J Appl Oral Sci. 524
ABSTRACT
www.scielo.br/jaos
http://dx.doi.org/10.1590/1678-775720160178
Prevalence, severit y, and risk indicat ors of gingival
LQÀDPPDWLRQLQDPXOWLFHQWHUVWXG\RQ6RXWK
Am er ican adult s: a cr oss sect ional st udy
Paola CARVAJAL1, Mariel GÓMEZ2, Sabrina GOMES3, Ricardo COSTA3, Andres TOLEDO2, Fernando SOLANES1,
Hugo ROMANELLI2, Rui OPPERMANN3, Cassiano RÖSING3, Jorge GAMONAL1
1- Universidade de Chile, Facultad de Odontología, Departamento de Odontología Conservadora, Laboratorio de Biología Periodontal, Santiago, Chile. 2- Universidad Maimónides, Facultad de Odontología, Buenos Aires, Argentina.
3- Universidade Federal do Rio Grande do Sul, Faculdade de Odontologia, Departamento de Odontologia Conservadora, Porto Alegre, Brasil.
Corresponding address: Jorge Gamonal. Laboratorio de Biología Periodontal - Departamento de Odontología Conservadora - Facultad de Odontología
- Universidad de Chile - Sergio Livingstone Pohlhammer 943 - 83800 - Independencia - Santiago - Chile - Phone: +56 229781833 - Fax: +56 229781815 - e-mail: [email protected]
6XEPLWWHG$SULO0RGL¿FDWLRQ-XQH$FFHSWHG-XQH
O
bj ect ives: The aim of t his st udy is t o invest igat e t he prevalence and severit y of gingivalLQÀDPPDWLRQDQGDVVRFLDWHGULVNLQGLFDWRUVLQ6RXWK$PHULFDQDGXOWV0DWHULDODQG
Met hods: Mult i- st age sam ples t ot aling 1,650 adult s fr om Por t o Alegr e ( Brazil) , Tucum án ( Ar gent ina) , and Sant iago ( Chile) w er e assessed. The sam pling pr ocedur e consist ed of a 4- st age pr ocess. Exam inat ions w er e per for m ed in m obile dent al unit s by calibrat ed exam iner s. A m ult ivar iable logist ic r egr ession m odel was ut ilized for associat ing var iables
DVLQGLFDWRUVRIJLQJLYDOLQÀDPPDWLRQ*,*LQJLYDO,QGH[6WDWLVWLFDOVLJQL¿FDQFH
was set at 0.05. Result s: A t ot al of 96.5% of t he adult s have GI . Regar ding t he sever it y of GI , 22.5% of par t icipant s exam ined have m ild GI , 74.0% have m oderat e GI , and 3.6% have sever e GI . The m ult ivar iat e analy ses ident ify t he m ain r isk indicat or s for GI as
DGXOWVZLWKKLJKHUPHDQRI&DOFXOXV,QGH[25 ZLWKD9LVLEOH3ODTXH,QGH[ 25 OLYLQJLQ6DQWLDJR25 KDYLQJ\HDUVRIVFKRROLQJ25
and fem ales ( OR= 1.93) . Conclusions: This st udy show s a high pr evalence and sever it y of
JLQJLYDOLQÀDPPDWLRQEHLQJWKH¿UVWRQHSHUIRUPHGLQDGXOWSRSXODWLRQVLQWKUHHFLWLHVRI
Sout h Am er ica.
Ke y w or ds: Gingival diseases. Per iodont al index. Sout h Am er ica.
I N TROD UCTI ON
*LQJLYDOLQÀDPPDWLRQ*,LVDFRPPRQFOLQLFDO f eat u r e d et ect ed in ch ild r en an d ad u lt s1. I t is
charact er ized by sw elling, r edness, and bleeding DWWKHJXPVDQGLWLVGHVFULEHGDVDQLQÀDPPDWRU\ UHDFWLRQXSRQWKHSURLQÀDPPDWRU\F\WRNLQHVWKDW m odulat e t he balance bet w een hum oral and cell-associat ed im m une responses28. This clinical feat ure
is charact er ist ic of bot h gingivit is and per iodont it is. GI is considered t o be one m aj or class of periodont al condit ions, and is r ecognized t o r esult fr om t he incr ease in supragingival plaque and t he ensuing LQWHUDFWLRQVEHWZHHQWKHPLFURELRWDRIELR¿OPDQG
host r esponse26. Consequent ly, t he pr event ion of
plaque accum ulat ion and ear ly t r eat m ent of GI
r educe t he r isks associat ed w it h t he developm ent of t he m ore dest ruct ive periodont al disease5, w hich
has also been associat ed wit h syst em ic condit ions8.
Under st anding t he epidem iologic pat t er n of GI is essent ial for planning appr opr iat e public- healt h ser v ices. I t has been clear ly dem onst rat ed t hat plaque- induced GI is pr evalent at all ages of t he dent at e populat ion2,29. I n r ecent decades, cr
oss-sect ional and longit udinal epidem iological st udies on periodont it is in adult s were perform ed in Chile12 and
Brazil14. Mor eover, analyt ical appr oaches designed
t o ident ify associat ed fact or s t hat could be r isk LQGLFDWRUVIRUJLQJLYDOLQÀDPPDWLRQDUHQRQH[LVWHQW Our m ain obj ect ive in t his m ult i- cent er, populat ion-based, cr oss- sect ional and epidem iological st udy is t o in v est ig at e t h e p r ev alen ce, sev er it y, an d
J Appl Oral Sci. 525 r i s k i n d i c a t o r s f o r g i n g i v a l i n f l a m m a t i o n i n r epr esent at ive sam ples of t he adult populat ions of Por t o Alegr e ( Brazil) , Tucum án ( Ar gent ina) , and Sant iago ( Chile) .
M ATERI AL AN D M ETH OD S
St u dy de sign , sa m plin g, a n d sa m ple siz e s Th e p r esen t cr oss- sect ion al, r ep r esen t at iv e st u d y u t ilized st r at if ied , m u lt ist ag e p r ob ab ilit y sam ples of t he civilian, noninst it ut ionalized adult populat ions in t hr ee Sout h Am er ican cit ies. Dat a w er e collect ed bet w een Januar y and July of 2014.
Ou r sam p lin g ap p r oach con sid er ed v ar iou s ag e su b g r ou p s ( 1 8 - 1 9 ; 2 0 - 2 9 ; 3 0 - 3 9 ; 4 0 - 4 9 ; DQG \HDUV RI DJH &RQVLGHULQJ SUHYLRXVO\ published infor m at ion t hat est im at ed a pr evalence
of gingiv it is of 93.9%21 ( average Gingival I ndex
ZLWKDSUHFLVLRQUDWHRIDQGDHUURU w e det er m ined t hat a sam ple size of 550 adult s w ould be appr opr iat e for each of t he t hr ee cit ies in t he st udy. To do so, t he for m ula t o est im at e t he
pr evalence of a populat ion ( n= Z2
1 -D/ 2 P( 1 - P) / e 2)
was used.
The st udy par t icipant s w er e select ed using a m u lt i- st aged pr obabilit y sam plin g pr ocess. Age gr oups w er e for m ed accor ding t o a pr opor t ional appr oach t o t he base populat ion r egist r ies in t he t ot al of u r b an ad m in ist r at iv e r eg ion s in Por t o Alegr e, Tucum án, and Sant iago, accor ding t o t he last census in each cit y, and considering differences in gender and age.
The sam pling pr ocess consist ed of four st ages: Cit y ( pr im ar y sam pling unit s - 1st st age) ; Tract
ce n su s ( 2n d st a g e ) ; Bl o ck s ( 3r d st a g e ) ; a n d
I ndividuals w it hin t he age gr oup ( 4t h st age) . The
ci t i es w er e ch osen accor d i n g t o l og i st i cs an d int er est s in t he t hr ee count r ies. Using m aps of each cit y, pr im ar y census sect or s w er e random ly chosen. The num ber of sect or s in each cit y was det er m ined accor ding t o t he cit y size and census dist ribut ion. I f t he access t o a prim ary census sect or was not possible, t he next available census sect or was chosen. I n each census sect or, t he blocks w er e random ly chosen. On each block, households w er e consecut ively appr oached accor ding t o t he sect or st ar t ing point , unt il t he num ber of par t icipant s expect ed for each sect or was r eached. Places such as nur sing hom es and com m er cial est ablishm ent s w er e not included. When no pot ent ial par t icipant s w er e available for exam inat ion in a household, t he next household was visit ed.
Can didat es w h o h av e ex pr essed an in t er est in par t icipat ing in t he st udy w er e select ed based on t he follow ing cr it er ia: 18 year s of age or older, healt hy, and w it h at least four per m anent t eet h. Wer e excluded fr om t he st udy candidat es needing ant ibiot ic pr ophylaxis pr ior t o dent al exam inat ion,
w om en w h o w er e p r eg n an t or b r east f eed i n g , i n d i v i d u al s w i t h f i x ed o r t h o d o n t i c ap p l i an ces, or in d iv id u als w h o ch r on ically u sed n if ed ip in e, cy cl o sp o r i n e , p h e n y t o i n , o r a n y p r e scr i p t i o n m ed icin es t h at m ig h t in t er f er e w it h t h e st u d y out com e.
The prot ocol used for t his st udy is in accordance w it h t he Declarat ion of Helsinki and was r eview ed and appr oved by t he I nst it ut ional Review Boar ds of t he Univer sit y of Chile, Federal Univer sit y of Rio Grande do Sul, and Maim onides Universit y. All st udy par t icipant s w er e infor m ed about t he aim s of t he st udy and signed an infor m ed consent for m .
Clin ica l e v a lu a t ion a n d sociode m ogr a ph ic a n d be h a v ior a l da t a
A sociodem ographic and general healt h int erview w as conduct ed and a st r uct ur ed quest ionnair e, con sist in g of open an d closed qu est ion s abou t dem ographics, habit s, at t it udes, and k now ledge relat ed t o oral healt h, was designed and adm inist ered t o all par t icipant s. This quest ionnair e was t est ed at each of t he t hree st udy sit es and adapt ed according t o t he necessit ies of t he local populat ion. Finally, a com plet e dent al exam inat ion was per for m ed on all par t icipant s in t he st udy.
Pr ior t o t he init iat ion of t he st udy, t he pr incipal invest igat or s and exam iner s m et in Por t o Alegr e in or der t o st andar dize diagnost ic cr it er ia w it h t he reference exam iner ( CR) . I nt ra- and int er- exam iner NDSSD FRHI¿FLHQWV IRU WKH 9LVLEOH 3ODTXH ,QGH[ Calculus I ndex , and Gingival I ndex w er e abov e 0.7. I n addit ion, t he st r uct ur ed quest ionnair e was st andar dized for each of t he t hr ee st udy locat ions.
Each t eam consist ed of one clinical exam iner, t ot aling t hr ee dent al exam iner s ( RC, AT, FS) and each conduct ed exam s using a m anual per iodont al pr obe ( UNC- 1 5 ) and m obile dent al unit s. Good clinical pract ice st andards were used and warrant ed. Per iodont al clinical param et er s w er e evaluat ed in all t eet h, excluding t hir d m olar s. The param et er s evaluat ed were Visible Plaque I ndex ( VPI ) , Calculus I ndex ( CI ) , and Gingival I ndex ( G- I ndex) . Visual plaque assessm ent was det er m ined using absence ( 0) or pr esence ( 1) of dent al plaque accor ding t o $LQDPR %D\ 7KH /|H PRGL¿FDWLRQ RI WKH /|H Silness index was used t o evaluat e gingival healt h. Each t oot h w as div ided int o six sur faces, t hr ee facial and t hr ee lingual, as follow s: 1) m esio- facial; 2) m id- facial; 3) dist o- facial; 4) m esio- lingual; 5) m id- lingual; and 6) dist o- lingual. Thir d m olar s and t hose t eet h w it h cer vical r est orat ions or pr ost het ic cr ow ns w er e excluded fr om t he scor ing pr ocedur e. Absence ( 0) or pr esence ( 1) of calculus was scor ed in low er ant er ior t eet h ( CI ) . Each t oot h was divided int o t hree lingual surfaces, as follows: dist o- lingual, m edio- lingual, and m esio- lingual. At t he end of clinical exam inat ions, t hose par t icipant s w ho w er e
3UHYDOHQFHVHYHULW\DQGULVNLQGLFDWRUVRIJLQJLYDOLQÀDPPDWLRQLQDPXOWLFHQWHUVWXG\RQ6RXWK$PHULFDQDGXOWVDFURVVVHFWLRQDOVWXG\
J Appl Oral Sci. 526 diagnosed w it h per iodont al pat hologic condit ions w er e pr ovided a w r it t en r epor t of t heir condit ion and advised t o seek an oral healt h consult at ion.
'H¿QLWLRQRIYDULDEOHV
7KH SUHYDOHQFH RI JLQJLYDO LQÀDPPDWLRQ ZDV GH¿QHGDVWKHSHUFHQWDJHRIVWXG\SDUWLFLSDQWVZLWK D PHDQ *LQJLYDO ,QGH[ *,QGH[ *LQJLYDO %OHHGLQJ,QGH[*%,ZDVGH¿QHGDVWKHSHUFHQWDJH RI VLWHV ZLWK *,QGH[ :KHQ DSSURSULDWH est im at es w er e isolat ed for int er pr ox im al sit es. 6HYHULW\RIJLQJLYDOLQÀDPPDWLRQZDVGH¿QHGDV G- I ndex 0.5- 1.0 for m ild, 1.1- 2.0 for m oderat e, DQG!IRUVHYHUHJLQJLYDOLQÀDPPDWLRQ6WXG\ SDUWLFLSDQWVZHUHFODVVL¿HGE\WKHLUVPRNLQJKDELWV as eit her nonsm oker s or sm oker s. Sm oker s w er e IXUWKHU FODVVL¿HG DV OLJKW FLJDUHWWHVper day) , m oderat e ( 5- 10 per day) , and heavy ( over 10 per day) . The educat ional level of t he st udy part icipant s ZDV DOVR FDWHJRUL]HG DV RU ! \HDUV RI school. The G- I ndex, VPI , GBI , and CI indices ar e r epr esent ed in t he dat a as m ean values.
St a t ist ica l a n a ly se s
Con t in u ou s dat a ar e pr esen t ed as m ean s ± SDs, and cat egor ical var iables ar e pr esent ed as SHUFHQWDJHV7KHGDWDDUHVWUDWL¿HGDFFRUGLQJWR sociod em og r ap h ic, b eh av ior al, an d p er iod on t al values. Chi- squar e t est s w er e applied t o com par e dist r ibut ions of per iodont al var iables bet w een age gr oups and cent er s; t o assess differ ences in t he m eans and percent ages, Mann-Whit ney or Kruskall-Wallis t est s w er e applied, and st at ist ical analyses were perform ed using a st at ist ical soft ware package ( St at a/ I C 13.1) . A m ult i- variable logist ic regression m od el w as b u ilt t o assess t h e con t r ib u t ion of each var iable ( age, gender, sm ok ing, and social or cu lt u r al fact or s) . Th e occu r r en ce of gin gival LQÀDPPDWLRQZDVFRQVLGHUHGLI*,QGH[,Q addit ion, var iables w er e analyzed in t he m odel and DOORZHGLIWKHFRHI¿FLHQWZDVPRGL¿HGE\DWOHDVW 10% . VPI was dichot om ized at 30% . Odds rat ios ZHUH FDOFXODWHG ZLWK FRQ¿GHQFH LQWHUYDOV DQGVWDWLVWLFDOVLJQL¿FDQFHZDVGH¿QHGDVS
RESULTS
A t o t al o f 1 6 5 0 ad u l t s f r o m Po r t o Al eg r e, Tucum án, and Sant iago par t icipat ed in t his st udy. Fem ales r epr esen t 5 2 . 5 % of t h e ov er all st u dy par t icipant s, w hile one t hir d of t he par t icipant s ar e LQWKH\HDUVDJHJURXS
3UHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQ
Table 1 show s t hat t he overall pr evalence of JLQJLYDOLQÀDPPDWLRQPHDQ*,QGH[IRUWKH st udy populat ion is 95.6% . The Sant iago and Por t o $OHJUH SDUWLFLSDQWV SUHVHQW D VLJQL¿FDQWO\ KLJKHU SUHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQSDW 99.1% and 97.3% , r espect ively, as com par ed w it h part icipant s from Tucum án, at 90.4% . Only in Port o $OHJUHWKHSUHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQLQ CARVAJAL P, GÓMEZ M, GOMES S, COSTA R, TOLEDO A, SOLANES F, ROMANELLI H, OPPERMANN R, RÖSING C, GAMONAL J
2016;24(5):524-34 QUESTIONNAIRE
DATE:
GENERAL INFORMATION Number Questionnaire
Birth date
Age in Years
Gender 1 Female
2 Male
Place of residence SOCIOCULTURAL LEVEL 1. Currently you are:
1 Working
2 Unemployed
3 Voluntary work
4 Studying
5 Studying and working
6 Retired
2. What kind of education have you received? 1 Without education
2 Some elementary school 3 Elementary school
4 Some high school
5 High school
6 Professional degree
7 Some college
8 College degree
9 Graduate degree
GENERAL HEALTH
3. Have you been diagnosed with any of the following illnesses?
1 No
2 Yes Which?
1 Diabetes
2 Arterial hypertension
3 Obesity
4 Myocardial infarction
5 Stroke
6 Pneumonia
7 Asthma
8 Osteoporosis
9 Depression
10 Cancer
11 Other
4. Do you use any medication permanently?
1 No
2 Yes Which?
1 Anxiolytic
2 Antihypertensive
3 Anticoagulant
4 For cholesterol
5 For thyroid disorders
6 For cardiac disorders
7 Hormonal support
8 Cancer treatment
9 Diabetes treatment
10 Contraceptives
11 Other (specify)
SMOKING HABIT 5. Have you ever smoked?
1 Never smoked
2 Smoked but quit
3 Currently smoking
6. If you smoke, how many years have you been smoking? 7. If you smoke, how many cigarettes do you smoke a day on average?
J Appl Oral Sci. 527 WKH\HDUVDJHJURXSLVVLJQL¿FDQWO\KLJKHUWKDQ in t he 40- 49 and 20- 29 years age groups ( p< 0.05) . :KHQWKHWRWDOVDPSOHLVFRQVLGHUHGDVLJQL¿FDQW differ ence is obser ved bet w een t he pr evalence of JLQJLYDOLQÀDPPDWLRQLQWKHDQGWKH
\HDUVDJHJURXSVSIRU3RUWR Alegr e and Tucum án, but not for Sant iago.
Con sider in g t h e t ot al sam ple of t h e pr esen t st u d y, n o st at ist ically sig n if ican t d if f er en ce is obser ved bet w een gender s ( Table 2) . I n t he ent ir e
Age (years)
PORTO ALEGRE** TUCUMÁN SANTIAGO TOTAL**
Gingival
,QÀDPPDWLRQ
Gingival
,QÀDPPDWLRQ
Gingival
,QÀDPPDWLRQ
Gingival
,QÀDPPDWLRQ
Total
n (%) n (%) n (%) n (%) n (%)
18-19 24 100 29 93.5 24 100 77 97.5 79 4.8
20-29 98 94.2 125 85.0 126 99.2 349 92.3 378 22.9
30-39 115 96.6 115 91.3 101 98.1 331 95.1 348 21.1
40-49 102 95.3 86 94.5 102 100 290 96.7 300 18.2
196 100 142 91.6 192 99.0 530 97.3 545 33.0
Total 535 97.3* 497 90.4* 545 99.1* 1 577 95.6 1 650 100
SYDOXH)LVKHUVH[DFWWHVWWRDVVHVVGLIIHUHQFHVEHWZHHQSUHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQ7XFXPiQYHUVXV
P. Alegre and Santiago
SYDOXH)LVKHUVH[DFWWHVWWRDVVHVVGLIIHUHQFHVEHWZHHQSUHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQDQGDJH
Table 1-3UHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQPHDQ*,QGH[DFFRUGLQJWRDJHper city
Variables PREVALENCE OF GINGIVAL INFLAMMATION
BY CITY AND TOTAL
n PORTO
ALEGRE
TUCUMÁN SANTIAGO TOTAL p-value**
n n n n
Gender Female 867 52.6 275 98 274 92.6 286 98.3 835 96.3
Male 783 47.5 260 96.3 223 87.8 259 100 742 94.8 0.127
Education (years)
1 099 66.6 424 97.9 352 94.9* 293 99.3 1 069 97.3*
>12 551 33.4 111 94.9 145 81.0 252 98.8 508 92.2 0.000
Smoking No 1 180 71.5 384 96.7 368 89.5 368 98.9 1 120 94.2
Current (light) 171 10.4 17 100.0 57 96.6 94 98.9 168 98.3
Current (moderate) 76 4.6 24 96.0 17 94.4 33 100.0 74 97.4
Current (heavy) 223 13.5 110 99.1 55 88.7 50 100.0 215 96.4 0.194
Self-reported diabetes
No diabetes
1 528 92.6 489 97.0 493 90.3 473 99.0 1 455 95.2
Yes 122 7.4 46 100 4 100 72 100 122 100* 0.005
Self-reported hypertension
No hypertension 1 332 80.7 379 96.4 443 89.5 441 99.3 1 263 94.8
Yes 318 19.3 156 99.4 54 98.2* 104 98.1 314 98.7* 0.001
Plaque Index <30% 58 3.5 11 64.7 7 21.2 6 75.0 24 41.4
1 592 96.5 524 98.3* 490 94.8* 539 99.5* 1 553 97.6* 0.000
SYDOXH)LVKHUVH[DFWWHVWWRDVVHVVGLIIHUHQFHVEHWZHHQSUHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQIRUHDFKYDULDEOH
and city
SYDOXH)LVKHUVH[DFWWHVWWRDVVHVVGLIIHUHQFHVEHWZHHQSUHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQLQWKHWRWDOVDPSOHIRU
each variable
Table 2-3UHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQDFFRUGLQJWRULVNLQGLFDWRUVSHUFLW\
3UHYDOHQFHVHYHULW\DQGULVNLQGLFDWRUVRIJLQJLYDOLQÀDPPDWLRQLQDPXOWLFHQWHUVWXG\RQ6RXWK$PHULFDQDGXOWVDFURVVVHFWLRQDOVWXG\
J Appl Oral Sci. 528 VDPSOH LQGLYLGXDOV ZLWK \HDUV RI HGXFDWLRQ SUHVHQW D JLQJLYDO LQÀDPPDWLRQ SUHYDOHQFH WKDW is higher t han t hose w it h > 12 year s of educat ion ( pr evalence of 97.3% ver sus 92.2% , r espect ively, p< 0.0001) , but t his differ ence is m ost pr onounced
DQG VLJQL¿FDQW RQO\ IRU WKH VDPSOH RI 7XFXPiQ ( 94.9% ver sus 81.0% , p< 0.05) w hen t he t hr ee cit y sam ples ar e separat ely analyzed.
Pa r t i ci p a n t s w h o sm o k e p r e se n t a h i g h e r SUHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQDVFRPSDUHG w it h n on sm ok er s, b u t t h e d if f er en ce w as n ot VWDWLVWLFDOO\VLJQL¿FDQWS 7KRVHSDUWLFLSDQWV w it h self- r epor t ed diabet es and hyper t ension also SUHVHQWDVLJQL¿FDQWO\KLJKHUSUHYDOHQFHRIJLQJLYDO LQÀDPPDWLRQDVFRPSDUHGZLWKWKRVHQRWUHSRUWLQJ t hese condit ions. Wit hin cit ies, only in Tucum án t h er e is a st at ist ically sig n if ican t d if f er en ce in JLQJLYDO LQÀDPPDWLRQ SUHYDOHQFH EHWZHHQ WKRVH w ho self- r epor t hy per t ension and t hose w ho do not ( 98.2% ver sus 89.5% , r espect ively, p< 0.05) . $GXOWVZLWKDYLVLEOHSODTXHLQGH[SUHVHQW a si g n i f i ca n t l y h i g h e r p r e v a l e n ce o f g i n g i v a l i n f l a m m a t i o n t h a n t h o se w i t h v i si b l e p l a q u e index < 30% ( 97.6% ver sus 41.4% , r espect ively, p< 0.0001) ( Table 2) .
Table 3 descr ibes all clinical var iables exam ined in t his st udy ( m ean G- I ndex, m ean GBI , m ean VPI , and m ean CI ) . Regar ding all of t hese var iables, h igh er v alu es ar e obser v ed in in div idu als w it h KLJKHUJLQJLYDOLQÀDPPDWLRQSUHYDOHQFHFRPSDUHG w it h low er v alu es in h ealt hy adu lt s ( p< 0 . 0 0 1 ) in t he t hr ee cit ies. I n par t icipant s w it h gingival LQÀDPPDWLRQWKHPHDQ*,QGH[LQLQWHUSUR[LPDO sit es is 1 . 3 5 ( ± 0 . 4 3 ) an d in all sit es is 1 . 3 3 ZLWKRXWVWDWLVWLFDOO\VLJQL¿FDQWGLIIHUHQFHV St udy par t icipant s fr om Sant iago had t he highest av er ag e g in g iv al in d ex ( 1 . 7 3 ) com p ar ed w it h t hose fr om Tucum án and Por t o Alegr e, at 1 . 1 1 and 1.12, r espect ively ( p< 0.001) . The m ean VPI in in t er pr ox im al sit es is h igh er t h an t h e m ean plaque index for all sit es exam ined ( 81% ver sus 75% , r espect ively) for t he t ot al st udy populat ion. 6LJQL¿FDQWGLIIHUHQFHVIRUWKHFLW\RI3RUWR$OHJUH and Sant iago ar e found bet w een int er pr oxim al VPI and t ot al VPI . The rat es of int er pr ox im al VPI in LQGLYLGXDOVZLWKJLQJLYDOLQÀDPPDWLRQLQ6DQWLDJR Por t o Alegr e, and Tucum án ar e 89% , 80% , and 74% , r espect ively, w hile t he m ean int er pr oxim al VPI values in healt hy adult s ar e 45% , 30% , and 52% , for Sant iago, Tucum án, and Por t o Alegr e, UHVSHFWLYHO\ ZLWK VLJQL¿FDQW GLIIHUHQFHV EHWZHHQ t hem ( p< 0.001) ( Table 3) . The m ean CI rat es in LQGLYLGXDOVZLWKJLQJLYDOLQÀDPPDWLRQDUHLQ Port o Alegre, 74% in Tucum án, and 81% in Sant iago ZLWKVLJQL¿FDQWGLIIHUHQFHVEHWZHHQWKHPZKLOHWKH CI rat es in healt hy adult s are 52% , 26% , and 41% , r espect ively ( Table 3) . GBI is higher in individuals FODVVL¿HGDVKDYLQJJLQJLYDOLQÀDPPDWLRQDV com par ed w it h healt hy adult s ( 2% , p= 0.001) , and GBI is higher in Sant iago as com par ed w it h Por t o Alegr e and Tucum án ( Table 3) .
6HYHULW\RIJLQJLYDOLQÀDPPDWLRQ
Tables 4 a an d 4 b pr esen t m ean G- I n dex as
PORT O ALEGRE TUCUMÁN SANTIAGO T O T A L p -value* p -value** p-value*** p -value****
(n = 550)
(n = 550)
(n = 550)
(n = 1650)
V a riable Healthy GI Healthy GI Healthy GI Healthy GI n=15 n=535 n=53 n=497 n=5 n =545 n=73 n=1577 mean S D mean S D mean SD mean SD mean S D mean SD mean S D m ean S D G-Index 0 .44 0 .05 1 .12 0.34 0 .36 0.1 1 1.1 1 0.35 0.24 23.4 1.73 0.28 0.37 0.12 1.33 0.44 0.000 0.424 0.000 0.000 Inter G-Index 0.49 0.08 1.17 0.32 0.36 0.1 1 1.09 0.35 0.30 0.28 1.76 0.28 0.38 0.13 1.35 0.43 0.000 0.002 0.000 0.000 GBI 3.1 3.0 22.9 18.4 0 .02 2.3 2 3.0 19.7 2.2 2.2 7 4.1 23.4 2 .3 2.5 40.6 31.9 0 .000 0.408 0.000 0.000 VPI 35.8 18.8 70.5 18.1 29.4 12.1 73.5 20.0 44.2 21.9 8 1.6 1 8.1 31.7 14.8 75.2 19.4 0 .001 0.001 0.000 0.000 Inter VPI 45.1 2 2.5 79.0 17.1 30.0 12.5 74.0 20.3 52.4 2 7.1 88.9 1 6.0 3 4.6 17.7 81.2 18.8 0 .004 0.002 0.000 0.000 CI 52.0 34.9 88.5 21.1 25.9 26.9 73.8 32.0 41.2 28.5 8 1.1 2 7.2 3 2.0 30.2 8 1.3 27.7 0 .003 0.000 0.000 0.003 T a ble A
verage G-Index, Interproximal Inter G-Index, Gingival Bleeding Index (GBI), V
isual Plaque Index (VPI), Interproximal VPI, and
Calculus Index (CI)
DFFR UG LQ J WR WK H RFFX UUH QFH R IJ LQ JL YD OL QÀD PPD WLR Q * ,
G-Index, Gingival Index; Inter G-Index, Interproximal Gingival Index; GBI, Gingival Bleeding Index; VPI, V
isual Plaque Index, I
nter VPI, Interproximal V
isual Plaque Index; CI,
& DO FX OX V ,Q GH [ 0D QQ : KL WQ H\ WH VW R U.UX VND O: DO OLV DG MX VW HG S YD OX H IR UVL JQ L¿FD QFH D V DS SUR SUL DW H WR D VVH VV G LII HUH QFH V EH WZ HH Q KH DO WK \ YH UVX V JL QJ LYD OL QÀD PPD WLR Q IR UD OO FL WLH V SUH YD OH QFH R IJ LQ JL YD OL QÀD PPD WLR Q 3R UWR $O HJ UH Y HU VX V 7X FX Pi Q S UH YD OH QFH R IJ LQ JL YD OL QÀD PPD WLR Q 3R UWR $O HJ UH Y HUVX V 6D QW LD JR D QG S UH YD OH QFH R IJ LQ JL YD O LQ ÀD PPD WLR Q 7X FX Pi Q YH UVX V 6D QW LD JR
CARVAJAL P, GÓMEZ M, GOMES S, COSTA R, TOLEDO A, SOLANES F, ROMANELLI H, OPPERMANN R, RÖSING C, GAMONAL J
J
Appl Oral Sci.
529
Gingival Index Interproximal Gingival Index Gingival Bleeding Index Age
(years)
Mean ,& p-value * p-value ** p-value *** mean ,& p-value * p-value ** p-value *** mean ,& p-value * p-value ** p-value ***
PORTO
ALEGRE
18-19 1.00 0.89,1.11 0.005 1.06 0.95,1.16 0.010 18.5 1.0,56.0 0.344
20-29 1.07 1.01,1.13 1.12 1.07,1.18 21.1 0.0,72.0
30-39 1.07 1.02,1.13 1.13 1.07,1.18 20.6 1.0,78.0
40-49 1.11 1.05,1.18 1.16 1.10,1.22 22.3 1.0,94.0
1.19 1.14,1.25 1.23 1.18,1.28 25.9 0.0,100
TUCUMÁN 18-19 1.15 1.00,1.29 0.188 0.683 1.12 0.97,1.27 0.229 2.263 23.6 15.9,31.3 0.285 1.358
20-29 1.07 1.01,1.13 2.535 1.05 1.00,1.11 0.078 21.0 18.0,24.1 2.333
30-39 1.10 1.04,1.16 1.175 1.07 1.01,1.13 0.556 21.9 18.8,25.0 1.415
40-49 1.08 1.01,1.16 1.043 1.06 0.99,1.14 0.042 21.6 17.0,26.2 0.422
1.17 1.11,1.23 2.167 1.15 1.08,1.21 0.093 26.4 22.7,30.1 2.969
SANTIAGO 18-19 1.51 1.34,1.67 0.000 0.000 0.005 1.55 1.39,1.70 0.000 0.000 0.000 57.1 44.8,69.4 0.000 0.000 0.000
20-29 1.66 1.61,1.70 0.000 0.000 1.68 1.64,1.73 0.000 0.000 67.1 63.0,71.2 0.000 0.000
30-39 1.72 1.66,1.79 0.000 0.000 1.76 1.70,1.82 0.000 0.000 74.2 69.3,79.1 0.000 0.000
40-49 1.77 1.71,1.82 0.000 0.000 1.8 1.75,1.86 0.000 0.000 77.7 73.3,82.2 0.000 0.000
1.78 1.74,1.81 0.000 0.000 1.8 1.77,1.84 0.000 0.000 78.8 75.8,81.7 0.000 0.000
TOTAL 18-19 1.21 1.12,1.31 0.000 1.23 1.14,1.32 0.000 32.5 26.2,38.7 0.002
20-29 1.28 1.24,1.33 1.3 1.26,1.34 37.7 34.6,40.8
30-39 1.28 1.23,1.33 1.3 1.25,1.35 37.4 34.0,40.8
40-49 1.33 1.28,1.39 1.36 1.30,1.41 41.6 37.7,45.5
1.40 1.36,1.44 1.42 1.38,1.45 45.2 42.4,48.0
.UXVNDO:DOOLVDGMXVWHGSYDOXHIRUVLJQL¿FDQFHWRDVVHVVGLIIHUHQFHVEHWZHHQDJHVYHUVXVHDFK,QGH[E\FLW\DQGWRWDOSYDOXHGLIIHUHQFHVEHWZHHQ3RUWR$OHJUHYHUVXV Tucumán or Santiago in each Index (p-value**).
differences between Tucumán versus Santiago in each Index (p-value***)
Table 4a- Average Gingival Index (total and interproximal) and average Gingival Bleeding Index by age and city
3U
HY
DOH
QF
HV
HY
HUL
W\
D
QG
ULV
NLQ
GLF
DWR
UV
R
IJ
LQ
JLY
DOL
QÀ
DP
P
DWL
RQ
LQ
DP
XOWL
F
HQ
WH
UV
WX
G\
R
Q6R
XWK
$
P
HUL
FD
QD
GX
OWV
D
FU
RV
VV
HF
WLR
QD
OV
WX
G\
J
Appl Oral Sci.
530
MILD GI MODERATE GI SEVERE GI
Age (years)
n ,& n ,& n ,& p-value* p-value**
PORTO ALEGRE
18-19 13 54.2 34.2,72.9 11 45.8 27.1,65.8 0 0.0
20-29 37 37.8 28.7,47.8 61 62.2 52.2,71.3 0 0.0
30-39 54 47.0 38.0,56.1 57 49.6 40.5,58.7 4 3.5 1.3,9.0 0.090
40-49 41 40.2 31.1,50.0 58 56.9 47.0,66.2 3 2.9 0.9,8.8
64 32.7 26.4,39.6 126 64.3 57.3,70.7 6 3.1 1.4,6.7
TUCUMÁN 18-19 12 41.4 24.9,60.0 16 55.2 36.8,72.2 1 3.5 0.4,21.5
20-29 55 44.0 35.5,52.9 69 55.2 46.4,63.7 1 0.8 0.1,5.5
30-39 48 41.7 33.0,51.0 65 56.5 47.3,65.3 2 1.7 0.4,6.7 0.300
40-49 42 48.8 38.4,59.4 41 47.8 37.3,58.3 3 3.5 1.1,10.4
51 35.9 28.4,44.2 90 63.4 55.1,70.9 1 0.7 0.1,4.9
SANTIAGO 18-19 3 12.5 4.0,33.0 21 87.5 67.0,96.0 0 0.0 0.007
20-29 2 1.6 0.4,6.2 118 93.7 87.8,96.8 6 4.8 2.1,10.2 0.000
30-39 6 6.0 2.7,12.7 90 89.1 81.3,93.9 5 5.0 2.1,11.4 0.230 0.000
40-49 3 2.9 0.9,8.8 93 91.2 83.8,95.4 6 5.9 2.7,12.5 0.000
4 2.1 0.8,5.4 176 91.7 86.8,94.8 12 6.3 3.6,10.7 0.000
TOTAL 18-19 28 36.4 26.4,47.7 48 62.3 51.0,72,5 1 1.3 0.2,8.7
20-29 94 26.9 22.5,31.8 248 71.1 66.1,75.6 7 2.0 1.0,4.2
30-39 108 32.6 27.8,37.9 212 64.1 58.7,69.1 11 3.3 1.9,5.9 0.019
40-49 86 29.7 24.7,35.2 192 66.2 60.6,71.4 12 4.1 2.4,7.2
119 22.5 19.1,26.2 392 74 70.0,77.5 19 3.6 2.3,5.6
Chi-square test, to assess differences between ages versus severity for each city and total (p-value*), differences between cities by each group (p-value**) Table 4b-6HYHULW\PLOGPRGHUDWHDQGVHYHUHRIJLQJLYDOLQÀDPPDWLRQ*,per age and city
CAR
V
AJAL
P
, GÓMEZ M, GOMES S, COST
A
R, T
OLEDO
A, SOLANES F
, ROMANELLI H, OPPERMANN R, RÖSING C, GAMONAL
J
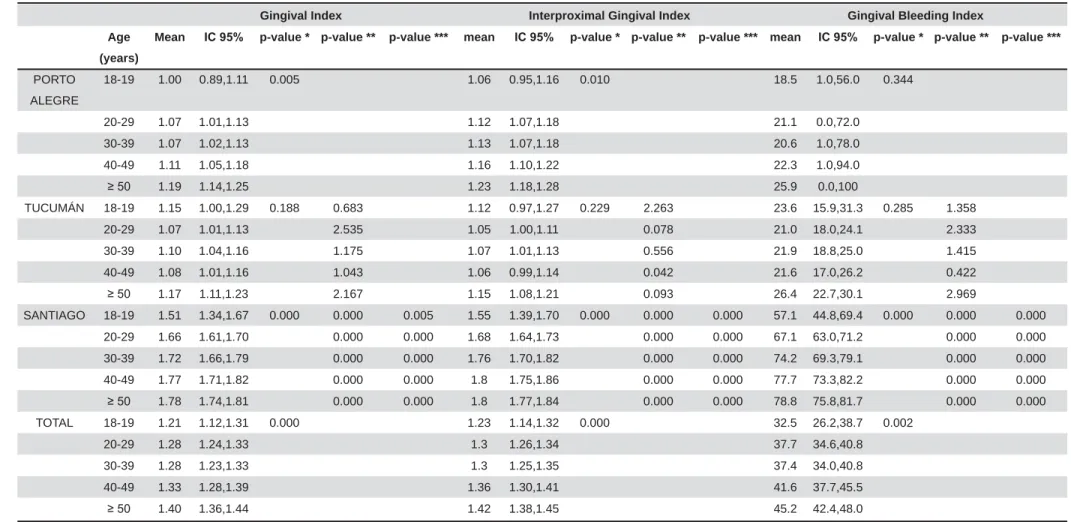
J Appl Oral Sci. 531 rest rict ed t o int erproxim al surfaces as well as m ean GBI according t o age and cit y. GBI m eans of 32.5% , 37.7% , 37.4% , 41.6% , and 45.2% ar e found for 18- 19 year olds, 20- 29 year olds, 30- 39 year olds, \HDUROGVDQG\HDUROGVUHVSHFWLYHO\ ( Table 4a) . Par t icipant s fr om Sant iago show ed t he highest m ean GBI ( Table 4a) . Regarding t he severit y RI JLQJLYDO LQÀDPPDWLRQ RI SDUWLFLSDQWV H[DPLQHGKDYHPLOGJLQJLYDOLQÀDPPDWLRQ KDYH PRGHUDWH JLQJLYDO LQÀDPPDWLRQ DQG KDYHVHYHUHJLQJLYDOLQÀDPPDWLRQ,Q6DQWLDJRWKH vast m aj or it y of adult s pr esent m oderat e gingival LQÀDPPDWLRQDQGIRUDOODJHJURXSVWKH JLQJLYDO LQÀDPPDWLRQ SUHYDOHQFH LV KLJKHU WKDQ w hat is obser v ed in Por t o Alegr e and Tucum án ( Table 4b) .
5LVNLQGLFDWRUVRIJLQJLYDOLQÀDPPDWLRQ Th e m u lt iv ar iat e log ist ic r eg r ession m od el, w hich was designed t o assess indicat or s t hat could EH UHODWHG WR JLQJLYDO LQÀDPPDWLRQ SUHYDOHQFH *,QGH[LQWKHDGXOWVDPSOHVGHPRQVWUDWHV t hat subj ect s w it h higher CI m ean ( OR= 18.59) ; ZLWKD93,25 OLYLQJLQ6DQWLDJR 25 KDYLQJ \HDUV RI VFKRROLQJ ( OR= 2.18) , and fem ales ( OR= 1.93) are m ore likely WRSUHVHQWJLQJLYDOLQÀDPPDWLRQ7KLVPRGHOZDV adj ust ed for age, pr esence of diabet es, and self-r epoself-r t ed hypeself-r t ension and sm oking ( Table 5) .
D I SCUSSI ON
The populat ion exam ined in t he pr esent st udy is com pr ised of a random sam ple of indiv iduals aging 18 year s or older fr om Por t o Alegr e ( Brazil) , Tu cu m án ( Ar gen t in a) , an d San t iago ( Ch ile) . To RXUNQRZOHGJHWKLVLVWKH¿UVWVWXG\FRQGXFWHGWR DVVHVVWKHSUHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQLQ a r epr esent at ive sam ple of adult populat ions fr om t hr ee Lat in Am er ican cit ies. The sam pling st rat egy t hat w e em ployed was successful in achieving a represent at ive and balanced sam ple of part icipant s, since t he individuals exam ined in each age group for each of t he t hr ee cit ies ar e in t he sam e pr opor t ion as in t he w hole st udy populat ion for t he t hr ee cit ies com bined. I n t his st udy, 95.6% of t he 1650 adult s exam ined from t hree Sout h Am erican cit ies present D*,QGH[7KLVLQIRUPDWLRQFRUURERUDWHVWKH dat a report ed for adult s from Jordan, China, and t he Unit ed St at es of Am erica, w hich dem onst rat ed t hat DGXOWVZLWKD*,QGH[FRPSULVH and 93. 9% of t heir r espect iv e populat ions1, 21, 30.
Com par in g ou r r esu lt s w it h t h at fr om pr ev iou s st udies is som ewhat hindered by t he use of different nom enclat ure and diagnost ic crit eria across st udies. Th e Co m m u n i t y Per i o d o n t a l I n d ex ( CPI ) w a s used t o r epor t t he occur r ence of pr obing pocket GHSWKFDOFXOXVDQGJLQJLYDOLQÀDPPDWLRQLQWKH
Hungar ian adult populat ion, and gingival bleeding
( CPI = 1) was obser ved in 8% of t he populat ion15.
Th e Nat ion al Healt h an d Nu t r it ion Ex am in at ion Sur v ey I I I ( NHANES I I I ) conduct ed in t he USA bet w een 1988- 1994 dem onst rat ed t hat 50% of t he DGXOW 86$ SRSXODWLRQ KDG JLQJLYDO LQÀDPPDWLRQ
using gingival bleeding as t he cr it er ion3. A st udy
conduct ed in I t aly, using bleeding on pr obing ( BoP) as t he cr it er ion, det er m ined t hat t he pr evalence of individuals show ing at least one sit e posit ive for
BoP w as 99%11. All t he afor em ent ioned st udies
d e m o n st r a t e t h a t t h e o ccu r r e n ce o f g i n g i v a l LQÀDPPDWLRQLVDOPRVWXQLYHUVDOO\FRUUHODWHGZLWK poor gingival condit ions. I n addit ion, t her e is a lar ge discussion in t he lit erat ur e r egar ding how t o GH¿QHGLVHDVHFULWHULD,WZRXOGEHLQWHUHVWLQJWR develop guidelines t o suggest w hich cr it er ia should be st andar dized for use in epidem iological st udies for gingival condit ions16. Concer ning t he sever it y of
JLQJLYDOLQÀDPPDWLRQWKHSUHVHQWVWXG\VKRZVWKDW RIDGXOWVKDYHPLOGJLQJLYDOLQÀDPPDWLRQ 7 4 . 0 % h av e m o d er at e g i n g i v al i n f l am m at i o n , DQG KDYH VHYHUH JLQJLYDO LQÀDPPDWLRQ ,Q cont rast , represent at ive st udies conduct ed in Europe and Aust ralia dem onst rat ed t hat t he pr evalence of VHYHUHJLQJLYDOLQÀDPPDWLRQLVFRPSDUDEO\PXFK higher ( 17% and 19. 7% , r espect ively ) in t hese populat ions15,17. The m ult ivariat e logist ic regression
m odels t hat w e em ployed show t hat a fem ale w it h \HDUV RI VFKRROLQJ D KLJKHU GHQWDO FDOFXOXV LQGH[ RI 93, DQG OLYLQJ LQ 6DQWLDJR KDV an in cr eased lik elih ood of p r esen t in g g in g iv al LQÀDPPDWLRQ ZKHQ DGMXVWLQJ IRU DJH SUHVHQFH of diabet es, and self- r epor t ed hy per t ension and sm oking. I n t his st udy, t o live in Sant iago was a risk indicat or for present ing GI . I t could be because t h ese su b j ect s h ad low er or al h y g ien e h ab it s com par ed w it h t hose fr om t he ot her cit ies. I ndeed, subj ect s w it h pr esence of GI belonging t o Sant iago had a higher average per cent age of VPI , com par ed w it h subj ect s w it h GI of Tucum án and Por t o Alegr e. I n fact , t he plaque index has been associat ed w it h LQFUHDVHG SUHVHQFH RI JLQJLYDO LQÀDPPDWLRQ DQG w or st level of oral hygiene in ot her populat ions9.
Ther e ar e lim it ed st udies at t he Lat in Am er ican level on t he pr evalence of per iodont al condit ions27,
ZKLFKDOORZFRQWUDVWZLWKWKH¿QGLQJVLQWKLVVWXG\ Alt hough subj ect s belonging t o Sant iago pr esent JUHDWHU JLQJLYDO LQÀDPPDWLRQ DQG LQFUHDVHG ULVN of it , is based w it h t hose r epor t ed for t hat count r y, w her e Chilean adult s had a high pr evalence of per iodont al dest r uct ion and indicat or s of gingival LQÀDPPDWLRQ12.
Th e p r e s e n t s t u d y a l s o d e m o n s t r a t e s a socioeconom ic gradient in t he oral healt h of t he p op u lat ion s ex am in ed . Par t icip an t s f r om low er VRFLRHFRQRPLFJURXSVSUHVHQWVLJQL¿FDQWO\SRRUHU gingival healt h as com par ed w it h par t icipant s in
3UHYDOHQFHVHYHULW\DQGULVNLQGLFDWRUVRIJLQJLYDOLQÀDPPDWLRQLQDPXOWLFHQWHUVWXG\RQ6RXWK$PHULFDQDGXOWVDFURVVVHFWLRQDOVWXG\
J Appl Oral Sci. 532
h ig h er socioecon om ic g r ou p s4. I n t h is r eg ar d ,
dif f er en t ex plan at ion s h av e been r aised in t h e OLWHUDWXUH WR H[SODLQ VXFK ¿QGLQJV )RU H[DPSOH t hose in low er socioeconom ic sit uat ions ar e also m or e likely t o sm oke, and sm oking has been found DVDVLJQL¿FDQWULVNIDFWRUIRUSHULRGRQWLWLV10. On t he
ot her hand, individuals w it h higher socioeconom ic st at us ar e likely t o have m or e posit ive at t it udes r egar ding oral hygiene and self- car e, and bet t er access t o available healt h car e opt ions. Ther efor e, low incom es and low levels of educat ion seem t o be variables wit h good predict abilit y for periodont al
diseases77KHSUHYDOHQFHRIJLQJLYDOLQÀDPPDWLRQ
in fem ales found in t he pr esent st udy cont radict s r esu lt s f r om Gr eece, w h er e w om en h av e been show n t o have bet t er oral hy giene and gingival st at us t han m en22. Per haps t his differ ence is m or e
about cult ur e t han gender. I t should be not ed t hat only w hen adj ust ing t he m ult ivar iat e m odel by confounding var iables, fem ale gender appear s as a possible r isk indicat or for t he pr esence of gingival LQÀDPPDWLRQ2QWKHRWKHUKDQGWKHORQJLWXGLQDO UHFRYHU\RIEOHHGLQJVLWHVZDVSRVLWLYHO\LQÀXHQFHG in fem ales25.
Re g a r d i n g t h e se l f - r e p o r t e d d i a b e t e s a n d hyper t ension am ong our par t icipant s, 7.4% have diabet es and 19.3% have hypert ension. Part icipant s w i t h sel f - r ep o r t ed d i ab et es an d h y p er t en si o n p r e se n t a si g n i f i ca n t l y h i g h e r p r e v a l e n ce o f JLQJLYDO LQÀDPPDWLRQ WKDQ WKRVH QRW UHSRUWLQJ t hese condit ions. Pr evious st udies have r epor t ed com p ar ab le r esu lt s r eg ar d in g t h is associat ion bet w een t ype 2 diabet es and per iodont al disease20.
:H¿QGWKDWFXUUHQWVPRNHUVFRPSULVH of our t ot al st udy par t icipant s, and t hese sm oker s pr esent a slight ly higher pr evalence of gingival LQÀDPPDWLRQ WKDQ QRQVPRNHUV LQ RXU VWXG\ EXW WKLV¿QGLQJZDVQRWVWDWLVWLFDOO\VLJQL¿FDQW7KHVH UHVXOWVFRQWUDVWZLWKWKH¿QGLQJVRI0OOHUHWDO25
( 2002) , in w hich st udy par t icipant s ( soldier s of t he Ger m an Ar m ed For ces ser ving bet w een Decem ber 1 9 9 9 an d May 2 0 0 0 ) w h o sm ok ed w er e f ou n d t o have m or e pr evalent bleeding on pr obing and PRUHFDOFXOXVWKDQQRQVPRNHUV6PRNLQJZDV¿UVW LGHQWL¿HGDVDULVNIDFWRULQSHULRGRQWDOGLVHDVHV from an analysis of dat a by I sm ail, et al.18 from dat a
collect ed fr om 1971 t o 1975. An analysis by t he Nat ional Healt h and Nut r it ion Exam inat ion Sur vey in t he U.S. ( NHANES I ) was able t o dem onst rat e an associat ion bet w een sm oking and per iodont al diseases t hat was independent of oral hygiene, age, or ot her pr obable r isk fact or s. Since t hen, t her e has been enough evidence t o ident ify sm oking as a r isk fact or for per iodont it is13. St udies per for m ed in
random ly chosen gr oups of pat ient s dem onst rat ed t hat t obacco use and oral hygiene are risk indicat ors f o r p er i o d o n t i t i s; i n p ar t i cu l ar, sm o k er s w er e invar iably show n t o have a higher pr evalence and
T O T A L (n=1650) PORT O ALEGRE (n=550) T UCUMÁN (n=550) SANTIAGO (n=550) V ariables O R & , p-value OR & , p-value OR & , p-value OR & , p-value Gender Male Female 1.93 1.03,3.59 0.039 6.48 1.32,31.86 0.021 1 .59 0.72,3.53 0.254 0.00 0.00 0.997
Education >12 (years)
2.18 1.19,4.02 0.012 1 .29 0 .33,5.06 0.713 3.21 1.46,7.08 0.004 1 .88 0.24,15.06 0 .550 CI (mean) 18.59 7.13,48.50 0.000 25.66 3 .89,169.10 0.001 18.24 5.44,61.19 0.000 36.61 0.51,2634.86 0.099 VPI <30% 14.56 6 .75,31.40 0 .000 10.78 2 .06,56.49 0 .005 21.10 7 .33,60.71 0 .000 18.70 1.30,269.52 0 .031 City T ucumán Porto Alegre 1 .75 0.81,3.79 0.153 Santiago 7.17 2.58,19.93 0.000 /R JL VW LF UH JUH VVL RQ P RG HO IR UW KH S UH VH QFH R IJ LQ JL YD OL QÀD PPD WLR Q D YH UD JH * ,Q GH [ D GM XVW HG IR UJ HQ GH U DJ H H GX FD WLR QD OO HYH O VH OIUH SR UWH G GL DE HW HV V HO IUH SR UWH G K\S HUW HQ VL RQ VPR NL QJ YL VX DO S OD TX H LQ GH [ FD OFX OX V LQ GH [ IR UH DFK FL W\ DQ G IR UW KH WR WD OVD PS OH E \ FL W\ 7 KH YD ULD EO HV WK DW D UH VW DW LVW LFD OO\ VL JQ L¿FD QW IR UD Q\ FL W\ RU WR WK H WR WD OD UH VK RZ Q Ta b le 5 -0 XO WLYD ULD WH D QD O\VH V RI ID FW RUV DVVR FL DW HG Z LWK J LQ JL YD OL QÀD PPD WLR Q D YH UD JH * ,Q GH [ 7K H YD ULD EO HV WK DW D UH VW DW LVW LFD OO\ VL JQ L¿FD QW IR U DQ \ FL W\ RU WR the total are shown
CARVAJAL P, GÓMEZ M, GOMES S, COSTA R, TOLEDO A, SOLANES F, ROMANELLI H, OPPERMANN R, RÖSING C, GAMONAL J
J Appl Oral Sci. 533 pr ogr ession of dest r uct ive per iodont al diseases24.
Ther e is a st r ong need in Lat in Am er ica t o focus on m ore effect ive int ervent ion program s t o prevent and cont r ol per iodont al diseases at nat ional levels. I t should be em phasized t hat since per iodont it is begins as gingivit is, it is r easonable t o conclude WKDW WKH FRQWURO RI JLQJLYDO LQÀDPPDWLRQ FDQ EH EHQH¿FLDOWRWKHSRSXODWLRQDVDZKROHWRSUHYHQW bot h t he onset and t he pr ogr ession of per iodont al d a m a g e ca u se d b y p e r i o d o n t i t i s. W h i l e t h e disabilit y- adj ust ed life- years ( DALYs) due t o severe per iodont it is and unt r eat ed car ies have incr eased since 1990, t hose due t o sever e t oot h loss have decreased. Oral condit ions are all ranked am ong t he
t op 100 det ailed causes of DALYs237KHVH¿QGLQJV
highlight t he challenge in responding t o t he diversit y of ur gent oral healt h needs w or ldw ide, par t icular ly in developing com m unit ies.
*LQJLYDOLQÀDPPDWLRQZKLFKFRXOGEHFRQVLGHUHG a r ever sible and easily cont r olled disease in st age of gingivit is, is found t o be highly pr evalent am ong adult st udy part icipant s from t he t hree cit ies in Lat in Am er ica of t his st udy. I n addit ion, t hese individuals ar e also m or e likely t o at t end pr event ive or follow-up v isit s because socioeconom ic charact er ist ics VXFKDVLQFRPHDQGOHYHORIHGXFDWLRQLQÀXHQFH t h e pat t er n an d t y pe of den t al ser v ices u sed6.
Poor awar eness of t he im por t ance of per iodont al h ea l t h a n d t h e co n seq u en ces o f t h e d i sea se am ong t he public and even am ong som e general dent al pract it ioner s is one of t he m ost com m on r easons for failur e t o cont r ol and t r eat per iodont al
diseases effect ively on a populat ion basis19. We
r ecom m end t hat effect ive int er vent ion pr ogram s f or t h e p r ev en t ion an d con t r ol of p er iod on t al diseases should be im plem ent ed at nat ional levels, and t he need for such im plem ent at ion seem s t o be ext r em ely im por t ant in t he t hr ee count r ies w e st udied here. We believe t hat t here is a st rong need acr oss Lat in Am er ica t o im pr ove t he populat ion’s self- awareness about oral healt h t hrough bet t er oral healt h educat ion t hat pr om ot es good oral hygiene and r egular dent al car e.
Th i s st u d y w a s a i m e d t o d e t e ct g i n g i v a l LQÀDPPDWLRQLQVWHDGRIHVWDEOLVKLQJWKHGLDJQRVLV of eit h er g in g iv it is or p er iod on t it is in or d er t o det erm ine t he risk of gingivit is onset or periodont it is pr ogr ession in t he st udy populat ion.
CON CLUSI ON S
&RQVLGHULQJRXU¿QGLQJVWRJHWKHULWLVSRVVLEOH WR FRQFOXGH WKDW JLQJLYDO LQÀDPPDWLRQ LV KLJKO\ prevalent in t he t hree Lat in Am erican cit ies st udied. Overall, 95.6% of t he par t icipant s aging 18 year s RU ROGHU KDG JLQJLYDO LQÀDPPDWLRQ FRQVLGHULQJ t hat m or e t han t w o- t hir ds have m oderat e gingival i n f l am m at i o n an d 3 . 6 % h av e sev er e g i n g i v al
LQÀDPPDWLRQ ,Q JHQHUDO WHUPV WKH SUHVHQFH RI JLQJLYDOLQÀDPPDWLRQLVSRVLWLYHO\DVVRFLDWHGZLWK r isk in d icat or s su ch as g en d er, socioecon om ic var iables, and t he pr esence of plaque. The pr esent invest igat ion ser ves as t he basis for a longit udinal an aly sis of or al h ealt h in popu lat ion s of Sou t h Am er ican ad u lt s, an d f or t h e d ev elop m en t of st rat egies t o im pr ove t he healt h car e syst em s t hat ser ve t hem .
ACKN OW LED GEM EN TS
The pr esent st udy was kindly suppor t ed by an independent research grant from Colgat e Palm olive, Piscat away, New Jersey, Nº CRO- 2013- 03- GI N- SC-%67KHDXWKRUVGHFODUHWKDWWKHUHLVQRFRQÀLFWRI int er est for any aut hor s r elat ed t o t he cont ent of t he pr esent analysis.
REFEREN CES
1- Ababneh KT, Abu Hwaij ZM, Khader YS. Pr evalence and r isk indicat or s of gingivit is and per iodont it is in a m ult i- cent r e st udy in Nort h Jordan: a cross sect ional st udy. BMC Oral Healt h. 2012; 12: 1. 2- Albandar JM. Periodont al diseases in Nort h Am erica. Periodont ol 2000. 2002; 29: 31- 69.
3- Albandar JM, Br unelle JA, Kingm an A. Dest r uct ive per iodont al disease in adult s 30 year s of age and older in t he Unit ed St at es, 1988- 1994. J Per iodont ol. 1999; 70( 1) : 13- 29.
4- Aust ralian Resear ch Cent r e for Populat ion Oral Healt h, The Univer sit y of Adelaide, Sout h Aust ralia. Per iodont al diseases in t he Aust ralian adult populat ion. Aust Dent J. 2009; 54( 4) : 390- 3. 5- Baehni PC, Takeuchi Y. Ant i- plaque agent s in t he pr event ion of
ELR¿OPDVVRFLDWHGRUDOGLVHDVHV2UDO'LV6XSSO
6- Bar bat o PR, Muller Nagano HC, Zanchet FN, Boing AF, Per es MA. Toot h loss an d associat ed socioecon om ic, dem ogr aph ic, and dent al- car e fact or s in Brazilian adult s: an analy sis of t he Brazilian Oral Healt h Sur vey, 2002- 2003. Cad Saude Publica. 2007; 23( 8) : 1803- 14.
7- Bur t B, Resear ch, Science and Therapy Com m it t ee of t he Am erican Academ y of Periodont ology. Posit ion paper: epidem iology of per iodont al diseases. J Per iodont ol. 2005; 76( 8) : 1406- 19. 8 - Cr a i g RG. D e st r u ct i v e p e r i o d o n t a l d i se a se s, sy st e m i c
LQÀDPPDWLRQDQGDWKHURVFOHURWLFFRPSOLFDWLRQVWKHHPHUJLQJUROH
of t he dent al pr ofession. J Calif Dent Assoc. 2009; 37( 11) : 773- 7. 9 - Cr o co m b e LA, Br en n an D S, Sl ad e GD, Lo c D O. I s sel f int er dent al cleaning associat ed w it h dent al plaque levels, dent al calculus, gingivit is and per iodont al disease? J Per iodont al Res. 2012; 47( 2) : 188- 97.
10- Do LG, Slade GD, Robert s-Thom son KF, Sanders AE. Sm oking-at t ribut able periodont al disease in t he Aust ralian adult populoking-at ion. J Clin Per iodont ol. 2008; 35( 5) : 398- 404.
11- Far ina R, Scapoli C, Car r ier i A, Guar nelli ME, Tr om belli L. Pr evalence of bleeding on pr obing: a cohor t st udy in a specialist per iodont al clinic. Quint essence I nt . 2011; 42( 1) : 57- 68. 12- Gam onal J, Mendoza C, Espinoza I , Muñoz A, Ur zúa I , Aranda W, et al. Clinical at t achm ent loss in Chilean adult populat ion: Fir st Chilean Nat ional Dent al Exam inat ion Sur vey. J Per iodont ol. 2010; 81( 10) : 1403- 10.
13- Genco RJ, Borgnakke WS. Risk fact ors for periodont al disease. Per iodont ol 2000. 2013; 62( 1) : 59- 94.
14- Haas AN, Wagner MC, Opper m ann RV, Rösing CK, Albandar JM, Su sin C. Risk f act or s f or t h e pr ogr ession of per iodon t al at t achm ent loss: a 5- year populat ion- based st udy in Sout h Brazil. J Clin Per iodont ol. 2014; 41( 3) : 215- 23.
3UHYDOHQFHVHYHULW\DQGULVNLQGLFDWRUVRIJLQJLYDOLQÀDPPDWLRQLQDPXOWLFHQWHUVWXG\RQ6RXWK$PHULFDQDGXOWVDFURVVVHFWLRQDOVWXG\
J Appl Oral Sci. 534
15- Herm ann P, Gera I , Borbély J, Fej érdy P, Madléna M. Periodont al
KHDOWKRIDQDGXOWSRSXODWLRQLQ+XQJDU\¿QGLQJVRIDQDWLRQDO
sur vey. J Clin Per iodont ol. 2009; 36( 6) : 449- 57.
16- Hugoson A, Nor der yd O. Has t he pr evalence of per iodont it is changed dur ing t he last 30 year s? J Clin Per iodont ol. 2008; 35( 8 Suppl) : 338- 45.
17- Hugoson A, Sj ödin B, Norderyd O. Trends over 30 years, 1973-2003, in t he pr evalence and sever it y of per iodont al disease. J Clin Per iodont ol. 2008; 35( 5) : 405- 14.
18- I sm ail AI , Bur t BA, Ek lund SA. Epidem iologic pat t er ns of sm oking and per iodont al disease in t he Unit ed St at es. J Am Dent Assoc. 1983; 106( 5) : 617- 21.
19- Jin LJ, Arm it age GC, Klinge B, Lang NP, Tonet t i M, William s RC. Global oral healt h inequalit ies: t ask gr oup - per iodont al disease. Adv Dent Res. 2011; 23( 2) : 221- 6.
20- Kaur G, Holt fr et er B, Rat hm ann W, Schwahn C, Wallaschofski H, Schipf S, et al. Associat ion bet w een t ype 1 and t ype 2 diabet es w it h p er iod on t al d isease an d t oot h loss. J Clin Per iod on t ol. 2009; 36( 9) : 765- 74.
21- Li Y, Lee S, Huj oel P, Su M, Zhang W, Kim J, et al. Pr evalence an d sev er i t y o f g i n g i v i t i s i n Am er i can ad u l t s. Am J D en t . 2010; 23( 1) : 9- 13.
22- Mam ai- Hom at a E, Polychr onopoulou A, Topit soglou V, Oulis C, At hanassouli T. Per iodont al diseases in Gr eek adult s bet w een 1985 and 2005 - r isk indicat or s. I nt Dent J. 2010; 60( 4) : 293- 9.
23- Mar cenes W, Kassebaum NJ, Ber nabé E, Flaxm an A, Naghavi M, Lopez A, et al. Global bur den of oral condit ions in 1990- 2010: a syst em at ic analysis. J Dent Res. 2013; 92( 7) : 592- 7.
24- Mdala I , Olsen I , Haffaj ee AD, Socransky SS, Thor esen M, de Blasio BF. Com par ing clinical at t achm ent level and pocket dept h for pr edict ing per iodont al disease pr ogr ession in healt hy sit es of pat ient s w it h chr onic per iodont it is using m ult i- st at e Mar kov m odels. J Clin Per iodont ol. 2014; 41( 9) : 837- 45.
25- Müller HP, St aderm ann S, Heinecke A. Longit udinal associat ion bet w een plaqu e an d gin giv al bleedin g in sm ok er s an d n on -sm oker s. J Clin Per iodont ol. 2002; 29( 4) : 287- 94.
26- Offenbacher S, Barros SP, Paquet t e DW, Winst on JL, Biesbrock AR, Thom ason RG, et al. Gingival t ranscr ipt om e pat t er ns dur ing induct ion and r esolut ion of exper im ent al gingivit is in hum ans. J Per iodont ol. 2009; 80( 12) : 1963- 82.
27- Opper m ann RV, Haas AN, Rösing CK, Susin C. Epidem iology of per iodont al diseases in adult s fr om Lat in Am er ica. Per iodont ol 2000. 2015; 67( 1) : 13- 33.
6KLPDGD<7DEHWD.6XJLWD1<RVKLH+3UR¿OLQJELRPDUNHUV LQJLQJLYDOFUHYLFXODUÀXLGXVLQJPXOWLSOH[EHDGLPPXQRDVVD\$UFK
Oral Biol. 2013; 58( 6) : 724- 30.
29- St am m JW. Epidem iology of gingiv it is. J Clin Per iodont ol. 1986; 13( 5) : 360- 6.
30- Zhang J, Xuan D, Fan W, Zhang X, Dibar t S, De Vizio W, et al. Severit y and prevalence of plaque- induced gingivit is in t he Chinese populat ion. Com pend Cont in Educ Dent . 2010; 31( 8) : 624- 9.
CARVAJAL P, GÓMEZ M, GOMES S, COSTA R, TOLEDO A, SOLANES F, ROMANELLI H, OPPERMANN R, RÖSING C, GAMONAL J