Journal
of
Coloproctology
w w w . j c o l . o r g . b r
Case
report
New
surgical
approach
of
retrorectal
cystic
hamartoma
using
transanal
minimally
invasive
surgery
(TAMIS)
Pablo
Colsa
Gutiérrez
∗,
Mahgol
Kharazmi
Taghavi,
Rocío
Daniela
Sosa,
Angel
Pelayo
Salas,
Victor
Jacinto
Ovejero,
Jose
Luis
Ruiz,
Jose
Manuel
Gutiérrez
Cabezas,
Alfredo
Ingelmo
Setién
ServiceofGeneralandGastrointestinalSurgery,SierrallanaRegionalHospital,Cantabria,Spain
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15March2014 Accepted11August2014
Availableonline6September2014
Keywords:
Cystichamartoma Tailgutcyst Retrorectaltumor
Minimally-invasivesurgical procedures
a
b
s
t
r
a
c
t
Introduction:Tailgutcystsorcystichamartomasareraredevelopmentaltumorsofthe pre-sacralspace.Theirtrueincidenceisnotwellknownbutwemustthinkonitwhenwehave apatientwithamulticysticuncapsulatedtumoratpresacralspace.Tailgutcystsareoften asymptomatic,andinothercasespresentwithchronicperinealpain,constipationorrectal tenesmus.Theymustbetreatedtoavoidcomplicationssuchasinfections(perianalfistula orabscess)andmalignantdegenerations(usuallyadenocarcinoma).
Casereport:Onepatientwithanalpainwasdiagnosedwithaperianalabscess.Hewas oper-atedbutatthesecondmonthreviewaMRIrevealedamultilocularlesioninthepresacral suggestingthepresenceofaretrorectalcystichamartoma.
Anelectiveoperationwasperformedbyendoanalsurgicalapproach usingTAMIS.En blocresectionofthecystwasachievedwithsafemargins.Thepathologyresultreported retrorectalcystichamartoma.Thepatientwasasymptomaticwithnosignsofrecurrence insubsequentcontrols.
Ourexperience,despitebeingbasedononecase,isevidencethatTAMIS(Transanal Min-imallyInvasiveSurgery)allowsaminimallyinvasivedissectionwithsimilarbenefitsasthe useofTEM/TEOdevices.
©2014SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Nova
abordagem
cirúrgica
do
hamartoma
cístico
retrorretal
usando
cirurgia
transanal
minimamente
invasiva
(TAMIS)
Palavras-chave:
Hamartomacístico
r
e
s
u
m
o
Introduc¸ão:Tailgutcystsouhamartomascísticossãotumoresrarosdedesenvolvimentodo espac¸opré-sacral.Suaverdadeiraincidêncianãoébemconhecida,masdevemospensar
∗ Correspondingauthor.
E-mail:[email protected](P.C.Gutiérrez).
http://dx.doi.org/10.1016/j.jcol.2014.08.004
Tailgutcyst Tumorretrorretal Procedimentoscirúrgicos minimamenteinvasivos
nelequandotemosumpacientecomumtumoruncapsulatedmulticísticanoespac¸o pré-sacral.Hamartomascísticossãomuitasvezesassintomáticas,emoutroscasos, apresenta-secomdorperinealcrônica,constipac¸ãooutenesmoretal.Elesdevemsertratadospara evitarcomplicac¸ões,comoinfecc¸ões(fístulaperianalouabscesso)edegenerac¸õesmalignas (geralmenteadenocarcinoma).
RelatodeCaso: Umpacientecomdoranalfoidiagnosticadocomumabscessoperianal.Ele foioperado,masnarevisãodosegundomêsumaressonânciamagnéticarevelouumalesão multilocularnopré-sacral,sugerindoapresenc¸adeumhamartomacísticoretrorretal. Umaoperac¸ãoeletivafoirealizada porabordagemcirúrgicaendoanalusandoTAMIS. A ressec¸ãoemblocodocistofoiconseguidocommargensseguras.Oresultadodoexame patológicorelatouhamartomacísticoretrorretal.Opacienteencontrava-seassintomático, semsinaisderecidivaemcontrolesposteriores.
Anossaexperiência,apesardeserbaseadoemumdoscasos,asprovasqueTAMIS (cirur-giatransanalminimamenteinvasiva)permite umesvaziamentominimamenteinvasivo combenefíciossimilarescomoousodedispositivosdeMET/TEO.
©2014SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Retrorectal cystic hamartomas are rare congenital tumors derivedfrom the regression ofthe tailgut, which normally regressesduringtheseventhoreighthweekoftheembryonic phase.1
Mosthamartomasarenon-symptomaticretrorectal mul-ticysticmassesandusuallyappearinmiddle-agedwomen. Surgery isrequired totreat hamartomas. Multiplesurgical approacheshavebeendescribed,primarilyduetolocationof thetumorandattendantdifficulties.
Wepresentacaseofaretrorectalhamartomacysticina youngmalepatient,whodebutedwithaperianalabscessand wassurgicallytreatedusingatransanalapproach.We con-cludewithanexaminationofclinicalseriesandreviewsfound intheliteratureusingthePubMedelectronicdatabase.
Case
report
A24-year-oldmalearrivedattheemergencyroom complain-ingofanalpainthatworsenedoverseveralmonths.Hehad previouslyreceivedambulatorycare,wherehewasdiagnosed with an anal fissure and treated symptomatically. Despite treatment,thepatientcontinuedtocomplainofanalpain.
Thepatienthadbeentreatedintheemergencyroomon twoprioroccasions.Onthesecondoccasion,hesufferedfrom a38◦Cfeverandanalincontinence,whichprogressedtoliquid
overnight.
Onphysicalexamination,thepatient’sabdomenwassoft andpainless;theDRE(digitalrectalexamination)wasnot pos-siblebecauseofpain.
ApelvicCTscanwasreportedasaheterogeneous hypo-denseimageof3cm×3cm×6cmintherecto-sacrumspace
compatiblewithanoverthelevatoranimuscleabscess(Fig.1). Thepatientwas diagnosedwith aperianal abscessand decided to operate. Using an endoanal surgical approach,
Fig.1–Heterogeneoushypodenseimageinthe
recto-sacrumspacecompatiblewithabscessinpelvicCT scan.
palpation discovered a fluctuating cystic mass on, and extractedatransparent,odorlessandmucoidsubstance.
The patient was seen in consultation one week after surgery.Despitebeingfeverless,thepatientstillcomplained ofdiscomfortondefecationandtenesmus.Subsequent exam-inationswerescheduledinordertocontinuethestudy.
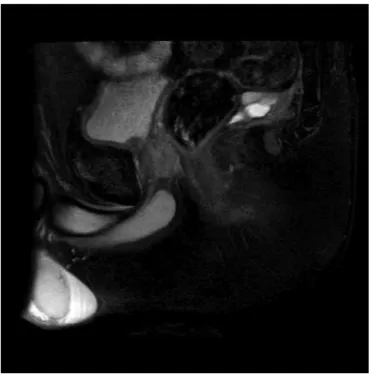
Atthe secondmonthreviewthe woundwasclosed.An MRI revealed amultilocular lesion of3cm×3.5cm×1.7cm
Fig.2–MRIrevealedamultilocularcysticmassinthe presacralspace.
considerwhetherthepatientsufferedfromaretrorectalcystic hamartoma.
An elective operation was performed. Given the previ-oushistory,we choseanendoanalsurgicalapproachusing TAMIS(Fig.4).Enblocresectionofthecystwasachievedwith safemargins.Thepathologyresultreportedretrorectalcystic hamartoma(Fig.5).Thepatientwasdischargedonthesecond dayfollowingtheoperation,andwasasymptomaticwithno signsofrecurrenceinsubsequentcontrols.
Fig.3–SagittalT2-weightedmagneticresonancescan suggestedthepresenceofamucidcontentcyst.
Fig.4–EndoanalsurgicalapproachusingTAMIS (TransanalMinimallyInvasiveSurgery).
Fig.5–Thepathologyresultreporteddifferenttypesof epitheliawithoutcryptsorvillisurroundedbya discontinuousmusclelayer.
Discussion
Retrorectaltumors
ThePre-sacrumor retrorectalspaceislocatedbetweenthe rectum,thepre-sacrumfascia,thelateralligaments,the per-itonealreflection,andtheWaldeyerfascia.Itusuallycontains structuresderivedfromneuroectoderm,notochord,gutand embryologicalremnants.
Thetrueincidenceofembryonarytumorsinthe retrorec-talspaceisnotknownbecausereportedfindingstendtobe incidentaltofindingsofasymptomaticlesions.
Predominanceinfemaleshasbeensubjecttoconsiderable debate, withsomeclaimsthat thisfinding couldbedueto regulargynecologicalandpelvicexaminations.2,3
Tailgutcysts
Thetailgutcystorcystichamartomaisatumorofthepresacral spacethatwasfirstdescribedin1885byMiddeldorf.5They derivedfromanembryonicremnantoftheprimitivebowel, asHjermstadetal.postulatedinthelargestcasereviewdone todate.6IfHjermstadiscorrect,theanalmarginmergeswith theprimitivegut(tailgut)aboveitsdistalend.Theoutcome ofthismergerisabagwithsquamouscubicalepitheliumin thepresacralspace.1,7Normally,thisvestigeregressesduring embryonicdevelopment,but whenthis doesnothappen,a cystichamartomaappears.
Patientsymptomsvaryandarerelatedtothelocation,size, mass,andthereforeinfectionsofthecyst.Mosttailgutcysts areasymptomaticfindingsduringaclinicalexaminationfor otherreasons(CTscan,MRI,Endorectalultrasound,etc.)For someauthors,50%ofhamartomaspresentwithchronic peri-nealpain,constipation,rectaltenesmus(aswepresentinour casereport),rectalbleedingorurinaryratechanges.Fever,or signsofperianalsuppurationintheperineum,suggests fis-tula,abscessandcomplicationsfromcystinfection.6,8,9This iswhymanypatientsarediagnosedfromretrorectalabscesses orfrommultipleinterventionsforrecurrentperianalfistula.
Diagnosis
Onphysicalexamination,mostpatientshavepalpablemass onDRE,whichisakeyconsiderationforanydiagnosis.There isasensibilitythatvariesbetween97%10and75%2described forthe DRE. In our case, the clinical picture debuted as a complicationofinfection thatledtoaninitialmisdiagnosis ofahighperirectalabscess.Rectalexaminationwaspainful andwhitishcontent orientedtothesuspecteddiagnosis.A colonoscopyallowedexaminationofendoluminalinjury,but bariumenemawasineffectiveasnoadditionalinformationis given.Imagingtestscansometimesbehelpful,becausethe presenceofamulticystic tumor,circumscribed and uncap-sulatedatapresacralspacelevel,leadstocystichamartoma diagnosesaswell.Withinimagingtestswedescribedtheuse ofendoscopy,MRIorCTandeco-endoanal4;endoanal ultra-soundisnotuseful.Itonlyallowsidentificationofthenature ofthecyst(jellytypeorwaterytype)anditsrelationtothe surroundingareas.11
TheCTshowsamasswithclearedgesandrevealsliquid orsofttissuecontent.Onerarelyfindscalcificationsinsidethe thinwall.11Inthecaseofacomplicatedcystduetoinfection ormalignization,weusuallyfindunevenmargins.1,11
TheMRIimagingisimportanttodeterminethemultiple cystcharacterofthetailgutanditsrelationtotheadjacent structures.TypicallythecystwillbehypointenseinT1wand hyperintenseinT2w sequence,and heterogeneouscontent canalso beseen resultingfrom the mucine, proteic mate-rialorintracystichemorrhage.11–13TheT2sequenceofacyst showingtractsinsideisalsocharacteristicofahamartoma, asKim et al.describes and similar to our case.12 Another finding isthepresenceofalittle peripheralcyst accompa-nyingthehamartoma.7Itisimportanttodeterminethe uni-ormulti-lobularnatureofthecyst becausethisestablishes thedifferentialdiagnosisbetweenhamartomaormultilocular cysticlymphangiomaversusotherpre-sacrumcysts.
In any event, we should avoidthe biopsy ofthe lesion becauseofahighriskofitslocaldisseminationanditslow outcomefordiagnosisconfirmation.
Inourcase,wedrainedthecystthroughtheanallumen which did notavoidthe lesion’sreproduction twomonths later.
Once the surgical piece has been processed, pathology will show different types of epithelia without crypts or villi surrounded by a discontinuous muscle layer (Fig. 5). Super-infectedcystsusuallypresentwallfibrosisandlossof definitionintheepitheliallining.
Treatment
Treatmentisbasedoncompleteresectionofthelesiontoavoid recurrence,infectionormalignantdegeneration.
The approach to the retrorectal space is latero-sacral, abdominalorperineal.
Thelatero-sacralparasacrococcigealapproachisthemost usedone,becauseitallowsagoodexpositionoftheanusand thelevatoranimuscleplan.
The abdominal approach, either laparotomy or laparoscopy,isindicatedonlywhenlargetumorsarepresent orifthetumorsgrowupwardsinsteadofdownwardstoward thepelvicarea.Theabdominallaparoscopicapproachgives us the advantage of a finer mesorectum dissection. The perinealaccessisdonewiththepatientinlithotomyposition. Incision is performed on the perineal raphe to reach the retrorectalspace.Howeverallofthesetechniqueshaveahigh rateofmorbidity.14,15
Inthepastfewyears,theuseofendoanalproceduresusing TEM/TEOdeviceshasincreasedtoavoidmorbidity.3,16–18 How-everaccessibilitytothesedevicesisrestrictedbecauseofhigh costanddifficultlearningcurves.19
The TAMIS (Transanal Minimally Invasive Surgery) achieves similar benefitsas the use ofTEM/TEO devices.20 TAMISuses asinglesitedevice, likeSILS(Covidien), which islubricatedandlocatedintheanalcanalmanually.Ithas threesiteswherewecanintroducetwo5mmandone10mm trocars (Fig. 4). The CO2 gas goes through the single site device cannula,being carefulnot to exceed 18mm Hg. In ourseriesweusea5mmand30gradesangulatedopticand conventionallaparoscopicmaterial.
Bothtechniquestrytoreachareasonableresectionwith theleastamountofdamagepossible.
Inthisway,TAMIShasproventobeareliablealternativeto TEM/TEOwiththesamebenefitsatalowercoast.
Conclusions
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. JohnsonAR,RosPR,HjermstadBM.Tailgutcyst:diagnosis withCTandsonography.AmJRoentgenol.1986;147:1309–11.
2. BuchsN,TaylorS,RocheB.Theposteriorapproachforlow rectaltumorsinadults.IntJColorectalDis.2007;22:381–5.
3. ZollerS,JoosA,DinterD,BackW,HorisbergerK,PostS,Palma P.Retrorectaltumors:excisionbytransanalendoscopic microsurgery.RevEspEnfermDig.2007;99:547–50.
4. KillingworthC,GadaczTR.Tailgutcyst(retrorectalcystic hamartoma):reportofacaseandreviewoftheliterature.Am Surg.2005;71:666–73.
5. MiddledorpfK.ZurKenntnissderangbornen sacralgeschwulst.VirchowsArch.1885;101:37–44.
6. LevertLM,VanRooyenW,VanDenBergenH.Cystsofthe tailgut.EurJSurg.1996;162:149–52.
7. YangDM,ParkCH,JinW,ChangSK,KimJE,ChoiSJ,etal. Tailgutcyst:MRIevaluation.AmJRoentgenol.
2005;184:1519–23.
8. WilliamsLS,RojianiAM,QuislingRG,MickleJP.Retrorectal cysthamartomasandsacraldysplasia:MRappearance.AmJ Neuroradiol.1998;19:1043–5.
9. LaQuagliaMP,FeinsN,ErakisA,HendrenWH.Rectal duplications.JPediatrSurg.1990;25:980–4.
10.JaoSW,BeartJrRW,SpencerRJ.Retrorectaltumors:mayor clinicexperience,1960–1979.DisColonRectum.
1985;28:644–52.
11.PrasantP,UttamG,PeacockM.Retrorectalhamartoma:a‘tail’ oftwocysts.IndianJRadiolImaging.2010;20(May):
129–31.
12.KimMJ,KimWH,KimNK,YunMJ,ParkYN,LeeJT,etal. Tailgutcyst:multilocularcysticappearanceonMRI.JComput AssistTomogr.1997;21:731–2.
13.MoulopoulosLA,KarvouniE,KehagiasD,DimopoulosMA, GouliamosA,VlahosL.MRimagingofcomplextail-gutcysts. ClinRadiol.1999;54:118–22.
14.ParksAG.Atechniqueforexcisingextensivevillous papillomatouschangesinthelowerrectum.ProcRSocMed. 1968;61:441–2.
15.MellgrenA,SirivongsP,RothenbergerDA,MadoffRD, Garcıa-AguilarJ.Islocalexcisionadequatetherapyforearly rectalcancer?DisColonRectum.1999;43:1064–71.
16.PalmaP,FreudenbergS,SamuelS,PostsS.Transanal endoscopicmicrosurgery:indicationsandresultsafter100 cases.ColorectalDis.2004;6:350–5.
17.DuekSD,KlugerY,GrunnerS,WeinbroumAA,KhouryW. Transanalendoscopicmicrosurgeryfortheresectionof submucosalandretrorectaltumors.SurgLaparoscEndosc PercutanTech.2013;23:66–8.
18.SerraAracilX,GómezDíazC,BombardóJuncaJ,MoraLópez L,AlcántaraMoralM,AyguavivesGarnicaI,NavarroSotoS. Surgicalexcisionofretrorectaltumourusingtransanal endoscopicmicrosurgery.ColorectalDis.2010;12: 594–5.
19.VandenBoezemPB,KruytPM,StommelMW,TobonMorales R,CuestaMA,SietsesC.Transanalsingle-portsurgeryforthe resectionoflargepolyps.DigSurg.2011;28:412–6.