;19(4):380–90.
16.JonesCK,SavoieFH.Arthroscopicrepairoflargeandmassive rotatorcufftears.Arthroscopy.2003;19(6):564–71.
17.PaxtonES,TeefeySA,DahiyaN,KeenerJD,YamaguchiK, GalatzLM.Clinicalandradiographicoutcomesoffailed repairsoflargeormassiverotatorcufftears:minimum ten-yearfollow-up.JBoneJointSurgAm.2013;95(7): 627–32.
18.EllmanH,HankerG,BayerM.Repairoftherotatorcuff.End resultstudyoffactorsinfluencingreconstruction.JBoneJoint SurgAm.1986;68(8):1136–44.
19.HawkinsRJ,BokosDJ.Clinicalevaluationofshoulder problems.In:RockwoodCAJr,MatsenFA3rd,editors.The shoulder.2nded.Philadelphia:Saunders;1998.
p.175–80.
20.FlatowEL,WeinsteinDM,DuraldeXA,CompitoCA,Pollock RG,BiglianiLU.Coracoacromialligamentpreservationin rotatorcuffsurgery.JShoulderElbowSurg.1994;Suppl.3:S73. 21.CarboneS,GuminaS,ArceriV,CampagnaV,FagnaniC,
PostacchiniF.Theimpactofpreoperativesmokinghabiton rotatorcufftear:cigarettesmokinginfluencesrotatorcuff tearsizes.JShoulderElbowSurg.2012;21(1):56–60.
22.BoileauP,BaqueF,ValerioL,AhrensP,ChuinardC,TrojaniC. Isolatedarthroscopicbicepstenotomyortenodesisimproves symptomsinpatientswithmassiveirreparablerotatorcuff tears.JBoneJointSurgAm.2007;89(4):747–57.
23.GerberC,FuchsB,HodierJ.Theresultsofrepairofmassive tearsoftherotatorcuff.JBoneJointSurgAm.
2000;82(4):505–15.
24.JostB,ZumsteinM,PfirrmannCW,GerberC.Long-term outcomeafterstructuralfailureofrotatorcuffrepairs.JBone JointSurgAm.2006;88(3):472–9.