rev bras ortop.2016;51(1):36–39
w w w . r b o . o r g . b r
Original
Article
Evaluation
of
surgical
treatment
of
carpal
tunnel
syndrome
using
local
anesthesia
夽
Marco
Felipe
Francisco
Honorato
Barros
∗,
Aurimar
da
Rocha
Luz
Júnior,
Bruno
Roncaglio,
Célio
Pinheiro
Queiróz
Júnior,
Marcelo
Fernandes
Tribst
HospitalRegionaldePresidentePrudente,PresidentePrudente,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20November2014 Accepted28January2015
Availableonline21December2015
Keywords:
Carpaltunnelsyndrome Localanesthesia Epinephrine
a
b
s
t
r
a
c
t
Objective:Toevaluatetheresultsandcomplicationsfromsurgicaltreatmentofcarpaltunnel syndromebymeansofanopenroute,usingalocalanesthesiatechniquecomprisinguseof asolutionoflidocaine,epinephrineandsodiumbicarbonate.
Materialandmethods: Thiswasacohortstudyconductedthroughevaluatingthemedical filesof16patientswhounderwentopensurgerytotreatcarpaltunnelsyndrome,withuse oflocalanesthesiaconsistingof20mLof1%lidocaine,adrenalineat1:100,000and2mL ofsodiumbicarbonate.TheDASHscoresbeforetheoperationandsixmonthsafterthe operationwereevaluated.Comparisonsweremaderegardingtheintensityofpainatthe timeofapplyingtheanestheticandduringthesurgicalprocedure,andinrelationtoother typesofprocedure.
Results:The DASHscore improved from 65.17to 16.53 six monthsafter the operation (p<0.01).Inrelationtotheanesthesia,75%ofthepatientsreportedthatthistechnique wasbetterthanorthesameasvenouspunctureand81%reportedthatitwasbetterthana dentalprocedure.Intraoperativepainoccurredintwocases.Therewerenooccurrencesof ischemia.
Conclusion:Useoflocalanesthesiaforsurgicallytreatingcarpaltunnelsyndromeiseffective forperformingtheprocedureandforthefinalresult.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Avaliac¸ão
do
tratamento
cirúrgico
da
síndrome
do
túnel
do
carpo
com
anestesia
local
Palavras-chave:
Síndromedotúneldocarpo Anestesialocal
Epinefrina
r
e
s
u
m
o
Objetivo:Avaliarosresultadoseascomplicac¸õesdotratamentocirúrgicodasíndromedo túneldocarpo(STC)porviaaberta,comoempregodatécnicaanestésicalocalcomuma soluc¸ãocompostaporlidocaína,epinefrinaebicarbonatodesódio.
夽
WorkdevelopedbytheDepartmentofOrthopedicsandTraumatology,UniversidadedoOestePaulista(UNOESTE),andOrthopedics andTraumatologyService,HospitalRegionaldePresidentePrudente,PresidentePrudente,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.F.F.H.Barros). http://dx.doi.org/10.1016/j.rboe.2015.12.001
r e v b r a s o r t o p . 2016;51(1):36–39
37
Materiaisemétodos:Estudodecoorte,pormeiodaavaliac¸ãodosprontuáriosde16pacientes submetidosacirurgiaabertaparaSTCcomempregodeanestesialocalcom20mLde lido-caína1%,adrenalina1:100.000e2mLdebicarbonatodesódio.Avaliac¸ãodoescoreDASH nopréepós-operatóriodeseismesesecomparac¸ãodaintensidadedadorduranteoato anestésico,duranteacirurgiaeemrelac¸ãoaoutrostiposdeprocedimentos.
Resultados: OescoreDASHmelhoroude65,17para16,53nopós-operatóriodeseismeses (p<0,01).Emrelac¸ãoàanestesia,75%dospacientesrelataramqueessatécnicaémelhor ouigualaumapunc¸ãovenosae81%relataramqueémelhordoqueumprocedimento dentário.Emdoiscasosocorreudornointraoperatório.Nãoocorreramisquemias.
Conclusão: Oempregodeanestesialocalparaotratamentocirúrgicodasíndromedotúnel docarpoéeficazparaoprocedimentoeparaoresultadofinal.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Carpal tunnelsyndrome (CTS)isone ofthe diseases most frequentlytreatedbyorthopedistsandhandsurgery special-ists and it is considered to be the commonest peripheral compressiveneuropathy.1,2Thisconditionisresponsiblefor substantialannualcoststosociety,bothintermsoflossof thesepatients’productivityandinrelationtothedirectcosts oftreatment.Inmanycases,conservativetreatmentis inef-fectiveandthereisaneedforsurgicaltreatment.3
Traditionalmedicaleducation contraindicatesthe useof adrenalineinanestheticblockadesoftheextremitiesofthe limbs,and this concept continues tobe taughtin medical schoolsandintraditionaltextbooksonsurgery.Somestudies havereportedthatthereisalackofconsensusamonghand surgeonsregardingwhetherornottouseadrenalineatthe extremities.4–6
Expenditureonmedicaltreatmentsisincreasing.Inthis light, thereis immenseconcern with funding forthis and alternative solutions are being sought.7–9 We believe that treatmentsthatareproposedtopatientsneedtobethemost effectiveonesintermsofthefunctionalandestheticresults, whilealsokeepingthecostsaslowaspossible.Forthisreason, weconsideredthatthetechniqueusedbyLalondeforsurgical treatmentofCTSwasofgreatinterest.10–12
The objective of this study was to assess the results andcomplicationsfromsurgicaltreatmentofCTSusingan open route under local anesthetic composed of lidocaine, epinephrineandbicarbonate,asdescribedbyLalondeetal.10
Materials
and
methods
Forthisstudy,16patientswithCTSwereselected.Theyhad beendiagnosedclinicallythroughpositiveDurkanandPhalen tests, and through electromyography. All ofthese patients agreedtoparticipateinthisstudyandsignedaconsent state-mentforthis.Theywereanesthetizedandunderwentsurgery usingthetechniquedescribedbyLalonde,whichisknownas “hole-in-onecarpaltunnelsurgery”.Thedayhospitalsystem wasused,whichthepatientsweredischargedjustafterthe surgicalprocedure and no preoperativeexaminationswere requested.
The technique has the aim of achieving longitudinal releaseofthetransverseligamentofthecarpusbymeansofan openroute,withanaccessofaround3cmabovetheregionof thecarpaltunnel(flexorzone4),underlocalanesthesiaalone, withoutsedationoranyconcomitantmedication,and with-out atourniquet.Theideaisthatthepatientwillonlyfeel thefirstprickoftheneedleandshouldnotfeelanyfurther pain ordiscomfortafterthis moment.Thepatient receives aninfusionof22mLofananesthetic solutionbymeansof a20mLsyringe(thesesyringesactuallyhold22mL)witha 30mm×0.7mmneedle.Initially,around3–4mLisinfiltrated intothesubdermalregionofthedistalportionoftheforearm, betweenthepathsofthemedianandulnarnerves.Then,8mL isinfiltratedintothesubfasciallayerofthedistalportionof theforearmandtheremaining10mLintothesubdermallayer, anteriorly to the transverse ligament ofthe carpus.10 The approximatetimetakenforinfiltrationofallofthe medica-tionisaroundfiveminutesandcareisrequiredinordertokeep theneedlewithinamarginof5mmfromtheregionthathas alreadybeenanesthetized.Duringtheinfiltrationofthe solu-tion,tissuetumefactionandskinpallorareobserved,andthis demonstratespenetrationofthemedicationandtissue vaso-constriction.Thesolutionthatisinfiltratediscomposedof 20mLof1%lidocainewithepinephrineat1:100,000and2mL of8.4%sodiumbicarbonate.Becauseoftheuseofepinephrine, thereisnoneedtoapplyatourniquet.12
ThepatientswereevaluatedusingtheDASHscore imme-diatelybeforetheoperationandsixmonthsafterwards.The resultsfromthese16patientswereexpressedasthemeanand standard deviation. The statistical analysis was performed usingStudent’sttest.Thisstudywasproperlyapprovedbythe ResearchEthicsCommitteeoftheUniversityofOestePaulista (UNOESTE)andalltheparticipantssignedafreeandinformed consentstatement.
Results
38
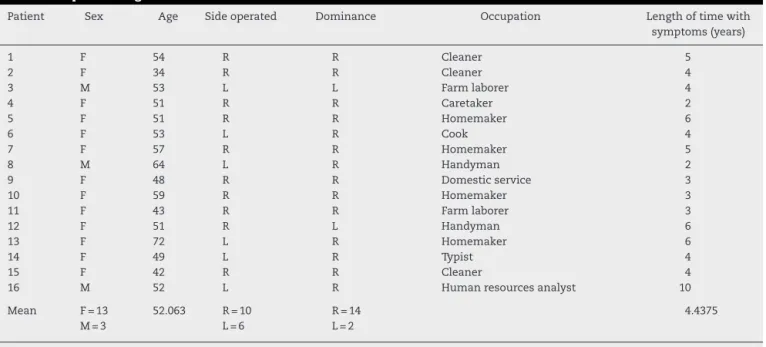
r e v b r a s o r t o p . 2016;51(1):36–39Table1–Epidemiologicaldata.
Patient Sex Age Sideoperated Dominance Occupation Lengthoftimewith
symptoms(years)
1 F 54 R R Cleaner 5
2 F 34 R R Cleaner 4
3 M 53 L L Farmlaborer 4
4 F 51 R R Caretaker 2
5 F 51 R R Homemaker 6
6 F 53 L R Cook 4
7 F 57 R R Homemaker 5
8 M 64 L R Handyman 2
9 F 48 R R Domesticservice 3
10 F 59 R R Homemaker 3
11 F 43 R R Farmlaborer 3
12 F 51 R L Handyman 6
13 F 72 L R Homemaker 6
14 F 49 L R Typist 4
15 F 42 R R Cleaner 4
16 M 52 L R Humanresourcesanalyst 10
Mean F=13
M=3
52.063 R=10 L=6
R=14 L=2
4.4375
F,female;M,male;R,right;L,left.
ownhomesordoingdomesticservicesorcleaningservices. Thelengthoftimewithsymptomsrangedfrom twototen years,withameanof4.43(Tables1and2).
Regardingthenumberoftimesthatpatientsfeltpain dur-ingtheanesthesia,12(75%)reportedfeelingonlyoneepisode, whilefour(25%)reportedtwoepisodes,thusgivingameanof 1.25times.Regardingtheintensityofthepainduringthe anes-thesia,12(75%)reportedintensity1,two(12.5%)intensity2 andtwo(12.5%)intensity8,withameanintensityof2.In com-parisonwiththeanesthesiausedforadentalprocedure,13 (81%)reportedthatthistechniquewasbetterandthree(19%) thatitwasworse.Incomparisonwithvenouspuncture,eight (50%)reportedthatthistechniquewasbetter,four(25%)that itwasworseandfour(25%)thattheywerethesame.In com-parisonwithanyothertypeofanesthesia,12(75%)reported thatthistechniquewasbetter,one(6%)thatitwasworseand three(19%)wereunabletorespond(Table3).Innocasewas thereanyischemiaornecrosis.
In twocases, there were reports ofintraoperative pain, whichwerebothsuddenandwerepromptlyresolved.Inone patient,thereweresymptomsofshockintheregionofthe ulnarnervebecausethesofttissueshadbeenpushedaside verybrusquely,andinanotherpatientthereweresymptoms intheregionofthemediannerveduetoinadvertentpinching ofthemediannerveusingtweezers.
Table2–Clinicalcharacteristicsofthepatients.
Clinicalcharacteristics Patients(n=16)
Durationofsymptoms,inyears(mean±SD) 4±2
Sideaffected,n(%)
Right 10(63)
Left 6(37)
Dominantlimb,n(%)
Right 14(88)
Left 2(12)
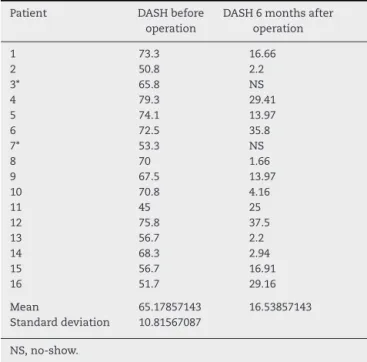
TheDASHquestionnairewasappliedtothepatientsbefore the operation and six months afterwards. Among the 16 patients,twodidnotcomebackforthepostoperative evalua-tion(nos.3and7).ThepreoperativeDASHscorerangedfrom 45to79.3,withameanof65.17.Inthepostoperative evalua-tion,weexcludedthetwopatientswhoweremissing.Among thosewhoansweredthequestionnairesixmonthsafterthe operation,thescoresrangedfrom1.66to37.5,withameanof 16.53(Table4).
Toascertaintheefficacyofthesurgicaltreatment,weused thepairedStudent’sttest,fromwhichweobtainedthevalue of6.43.Thisrejectedthenullhypothesiswithaconfidence intervalof99%,withp<0.01.
Discussion
Theanestheticandsurgicalmethodusedinthisstudywas based on the technique already used by Lalonde et al.,12 inwhichalocalanestheticsolutioncomposedoflidocaine,
Table3–Characteristicsoftheanesthesia.
Characteristicsoftheanesthesia Patients(n=16)
Numberofpainepisodes(mean±SD) 1.25±0.4
Intensityofpain(mean±SD) 2±2.3
Dentalprocedure,n(%)
Better 13(81)
Worse 3(19)
Venouspuncture,n(%)
Same 4(25)
Better 8(50)
Worse 4(25)
Otheranesthesia,n(%)
Donotknow 3(19)
Better 12(75)
r e v b r a s o r t o p . 2016;51(1):36–39
39
Table4–ResultsfromDASHscore.
Patient DASHbefore
operation
DASH6monthsafter operation
1 73.3 16.66
2 50.8 2.2
3* 65.8 NS
4 79.3 29.41
5 74.1 13.97
6 72.5 35.8
7* 53.3 NS
8 70 1.66
9 67.5 13.97
10 70.8 4.16
11 45 25
12 75.8 37.5
13 56.7 2.2
14 68.3 2.94
15 56.7 16.91
16 51.7 29.16
Mean 65.17857143 16.53857143
Standarddeviation 10.81567087
NS,no-show.
epinephrineandbicarbonatewasused,thusdoingawaywith theneedforatourniquetorotheranestheticmethods.The aimwastoascertaintheresultsandrisksfrom usinglocal anesthetic that included epinephrine, inanesthesia ofthe extremitiesofthe upperlimbs,giventhat theteachings of themedicalliteratureoftenmakereferencetothetheorythat vasoconstrictionoftheterminalarteriesmayinduceischemia andnecrosis.Ontheotherhand,theuseofthisdrughasthe advantageofincreasingandprolongingtheactionofthe anes-theticand providing atemporary hemostaticeffect.12 This techniquediffersfromthosetraditionallyusedinthatthereis noneedforatourniquetatanytimeduringthesurgery,not evenforabriefperiod.13,14
Tworeviewshavebeenconducted:onepublishedin200115 andthe otherin2007.16 Thesesearchesforcasesinwhich necrosisandischemiaofthefingersoccurredsubsequentto usinglocalanesthesia withorwithout adrenaline,covering theperiodbetween1880and2000.Amongthe48casesfound, 27occurred without useofadrenalineand 21withits use. Amongthelatter,procainewasusedin18cases,cocainein twocasesandanunknownanestheticinonecase.Nota sin-glecaseoffingerischemiaaftercombineduseoflidocaineand epinephrinehasbeenreportedintheliterature.15,16
In Canada,more than 90% of operations to release the carpus are now performed under local anesthesia without sedation.17Goodresultscanbeobtained,providedthatthe anesthetic and surgical techniques are used correctly. The localanestheticintheskinisgiventimetoactbeforeanynew skinpunctureismadeusinganeedle,andaslittletissueas possibleispushedaway inareasthathave notbeen anes-thetized.Inourseries, therewere reportsofintraoperative painintwopatients:oneduetobrusquelypushingthetissue awayandtheotherduetopinchingofthemediannerve,i.e. throughfailuresoftheintraoperativetechnique.Thewaiting timenowusedbetweenapplicationofanestheticandstarting thesurgicalprocedureisnowatleast26min,giventhatthis
isthetimeduringwhichadrenalinehasitsgreatestefficacy andgivesrisetoleastlocalbleeding.18
Conclusions
Surgicaltreatmentofcarpaltunnelsyndromeusingthelocal anesthetic procedure provided satisfactory clinical results. Thereisaneedforachangeinparadigmforsurgeons,given thatmostofthemareaccustomedtoconductingthis proce-durewiththeentirelimbororganismanesthetized.Achange inparadigm regardinguse ofadrenaline attheextremities isalsoneeded,giventhatmythsregardingitsusehavebeen oustedinthecurrentliterature.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MallickA,ClarkeM,KershawJC.Comparingtheoutcomeofa carpaltunneldecompressionat2weeksand6months.JHand Surg.2007;32(8):1154–8.
2.ChammasM,BorettoJ,BurmanncLM,RamosRM,NetoFS,Silva JB.Síndromedotúneldocarpo–ParteI(anatomia,fisiologia, etiologiaediagnóstico).RevBrasOrtop.2014;49(5):429–36.
3.BickelKD.Carpaltunnelsyndrome.JHandSurgAm. 2010;35(1):147–52.
4.PeimerCA.Surgeryofthehand.In:SchwartzSI,editor.Principles ofsurgery.7thed.NewYork:McGraw-HillHealthProfessions Division;1999.p.2084.
5.CambellWC,CanaleST.CampbellCirugiaOrtopédica.10thed. SãoPaulo:Manole;2006.
6.GreenDP,PedersonMD,HotchkissRN,WolfSW.Green’soperative handsurgery.5thed.Philadelphia:ElsevierChurchillLivingstone; 2005.p.25–52.
7.GoldMR,SiegelJE,RussellLB,WeinsteinMC.Cost-effectivenessin healthandmedicine.NewYork:OxfordUniversityPress;1996.p. 54–80.
8.PushmanA,ChungKC.FutureoftheUShealthcaresystemandits effectsonthepracticeofhandsurgery.Hand(NY).
2009;4(2):99–107.
9.ChungKC,WaltersMR,GreenfieldML,ChernewME.Endoscopic versusopencarpaltunnelrelease:acost-effectivenessanalysis. PlastReconstrSurg.1998;102(4):1089–99.
10.LalondeDH.Hole-in-onelocalanesthesiaforwide-awakecarpal tunnelsurgery.PlastReconstrSurg.2010;126(5):1642–4.
11.KangHJ,KohIH,LeeTJ,ChoiYR.Endoscopicversusopencarpal tunnelrelease:arandomizedtrial.ClinOrthopRelatRes. 2013;471(5):1548–54.
12.LalondeDH,BellM,BenoitP,SparkesG,DenklerK,ChangP.A multicenterprospectivestudyof3,110consecutivecasesof electiveepinephrineuseinthefingersandhand:theDalhousie projectclinicalphase.JHandSurgAm.2005;30(5):1061–7.
13.ChammasM,BorettoJ,BurmanncLM,RamosRM,NetoFS,Silva JB.Síndromedotúneldocarpo–ParteII(tratamento).RevBras Ortop.2014;49(5):437–45.
14.BarbieriCH,PinheiroMWA,MazerN.Tratamentocirúrgicoda síndromedotúneldocarposobanestesialocal.RevBrasOrtop. 1991;26(10):361–4.
15.DenklerKA.Comprehensivereviewofepinephrineinthefinger: todoornottodo.PlastReconstrSurg.2001;108(1):114–24.
16.ThomsonCJ,LalondeDH,DenklerKA,FeichtAJ.Acriticallookat theevidenceforandagainstelectiveepinephrineuseinthe finger.PlastReconstrSurg.2007;119(1):260–6.
17.DonaldH,LalondeJF.Discussion:donotuseepinephrineindigital blocks:mythortruth?PartII.Aretrospectivereviewof1111cases. PlastReconstrSurg.2010;126(6):2035–6.