SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Treatment
of
proximal
humeral
fractures
using
anatomical
locking
plate:
correlation
of
functional
and
radiographic
results
夽
Antonio
Carlos
Tenor
Junior
∗,
Alisson
Martins
Granja
Cavalcanti,
Bruno
Mota
Albuquerque,
Fabiano
Rebouc¸as
Ribeiro,
Miguel
Pereira
da
Costa,
Rômulo
Brasil
Filho
ServiceofOrthopedicandTraumatology,HospitaldoServidorPúblicoEstadualdeSãoPaulo(SOT/HSPE),SaoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22June2015 Accepted10August2015 Availableonline19April2016
Keywords:
Shoulderfractures/surgery Fracturefixation,internal Outcomeassessment
a
b
s
t
r
a
c
t
Objective:To correlate the functional outcomes and radiographic indices of proximal humerusfracturestreatedusingananatomicallockingplatefortheproximalhumerus.
Methods:Thirty-ninepatientswithfracturesoftheproximalhumeruswhohadbeentreated usingananatomicallockingplatewereassessedafterameanfollow-upof27months.These patientswereassessedusingtheUniversityofCaliforniaLosAngeles(UCLA)scoreandtheir rangeofmotionwasevaluatedusingthemethodoftheAmericanAcademyofOrthopedic Surgeonsontheoperatedshoulderandcomparativeradiographsonbothshoulders.The correlationbetweenradiographicmeasurementsandfunctionaloutcomeswasestablished.
Results:Wefoundthat64%oftheresultsweregoodorexcellent,accordingtotheUCLAscore, withthefollowingmeans:elevationof124◦;lateralrotationof44◦;andmedialrotationof
thumbtoT9.ThetypeoffractureaccordingtoNeer’sclassificationandthepatient’sage hadsignificantcorrelationswiththerangeofmotion,suchthatthegreaterthenumberof partsinthefractureandthegreaterthepatient’sagewere,theworsetheresultsalsowere. ElevationandUCLAscorewerefoundtopresentassociationswiththeanatomical neck-shaftangleinanteroposteriorview;fracturesfixedwithvarusdeviationsgreaterthan15◦
showedtheworstresults(p<0.001).
Conclusion: Thevariation intheneck-shaftanglemeasurementsinanteroposteriorview showedasignificantcorrelationwiththerangeofmotion;varusdeviationsgreaterthan15◦
werenotwelltolerated.Thisparametermaybeoneofthepredictorsoffunctionalresults fromproximalhumerusfracturestreatedusingalockingplate.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheGroupofShoulderandElbow,ServiceofOrthopedicandTraumatology,HospitaldoServidorPúblicoEstadual deSãoPaulo(SOT/HSPE),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.C.TenorJunior).
http://dx.doi.org/10.1016/j.rboe.2015.08.018
Tratamento
das
fraturas
do
úmero
proximal
com
placa
anatômica
bloqueada:
correlac¸ão
dos
resultados
funcionais
e
radiográficos
Palavras-chave:
Fraturasdoombro/cirurgia Fixac¸ãointernadefraturas Avaliac¸ãoderesultados
r
e
s
u
m
o
Objetivo: Correlacionarosresultadosfuncionaiseosíndicesradiográficosdasfraturasdo úmeroproximaltratadascomplacaanatômicabloqueadaparaúmeroproximal.
Métodos: Examinaram-se39pacientescomfraturasdoúmeroproximaltratadoscomplaca anatômicabloqueada,comseguimentomédiode27meses.Essespacientesforam submeti-dosàanálisedoescoredaUniversidadedaCalifórniadeLosAngeles(UCLA)eàavaliac¸ão doarcodemovimentopelométododaAcademiaAmericanadeCirurgiõesOrtopédicosno ombrooperadoeaexamesradiográficoscomparativosdeambososombros.Estabeleceu-se acorrelac¸ãoentreasmedidasradiográficaseosresultadosfuncionais.
Resultados: Obtivemos64%debonseexcelentesresultadosconformeoescoredaUCLA, commédiasde124◦deelevac¸ão;44◦derotac¸ãolateral;epolegar-T9derotac¸ãomedial.
Otipodefratura,deacordocoma classificac¸ãodeNeer,eaidadedopacientetiveram significativacorrelac¸ãocomoarcodemovimentos;quantomaioresonúmerodepartes dasfraturaseaidadedospacientes,pioresosresultados.Encontrou-seassociac¸ãoentrea elevac¸ãoeoescoredaUCLAcomoângulocervicodiafisárionaincidênciaanteroposterior;as fraturasfixadascomdesviosemvaromaioresdoque15◦apresentaramospioresresultados
(p<0,001).
Conclusão: Avariac¸ãodamedidadoângulocervicodiafisárionaincidênciaanteroposterior mostrousignificativacorrelac¸ãocomoarcodemovimento;desviosemvaromaioresdoque 15◦nãoforambemtolerados.Esseparâmetropodeserumdospreditoresdosresultados
funcionaisnasfraturasdoúmeroproximaltratadascomplacaanatômicabloqueada. ©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Proximal humeral fractures are relatively frequent; they accountfor5–10%ofallfractures.1Theirincidenceis6.6cases
forevery1000peopleeveryyears2;70%inpatientsabove60
yearsold.3Theyarethesecondmostcommonupperlimb
frac-tureandthethirdmostcommoninpatientsabove75years old.4
Themostcommonmechanismofinjuryisfallfrom stand-ingprotectedbytheextendedhand5;80%ofthesefractures
haveno displacement or are minimally displacedand sta-ble, resulting from low-energy trauma, and can be treated non-surgically6,7 withgoodprognosis. Surgicaltreatmentis
reservedforpatientswithfracturesthataredisplaced, unsta-ble, open, associated to vascular injury, or in polytrauma patients.8
Accordingtotheliterature,thereisnouniquetreatment methodthat is effective forall types ofproximal humeral fractures. The most commonly used surgical techniques are: closed reduction and fixation with pins or percuta-neousscrews,openreductionandinternalfixationwithplate andscrewsorwithtensionband,intramedullarynails,and hemiarthroplasty.2,9
Internal fixation of the proximal humerus with locking anatomic plate favors the maintenance of the reduction obtainedduringsurgery,allowingforearlierpassive mobiliza-tionandthusfacilitatingpost-operativerehabilitation.10
However,this techniqueis notfreefrom complications. Themostcommon amongthem are:limitationofrangeof
movement, avascular necrosis, loosening of the synthesis material,articularpenetrationofscrews,and/orvarusfixation ofthehumeralhead.1,11
Thisstudyaimedtoevaluatethecorrelationbetween func-tionaloutcomesandradiographicindicesofproximalhumeral fracturestreatedwithlockinganatomicalplate.
Methods
ThiswasaretrospectivestudyconductedbytheShoulderand ElbowGroupoftheOrthopedicsandTraumatologyServiceof thehospital,fromJanuary2012toMarch2013,with46patients who sufferedfracture oftheproximalhumerusand under-wentsurgicaltreatment(openreductionandinternalfixation) withlockinganatomicplate(PHILOS–Synthes®).
Thefollowingpatientswereexcluded:1individualfor pre-senting infection (re-operatedfor removalofthe synthesis material);1,fordevelopingavascularnecrosisofthehumeral head;and5duetolossoffollow-up.
Ofthe39patientsavailableforstudy,21(54%)hadafracture ontheleftsideand18(46%)ontherightside;18(46%)fractured thedominantside,and21(54%),thenon-dominant;26(67%) werefemaleand13(33%)male.Themeanagewas69years (range45–87years)forthewomenand51years(range19–71 years)forthemen.Themeanfollow-upwas27months(range 20–34months).Themostcommonmechanismofinjurywas fallfromstandingin89%ofcases.
Distribution of patients by age group and gender
100
80
60
40
Age
20
M F
Fig.1–Distributionofpatientsbyagegroupandgender.
50%,between61and77;and25%,above78.Amongthemen, 25%werebetween19and46years;50%,between47and65; and25%,above66(Fig.1).
The classification used in this study was described by Neer12in1970,basedondisplacementofthefourmain
frag-ments,which were firstly identified byCodman in 193413:
humeralhead,greatertuberosity,lessertuberosity,and diaph-ysis.AccordingtoNeer,12multiplepartsareconsideredwhen
therearedeviationsgreaterthan 1cmor 45◦ between
frag-ments.Forthegreatertuberosity,adistancegreaterthan5mm makesitadisplacedpart.
Fordiagnosisandpreoperativeclassification,X-raysinthe trueshoulderanteroposterior,scapularY,andVelpeauviews wereused,aswellasCTscanwhentherewasdoubtregarding articularinvolvement.Ofthe39studiedfractures,13(33.3%) wereclassifiedastwo-part,12asthree-part(30.8%),and14as four-part(35.9%).
Toassessthefunctionalresults,patientswithaminimum of12monthsoffollow-upwereincluded.Thedegreeof flex-ionand rotation(lateraland medial)ofbothshoulderswas measuredinaccordancetotheAmericanAcademyof Ortho-pedicSurgeons14method.TheUniversityofCaliforniainLos
Angeles(UCLA)scorewasapplied,15whichusesobjectiveand
subjectivecriteriaandassignspointsaccordingtopain,degree ofmobility,shoulderfunction,strengthandpatient satisfac-tion.Themaximumscoreis35points.
Fortheageanalysis,patientsweredividedintotwogroups: 60yearsorless(15patients–38%)andabove60(24patients– 62%),takingintoaccountLawNo.10.741oftheBrazilian Con-stitution,whichdeclaresthe ElderlyStatute,consideringas suchindividualsagedover60years.
Postoperative radiographic evaluation was standardized witha100cmdistancefromtheX-rayapparatustothefilmin theanteroposteriorincidence(AP),withcorrectionof antever-sionoftheglenoidcavityandlimbinneutralrotation;scapular Ymadewiththepatientstandingintheposteroanterior posi-tionwith45◦ anteriorlyandtheX-rayapparatustowardthe
scapula;andVelpeauviewamodification ofaxillaryprofile forpatientswithupperlimbimmobilization.16 Radiographs
werealwaysmadeonthesamedaybythesamepreviously trainedstaff,atleastoneyearaftersurgery.
α = 140º
Fig.2–Measurementofthecervicodiaphysealangle.
Theradiographicmeasurementsassessedwerethe cervi-codiaphysealangle(formedbytheintersectionbetweenaline perpendiculartotheanatomicalneckandalineparalleltothe axisofthehumeraldiaphysis),comparedtothenon-operated sideintrueshoulderanteroposteriorview1(Fig.2),and
dis-tance betweentheproximal endoftheplate andthe apex ofthegreatertuberosityonthetrueshoulderanteroposterior view(Fig.3).
Thepresenceofpseudoarthrosis,avascularnecrosis,and osteolysiswasinvestigated.
Fortheanalysisofthedifferenceofcervicodiaphysealangle inanteroposteriorincidence,avariationupto15◦ varuswas
usedasanevaluationparameter,followingthelineofthought describedbySolbergetal.17,18
Fortheanalysisofthedistancebetweentheplateandthe apexofthegreatertuberosity,patientsweredividedintotwo groups:thefirstgrouphadvalueslowerthan8mm,andthe second,valuesgreaterthanorequalto8mm.Thisparameter
7.1mm
waschosenbecauseitisthebestpositioning,accordingtothe surgicaltechniqueofosteosynthesiswithlockinganatomical platefortheproximalhumerus(PHILOS–Synthes®).
Subsequently,thecorrelationbetweenchanges in radio-graphicmeasurementsandfunctionalresultswascalculated. In the statistical analysis, the variables were presented on tables with absolute and relative frequency distribu-tion. Associations were tested using the chi-squared test, and thenormality ofthe variables wasassessed usingthe Shapiro–Wilktest.Continuousvariableswereevaluatedusing paired and unpaired Student’s t-test, ANOVA, and non-parametricMann–Whitneytest,allwith5%significancelevel. Statisticallysignificantresultswereconsideredthosewithp -valueslowerthan0.05.
Theinformationcollectedwasstoredinadatabase devel-oped in Excel® for Windows, and statistical analysis was
performedwithSTATA11SEandSPSS16.0.
Results
Functionaloutcome
Forthe39patientsanalyzed,themeanelevationofthe oper-ated limb was 123.9◦ (80–180◦), with a standard deviation
of26.4◦.Asforthecontralateralshoulder,ameanof154.1◦
(110–180◦),withastandarddeviationof19◦,wasobtained.A
meanlossof30◦ (20%)ofelevationfortheoperated
shoul-derwasobservedwhencomparedwiththecontralateral.The meanexternalrotation(ER)was44.2◦(5–80◦)fortheoperated
shoulder,withastandarddeviationof19.2◦.Forthe
contralat-eralshoulder,themeanwas62.9◦ (30–85◦),withastandard
deviationof14.4◦.Ameanexternalrotationlossof18.7◦(30%)
wasobservedfortheoperatedshoulderwhencomparedwith thecontralateral.Themeaninternalrotation(IR)was thumb-T9(T4-L5)oftheoperatedshoulderversusthumb-T7(T4-L1), themeanofthecontralateral.
IntheUCLAscore,1524(61.5%)patientshadexcellentand
good results;12 (30.8%),fair; andthree (7.7%),poor. Ofthe total,36(92.3%)patientsweresatisfiedandthree(7.7%)were unsatisfied.
Thirteenpatients (33.3%)had two-partfractures,with a mean UCLAscore15 of31.3.Compared tothe contralateral
side, the loss in range of motion was: 14.7◦ for elevation
(154.6–139.9◦);6.9◦forexternalrotation(55.8–62.7◦);and
inter-nal rotationremained atT7for operatedand contralateral shoulders.
Twelvepatients(30.8%)hadthree-partfractures,withan averageofUCLAscore15of27.6points.Comparedtothe
con-tralateral side, the loss in range of motion was: 34.6◦ for
elevation(127–161◦);21.4◦forexternalrotation(45.3–6.7◦);and
theaverageinternalrotationwentfromthumb-T9to thumb-T7inthecontralateralshoulder.
Theworstscoresinthestudywereinfour-partfractures, observedin14patients(35.9%),withmean UCLAscore15of
25.4 points.Comparedto thecontralateralside, thelossin rangeofmotionwas40.8◦ forelevation(107–147◦);,27.4◦for
externalrotation(32.4–59.8◦);andmeaninternalrotationwent
fromT10intheoperatedshouldertoT7inthecontralateral shoulder(Table1andFig.4).
Youngerpatients(60yearsorless)hadthebestresultsin theUCLAscore15(p=0.004),elevation(p<0.001),external
rota-tion(p<0.001),internalrotation(p=0.003),andvariationofthe cervicodiaphyseal angle(p=0.007)whencompared toolder patients(over60years;Table2).
Statistically significant results were observed (p<0.05) whencorrelatingtheUCLAscore15andflexionwiththeageof
thepatientandthenumberofpartsofthefractureaccording totheNeerclassification.Thehighertheageandthenumber ofparts,theworsttheflexionandUCLAscore.15
Radiographicassessment
Intheradiographicevaluation,onepatient(2.43%)had avas-cularnecrosis(thefracturehad beenclassifiedasfour-part preoperatively)andonepatient(2.43%)presentedinfection(it wasnecessarytoremovethesynthesismaterial).Itwasnot possibletoassessthepre-establishedstudymeasurementsfor thesetwopatients.
Of the 39 patients studied, the mean cervicodiaphyseal angleinanteroposteriorviewwas:129◦ontheoperatedside
(range:82–170◦;standarddeviation:19◦)and140◦inthe
con-tralateralshoulder(range:124–153◦;standarddeviation:6.9◦).
Thegreatestdifferenceswereobservedinfour-partfractures, especificallyintheanteroposteriorview,whichshoweda dif-ferenceof21◦whencomparedtothenon-operatedside.
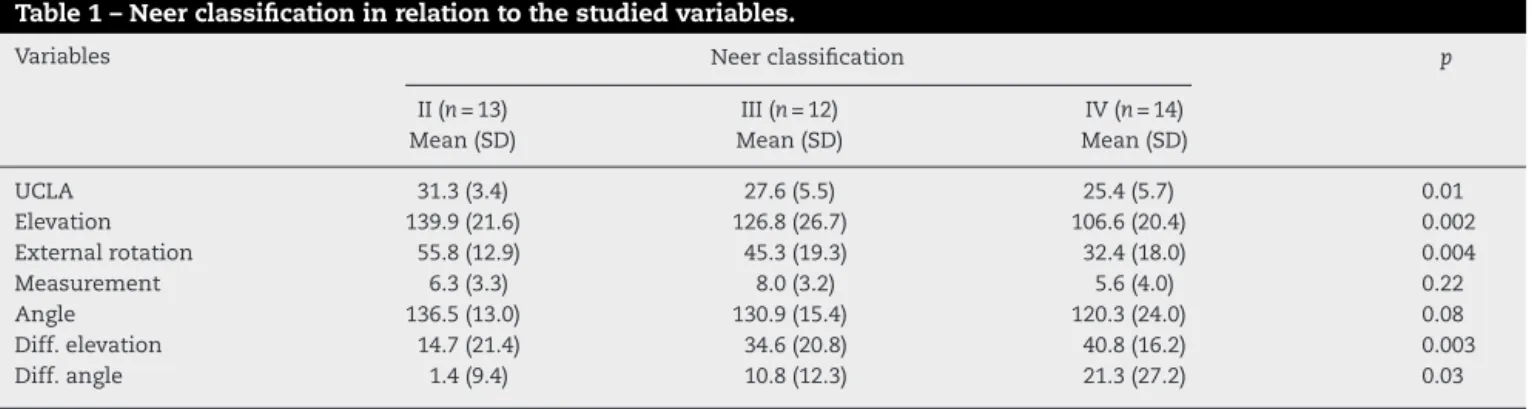
Table1–Neerclassificationinrelationtothestudiedvariables.
Variables Neerclassification p
II(n=13) III(n=12) IV(n=14)
Mean(SD) Mean(SD) Mean(SD)
UCLA 31.3(3.4) 27.6(5.5) 25.4(5.7) 0.01
Elevation 139.9(21.6) 126.8(26.7) 106.6(20.4) 0.002
Externalrotation 55.8(12.9) 45.3(19.3) 32.4(18.0) 0.004
Measurement 6.3(3.3) 8.0(3.2) 5.6(4.0) 0.22
Angle 136.5(13.0) 130.9(15.4) 120.3(24.0) 0.08
Diff.elevation 14.7(21.4) 34.6(20.8) 40.8(16.2) 0.003
Diff.angle 1.4(9.4) 10.8(12.3) 21.3(27.2) 0.03
Measurement,measurementfromthetipoftheplatetotheTMapex(mm);Angle,cervicodiaphysealangleinanteroposteriorincidence;Diff.
ele-vation,differenceinelevationintheaffectedshoulderwhencomparedtothecontralateralshoulder;Diff.angle,differenceincervicodiaphyseal
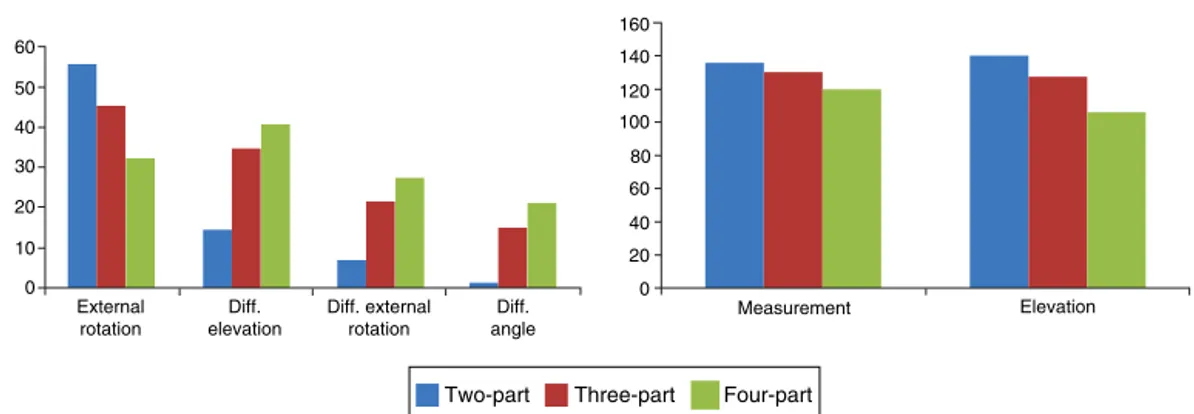
Comparison of the variables according to the Neer classification
60 50 40 30 20 10 0
160 140 120 100 80 60 40 20 0 External
rotation
Diff. elevation
Diff. external rotation
Diff. angle
Measurement
Two-part Three-part Four-part
Elevation
Fig.4–ComparisonofthevariablesaccordingtotheNeerclassification.
Table2–Ageinrelationtothestudiedvariables.
Variables Age p
≤60years(n=15) >60years(n=24)
Mean(SD) Mean(SD)
UCLA 31.1(3.1) 26.1(5.8) 0.004
Elevation 146.9(19.0) 109.6(19.3) <0.001
Externalrotation 58.7(13.6) 35.1(16.5) <0.001
Internalrotation T7 T10 0.003
Plateheightatthegreatertuberosity 7.4(2.9) 6.1(4.0) 0.27
Angle 135.1(11.5) 125.2(22.1) 0.12
Diff.elevation 22.7(23.3) 34.9(20.4) 0.09
Diff.externalrotation 13(14.5) 22.3(16.0) 0.08
Diff.angle 4.4(9.5) 15.8(23.4) 0.007
Angle,cervicodiaphysealangleinanteroposteriorincidence;Diff.elevation,differenceinelevationintheaffectedshoulderwhencompared
tothecontralateralshoulder;Diff.angle,differenceincervicodiaphysealangleintheaffectedshoulderwhencomparedtothecontralateral
shoulder.
Patientswhohadlessthan15◦variationinthe
cervicodia-physealanglemeasurementinanteroposteriorviewbetween theoperatedshoulderandthecontralateralhadbetter func-tionaloutcomes:betterUCLAscore15(p<0.001),higherflexion
(p<0.001),betterexternalrotation(p<0.001),andbetter inter-nalrotation(p=0.03;Table3).
Correlationwasobservedbetweencervicodiaphysealangle measurement in anteroposterior incidence and elevation (p=0.009)andUCLAscore15(p=0.005).
Table3–Differenceinthecervicodiaphysealanglein relationtothestudiedvariables.
Variables Differenceinthe
cervicodiaphysealanglein
anteroposteriorincidence
p
<15◦ ≥15◦
Mean(SD) Mean(SD)
UCLA 30.3(3.2) 25.2(6.2) <0.001
Elevation 139.2(22.6) 108.7(20.7) <0.001
Externalrotation 51.0(15.6) 31.7(16.1) <0.001
Internalrotation T8 T10 0.03
Plateheightat
thegreater
tuberosity
7.02(3.2) 5.4(4.1) 0.23
Whenmeasuringthedistancebetweentheproximalend oftheplateand theapexofthe greatertuberosity,amean of6.6mm(range:0–14mm;standarddeviation:3.6mm)was obtained.
ThecomparisonsamongtheresultsoftheUCLAscore,15
elevation, external rotation, and cervicodiaphyseal angle between the two groups were not significant in any case (Table4).
Correlationbetweenradiographicandfunctionaloutcomes
Theworstfunctionaloutcomeswereobservedincaseswhere the difference betweentheoperated and contralateralside was greater thanor equalto15◦ varusinthe
anteroposte-rior incidence.Insuchcases,the patientshad lowermean flexion(108.7◦)andworseUCLAscore15(25.2).Patientswho
hadvariationslowerthan15◦hadmeanflexionof139.2◦and
mean UCLAscore15 of30.3.These resultswerestatistically
significantinthepresentstudy(Table4).
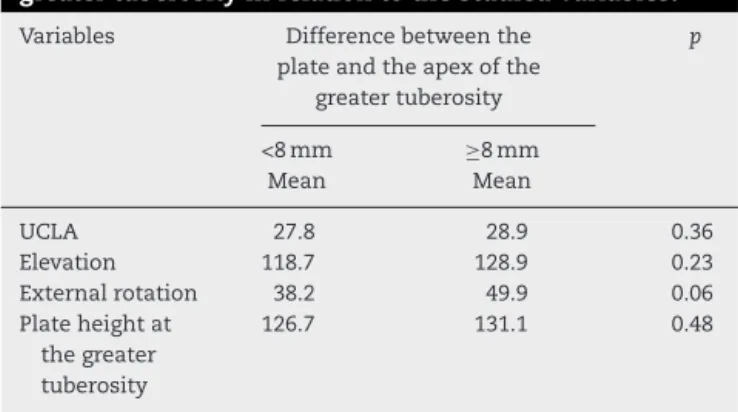
Table4–Distancefromtheplatetotheapexofthe greatertuberosityinrelationtothestudiedvariables.
Variables Differencebetweenthe
plateandtheapexofthe
greatertuberosity
p
<8mm ≥8mm
Mean Mean
UCLA 27.8 28.9 0.36
Elevation 118.7 128.9 0.23
Externalrotation 38.2 49.9 0.06
Plateheightat
thegreater
tuberosity
126.7 131.1 0.48
Measurement, measurement from the tip of the plate to the
TMapex(mm);Angle,cervicodiaphysealangleinanteroposterior
incidence.
groups,thefirstpresentedmeanflexionof118.7◦andthe
sec-ondof128.9◦.Therewasnostatisticallysignificantdifference
betweenbothgroups(Table4).
Discussion
Inthepresentstudy,itwasobservedthatdeviationsgreater than15◦varusrelativetocontralateralshoulderin
anteropos-teriorviewarenotwelltoleratedbythepatientandleadto withflexionlossandaworseUCLAscore.15
Solberg et al.17,18 reached asimilar conclusion. In their
study, the authors divided the results according to the obtained alignment relative to the contralateral shoulder. They considered less than 5◦ of varus angulation of the
humeral head as a good reduction. In turn, a satisfactory reductionrangedfrom5◦ and20◦ ofvarusdeformityofthe
humeralhead.Theauthorsconcludedthatpatientswithgood orsatisfactoryreductionshadbetteroutcomesthanpatients withvarusdeformitygreaterthan20◦,whopresentedflexion
lossandworsefunctionaloutcome.
Resch,19 in a 2011 reviewarticle, also considered these
parameters to be important, and proposed a classification based on varus and valgus deviations. Brunner et al.20
observedinferiorresultswhenthereductionofthefracture hadcervicodiaphysealanglewithanincreasedvarus; how-ever,theirresultswerenotstatisticallysignificant.Robinson et al.21 observed that severely displaced fractures tend to
increasevarusdeformityandrecommendedosteosynthesis withtheuseoflockingplatesinpatientswith cervicodiaphy-sealanglesmallerthan100◦.
The surgical technique of osteosynthesis with lock-ing anatomical plate for the proximal humerus (PHILOS – Synthes®)determinesthatthedistancefromtheplatein
rela-tion tothe apexofthe greater tuberosity shouldbe 8mm, sincelowerdistanceswouldcausesubacromialimpingement, andabductionandflexiondeficitsintheshoulder.21,22Inthe
presentstudy,asmall difference,withoutstatistical signifi-cance,wasobservedinfunctionaloutcomeamongpatients, regardlessofthedistancebetweentheproximalendofthe plateandtheapexofthegreatertuberosity.
Inthefunctionalevaluation,threepatientswerenot sat-isfiedwiththetreatment,andtheirresultswereconsidered aspoor(accordingtotheUCLAscore15).Oneofthesecases
(2.43%)hadosteolysisofthegreatertuberosity.Onecaseof avascularnecrosis(2.43%)wasobserved,andwasalso con-sideredpooraccordingtotheUCLAscore.15Brunneretal.20
reportedahighernumber,with8%necrosisinamulticenter study of158fractures.Accordingtotheliterature,the inci-denceofosteonecrosisforproximalhumerusfractureranges from4%to16%.23Patientswithavascularnecrosispresentthe
worstfunctionalresults.However,elderlypatients,whohave lowerfunctionaldemand,toleratethiscomplicationbetter.24
The 61.5% excellent and good results observed in the present studyare belowlevelsreportedintheliterature.In 2011,Hirschmannetal.25publishedastudywith64patients
withaminimumfollow-upoffouryears,treatedwithlocking plate,andreported75%excellentandgoodresults.Theyalso concludedthattheseresultscontinuedtoimproveevenone yearafterthesurgery.Roseetal.26 found75%consolidation
andexcellentresults.
Inthepresentstudy,thehighertheageofthepatientand the number ofparts of the fracture, the worst the flexion and the UCLA score.15 These results were statistically
sig-nificantp<0.001,p=0.02,p=0.008,andp=0.01,respectively). Yangetal.27foundthatthehighernumberoffractureparts
and the lackof medialsupport(calcarcomminution) were determinersofthefunctionaloutcome.Koukakisetal.28also
hadworseoutcomesrelatedtoage.
In the present study, the cervicodiaphyseal angle was usedasacomparativeradiographicparameterwiththe con-tralateralshoulderforcorrelationwithfunctionaloutcomes. However,thereisnouniversalstandardizedmethodto mea-surethisangle.29Otherbiasesintheresultsofthisstudywhich
werenotanalyzedaretheco-morbiditiesofpatients,priorand latepostoperativeintegrityoftherotatorcuff,andtheuse(or not)ofmedialsupportscrewsinlockingplates.30–33 Further
studieswithgreateremphasisonsuchfactorsareneededto complementthepresentfindings.
Conclusion
Thisstudyindicatedthatthealterationofthe cervicodiaphy-sealangleinanteroposteriorviewwassignificantlycorrelated with the range of motion; displacements greater than 15◦
varus were notwelltolerated. Thisradiographicparameter canbeoneofthepredictorsoffunctionalresultsinfractures oftheproximalhumerustreatedwithlockingplates.
Thegreatertheageofthepatientandthenumberofparts ofthefracture,theworsethefunctionaloutcomesare.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
fracturestreatedwithlockingplates.JOrthopTrauma. 2007;21(10):676–81.
2. LantingB,MacDermidJ,DrosdowechD,FaberKJ.Proximal humerusfractures:asystematicreviewoftreatment modalities.JShoulderElbowSurg.2008;17(1):42–54.
3. SüdkampN,BayerJ,HeppP,VoigtC,OesternH,KääbM,etal. Openreductionandinternalfixationofproximalhumeral fractureswithuseofthelockingproximalhumerusplate. Resultsofaprospective,multicenter,observationalstudy.J BoneJointSurgAm.2009;91(6):1320–8.
4. Court-BrownCM,CaesarB.Epidemiologyofadultfractures:a review.Injury.2006;37(8):691–7.
5. ThanasasC,KontakisG,AngoulesA,LimbD,GiannoudisP. Treatmentofproximalhumerusfractureswithlockingplates: asystematicreview.JShoulderElbowSurg.2009;18(6): 837–44.
6. EgolKA,OngCC,WalshM,JazrawiLM,TejwaniNC.Early complicationsinproximalhumerusfracturestreatedwith lockedplates.JOrthopTrauma.2008;22(3):159–64.
7. CohenM,AmaralMV,MonteiroM,BrandãoBL,MottaFilho GR.Osteossíntesedasfraturasdaextremidadeproximaldo úmerocomsistemadeplacadeângulofixocomparafusos bloqueados:técnicaeresultados.RevBrasOrtop.
2009;44(2):106–11.
8. TenorJuniorAC,RibeiroFR,BrasilFilhoR,FilardiFilhoCSF, CostaGL,MennitiEL.Avaliac¸ãodotratamentocirúrgicodas fraturasemduasoutrêspartesdoúmeroproximalcomo SistemaParaquedas.VerBrasOrtop.2010;45(3):241–6.
9. MonteiroGC,EjnismanB,AndreoliCV,PochiniAC,OlympioE. Resultadosdotratamentodasfraturasdoterc¸oproximaldo úmerocomplacasdebloqueio.ActaOrtopBras.
2011;19(2):69–73.
10.HirschmannMT,QuarzV,AudigéL,LudinD,MessmerP, RegazzoniP,etal.Internalfixationofunstableproximal humerusfractureswithananatomicallypreshaped interlockingplate:aclinicalandradiologicevaluation.J Trauma.2007;63(6):1314–23.
11.OwsleyKC,GorczycaJT.Fracturedisplacementandscrewcut outafteropenreductionandlockedplatefixationofproximal humeralfractures.JBoneJointSurgAm.2008;90(2):233–40.
12.NeerCS2nd.Displacedproximalhumeralfractures:PartI. Classificationandevaluation.1970.ClinOrthopRelatRes. 2006;442:77–82.
13.CodmanEA.Fracturesinrelationtothesubacromialbursa. In:CodmanEA,editor.Theshoulder.Ruptureofthe supraspinatustendonandotherlesionsinoraboutthe subacromialbursa.Boston:ThomasTodd;1934.p.313–33.
14.HawkinsRJ,BokorDJ.Clinicalevaluationofshoulder problems.In:RockwoodCA,MatsenFA,editors.Theshoulder. 2ed.SaintLouis:W.B.Saunders;1998.p.164–98.
15.AmstutzHC,SewHoyAL,ClarkeIC.UCLAanatomictotal shoulderarthroplasty.ClinOrthopRelatRes.1981;155:7–20.
16.DoneuxPS,ChecchiaSL,MiyazakiAN.Padronizac¸ãodo estudoradiográficodacinturaescapular.RevBrasOrtop. 1998;33(11):883–8.
17.SolbergBD,MoonCN,FrancoDP,PaiementGD.Surgical treatmentofthreeandfour-partproximalhumeralfractures. JBoneJointSurgAm.2009;91(7):1689–97.
18.SolbergBD,MoonCN,FrancoDP,PaiementGD.Lockedplating of3-and4-partproximalhumerusfracturesinolderpatients: theeffectofinitialfracturepatternonoutcome.JOrthop Trauma.2009;23(2):113–9.
19.ReschH.Proximalhumeralfractures:currentcontroversies.J ShoulderElbowSurg.2011;20(5):827–32.
20.BrunnerF,SommerC,BahrsC,HeuwinkelR,HafnerC, RillmannP,etal.Openreductionandinternalfixationof proximalhumerusfracturesusingaproximalhumerallocked plate:aprospectivemulticenteranalysis.JOrthopTrauma. 2009;23(3):163–72.
21.RobinsonCM,WylieJR,RayAG,DempsterNJ,OlabiB,Seah KT,etal.Proximalhumeralfractureswithaseverevarus deformitytreatedbyfixationwithalockingplate.JBoneJoint SurgBr.2010;92(5):672–8.
22.PaavolainenP,BjörkenheimJM,SlätisP,PaukkuP.Operative treatmentofsevereproximalhumeralfractures.ActaOrthop Scand.1983;54(3):374–9.
23.OngC,BechtelC,WalshM,ZuckermanJD,EgolKA. Three-andfour-partfractureshavepoorerfunctionthanone-part proximalhumerusfractures.ClinOrthopRelatRes. 2011;469(12):3292–9.
24.WijgmanAJ,RoolkerW,PattTW,RaaymakersEL,MartiRK. Openreductionandinternalfixationofthreeandfour-part fracturesoftheproximalpartofthehumerus.JBoneJoint SurgAm.2002;84(11):1919–26.
25.HirschmannMT,FalleggerB,AmslerF,RegazzoniP,GrossT. Clinicallonger-termresultsafterinternalfixationofproximal humerusfractureswithalockingcompressionplate
(PHILOS).JOrthopTrauma.2011;25(5):286–93.
26.RosePS,AdamsCR,TorchiaME,JacofskyDJ,HaidukewychGG, SteinmannSP.Lockingplatefixationforproximalhumeral fractures:initialresultswithanewimplant.JShoulderElbow Surg.2007;16(2):202–7.
27.YangH,LiZ,ZhouF,WangD,ZhongB.Aprospectiveclinical studyofproximalhumerusfracturestreatedwithalocking proximalhumerusplate.JOrthopTrauma.2011;25(1):11–7.
28.KoukakisA,ApostolouCD,TanejaT,KorresDS,AminiA. FixationofproximalhumerusfracturesusingthePhilosplate: earlyexperience.ClinOrthopRelatRes.2006;442:115–20.
29.JeongJ,BryanJ,IanottiJP.Effectofavariableprosthetic neck-shaftangleandthesurgicaltechniqueonreplicationof normalhumeralanatomy.JBoneJointSurgAm.
2009;91(8):1932–41.
30.GardnerMJ,WeilY,BarkerJU,KellyBT,HelfetDL,LorichDG. Theimportanceofmedialsupportinlockedplatingof proximalhumerusfractures.JOrthopTrauma. 2007;21(3):185–91.
31.RobinsonCM,LonginoD,MurrayIR,DuckworthAD.Proximal humerusfractureswithvalgusdeformityofthehumeral head:thespectrumofinjury,clinicalassessmentand treatment.JShoulderElbowSurg.2010;19(7):1105–14.
32.RobinsonCM,PageRS.Severelyimpactedvalgusproximal humeralfractures:resultsofoperativetreatment.JBoneJoint SurgAm.2003;85(9):1647–55.