REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiology www.sba.com.brSCIENTIFIC
ARTICLE
Low-dose
levobupivacaine
plus
fentanyl
combination
for
spinal
anesthesia
in
anorectal
surgery
Mehtap
Honca
a,∗,
Necla
Dereli
a,
Emine
Arzu
Kose
b,
Tevfik
Honca
c,
Selcen
Kutuk
a,
Selma
Savas
Unal
a,
Eyup
Horasanli
aaDepartmentofAnesthesiologyandReanimation,KeciorenTrainingandResearchHospital,Ankara,Turkey
bDepartmentofAnesthesiologyandReanimation,IstanbulMedipolUniversity,MedipolMegaHospital,Istanbul,Turkey cDepartmentofMedicalBiochemistry,GulhaneMilitaryMedicalAcademy,Ankara,Turkey
Received19November2013;accepted15January2014
Availableonline20February2014
KEYWORDS
Hyperbaric levobupivacaine; Fentanyl; Spinal;
Anorectalsurgery
Abstract
Background: theaimofthisstudywastoinvestigatetheeffectsofspinalanesthesiausingtwo differentdosesoffentanylcombinedwithlow-doselevobupivacaineinanorectalsurgery. Methods:inthis prospective,double-blindstudy,52 American Society ofAnaesthesiologists I---IIpatientsscheduledforelectiveanorectalsurgerywererandomizedintotwogroups.The patientsingroupIreceivedintrathecal2.5mghyperbariclevobupivacaineplus12.5gfentanyl andingroupIIreceivedintrathecal2.5mghyperbariclevobupivacaineplus25gfentanyl.All thepatientsremainedintheseatedpositionfor5minaftercompletionofthespinalanesthesia. Sensoryblockwasevaluatedwithpin-pricktestandmotorblockwasevaluatedwithamodified Bromagescale.
Results:motorblockwasnotobservedinbothofthegroups.Thesensoryblockwaslimited totheS2levelingroupI,andS1levelingroup II.Noneofthepatients requiredadditional analgesicsduringtheoperation.Timetotwo-segmentregressionwasshorteringroupI com-paredwithgroupII(p<0.01).OnepatientingroupIand5patients ingroupIIhadpruritus. Hemodynamicparameterswerestableduringtheoperationinbothofthegroups.
Conclusion: spinalsaddleblockusinghyperbariclevobupivacainewithboth12.5gand25g fentanylprovidedgoodqualityofanesthesiawithoutmotorblockforanorectalsurgeryinthe proneposition.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](M.Honca).
0104-0014/$–seefrontmatter©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Levobupivacaína; Fentanil; Raquianestesia; Cirurgiacolorretal
Combinac¸ãodelevobupivacaínaemdosebaixaefentanilpararaquianestesiaem
cirurgiaanorretal
Resumo
Justificativa:Oobjetivo deste estudofoi investigar osefeitos daraquianestesia comouso deduasdosesdiferentesdefentanilem combinac¸ãocomdosebaixadelevobupivacaína em cirurgiaanorretal.
Métodos: Nesteestudoprospectivoeduplo-cego,52pacientescomestadofísicoASAI-II, pro-gramadosparacirurgiaeletivaanorretal,foramrandomicamentealocadosemdoisgrupos.Os pacientesdoGrupoIreceberam2,5mgdelevobupivacaínahiperbáricamais12,5gdefentanil porviaintratecaleosdoGrupoIIreceberam2,5mgdelevobupivacaínahiperbáricamais25g defentanilporviaintratecal.Todospermaneceramemposic¸ãosentadaporcincominutosapós otérminodaraquianestesia.Obloqueiosensorialfoiavaliadocomotestedapicadadeagulha eobloqueiomotorcomaescalamodificadadeBromage.
Resultados: Obloqueiomotor não foiobservado em ambosos grupos.O bloqueiosensorial limitou-seaonívelS2noGrupoIeS1noGrupoII.Nenhumdospacientesprecisoudeanalgésico suplementarduranteaoperac¸ão.OtempoderegressãodedoisseguimentosfoimenornoGrupo Iemcomparac¸ãocomoGrupoII(p<0,01).UmpacientedoGrupoIecincodoGrupoII apresen-taramprurido.Osparâmetroshemodinâmicospermaneceramestáveisduranteacirurgia em ambososgrupos.
Conclusão:Obloqueioespinhalemselacomousodelevobupivacaínahiperbárica,tantocom 12,5gquanto com25gdefentanil,proporcionaboaqualidadedeanestesiasembloqueio motorparacirurgiaanorretalemdecúbitoventral.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Spinalanesthesiaforanorectalsurgeryisapopularand com-monlyusedmethodcharacterizedbyrapidonsetandoffset, easymobilizationandshorthospitalstory.1
Levobupivacaine hydrochloride is the pure S(-)-enantiomer of racemic bupivacaine with less effects to cardiovascular and central nervous system than bupivacaine.2Bothhyperbariclevobupivacaineandisobaric levobupivacaine have been used in anorectal surgery.3---5 Howevertherearenotenoughdatayet,whetheroneform issuperiortotheother.Hyperbariclocalanestheticsusedin spinalsaddleblockinthepronepositionhavesome disad-vantages.Patientsarerecommendedtostay inthesitting positionforseveralminutesafterintrathecaladministration topreventtheoccurrenceofhypotension. Alsohyperbaric localanestheticsolutionsmightcausehighlevelsofspinal anesthesia.6,7 The sideeffects can be reducedwith using lowdosesoflocalanesthetics. Adjuvants suchasfentanyl andsufentanilpotentiatetheafferentsensoryblockadeand facilitatereductionsinthedoseoflocalanesthetics.8 The aimofthisprospective,double-blind,randomizedtrialwas tocomparethedifferencesinsensoryandmotorblockade, patient and surgeon satisfaction and complications of intrathecal2.5mghyperbariclevobupivacaineplus12.5g
fentanylwithintrathecal2.5mghyperbariclevobupivacaine plus25gfentanyl.
Materials
and
methods
After approval from the Hospitals Ethics Committee and obtainingpatients’writteninformedconsent,52patients, aged>18years,withAmericanSocietyofAnaesthesiologists
(ASA) physical status I and II scheduled for ambulatory anorectalsurgery,wereincludedinthisstudy.
Patients were randomized into two groups using a computer-generated randomization sequence with sealed envelopes. Patients with abnormal coagulation profiles, severecardiopulmonarydisease,diabetes,peripheral neu-ropathy,infectionattheinjectionsite,markedscoliosis,and patientsreceivingchronicanalgesictherapywereexcluded from the study. None of the patients received premedi-cation. Patients were monitored with electrocardiogram, noninvasive arterial blood pressure and pulseoximetry in theoperatingroom.A20-Gcannulawasinsertedatthe dor-sumofthelefthandand8mL/kg/hof0.9%sodiumchloride infusionwasestablished1hbeforeinitiationoftheregional block.GroupI(n=26)received2.5mghyperbaric levobupi-vacaine 0.5% (5mg/mL, Chirocaine, Abbott Laboratories, NorthChicago,IL,USA)plus12.5gfentanylwhereasGroup
IIreceived(n=26)2.5mghyperbariclevobupivacaine0.5% (5mgml,Chirocaine, Abbott Laboratories,North Chicago, IL,USA)plus25gfentanyl.Bothofthesolutionswere
Sen-soryblockwasevaluatedbythepin-prickmethodatevery 2min until the sufficient block reached the S4 level and testing wasconductedat every5minuntilthe endof the operation. After sitting for 5min patients wereplaced in theproneposition.Motorblockwasevaluatedaccordingto a modified Bromage scale (0:nomotor block, 1:inability toraise extended legs, 2: inability toflex knees, able to movefeet,3:inabilitytoflexankle points).Onsettimeof S4levelsensoryblock(timetoreadinessforsurgery), max-imumlevelofsensoryblock,timeto2segmentregression, time tourination andtime tofirst analgesic requirement wereevaluatedbyanobserverblindedtothestudygroups andrecorded.Postoperativesideeffectslikenausea, vomi-ting,headacheandprurituswererecordedbynursingstaff. Diclofenac sodium 75mg intramuscular (IM) was used for rescue analgesiaandfirstanalgesiarequirementtimewas recorded.Hypotensionwasdefinedasadecreaseinsystolic arterial blood pressure>20% of baseline and was treated with intravenous (IV) 5---10mg bolus doses of ephedrine. Bradycardiawasdefinedasheartrate<60beatperminute andwastreated with0.01mg/kg bolus dosesof atropine. After completion of the surgery, patients were asked to rate the quality of their anesthesia using a 4 point scale (1:Perfect,2:Satisfactory,comfortablebut somefeelings ofpressureortraction,3:Poor,discomfortbecauseof feel-ingintensepressureortraction,4:Worst:Majordiscomfort becauseofpain).
ThestatisticalanalysiswasperformedusingSPSSfor Win-dowsversion10.0.1.Thesamplesizewascalculated,based on80%power,tobeabletodetecta25min(min)difference in mean timeto sensory block recovery.Pre-study power analysisusingourpopulationmeanandstandarddeviation suggestedthat24patientsineachgroupwouldbesufficient todetectadifferenceof25minassumingatypeIerrorof5%. Datawerepresentedasmean±standarddeviation,median (minimum---maximum) or frequencies as appropriate. Stu-dent’st-testwasperformedforanalysisoftheparametric dataandMann---WhitneyUtestwasperformedforanalysis ofthenon-parametricdata.Resultswereconsidered statis-ticallysignificantifp<0.05.
Results
Fifty-twopatientswereenrolledinthestudy.Nosignificant differencewasobservedbetween thegroups withrespect to gender, age, height, weight, ASA physical status, and duration of the operation (Table 1). The maximum sen-soryblock level reached toS1 dermatome in both of the groups. The median upper limit of the sensory block was S2in Group II and S1 in Group I preoperatively. Time to reachS4dermatomewassimilarbetweenthegroups. Pre-operativeandpostoperativemaximumblockeddermatomes inboth ofthe groups aregivenin Table2.Mean times to
Table1 Patientcharacteristics,operationtime,typeofsurgicalprocedure.
GroupI(n=26) GroupII(n=26) p
Age(years) 24±8 30±10 0.061
Height(cm) 173±8 175±8 0.94
Weight(kg) 81±17 82±14 0.346
Gender(female/male) 3/23 4/22 0.687
Durationofsurgery(min) 21±7 36±12 0.233
Surgicalprocedure(n)
Pilonidalsinusexcision 22 21 0.021
Hemorrhoidectomy 2 3
Analfissure 2 2
Dataareexpressedasmeanvalues±SD.
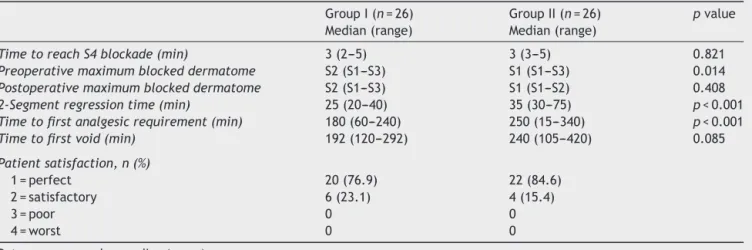
Table2 Spinalblockcharacteristics,timetofirstvoidingofurine,analgesicrequirementandpatientsatisfaction.
GroupI(n=26) Median(range)
GroupII(n=26) Median(range)
pvalue
TimetoreachS4blockade(min) 3(2---5) 3(3---5) 0.821 Preoperativemaximumblockeddermatome S2(S1---S3) S1(S1---S3) 0.014 Postoperativemaximumblockeddermatome S2(S1---S3) S1(S1---S2) 0.408 2-Segmentregressiontime(min) 25(20---40) 35(30---75) p<0.001 Timetofirstanalgesicrequirement(min) 180(60---240) 250(15---340) p<0.001 Timetofirstvoid(min) 192(120---292) 240(105---420) 0.085
Patientsatisfaction,n(%)
1=perfect 20(76.9) 22(84.6)
2=satisfactory 6(23.1) 4(15.4)
3=poor 0 0
4=worst 0 0
two-segmentregressionwereshorteringroupIthangroup II(p<0.001). Allpatientsin both ofthegroups wereable topositionthemselveswithBromagescores0.Timeto void-ingwassimilarinbothofthegroups(p=0.085),andnoneof thepatientsneededcatheterization.Firstanalgesic require-ment timewasshorter in group Icompared withgroup II (p<0.001).Noneofthepatientsneededsupplemental anal-gesicduringtheoperation.Patientssatisfactionweresimilar inbothofthegroups, and76.9%ofthepatientsingroupI and84%ofthepatientsingroupIIassessedtheanesthetic qualityas ‘perfect’ (Table 2).The adverse effects during theintraoperativeandpostoperativeperiod;nausea vomi-ting andpruritus were similarin both of thegroups. One patientingroupIandfivepatientsingroupIIreceived treat-mentforthepruritus(p=0.086).Therewerenosignificant differences between the groups regarding mean arterial bloodpressureandheartratevalues,beforeandduringthe surgery.
Discussion
Levobupivacaine,thepureS(-)-enantiomerofbupivacaine, wasdemonstrated lessaffinityand strengthof depressant effectsonto myocardial and central nervoussystem com-paredwithbupivacaine.Additionally,producingdifferential neuraxialblockpreservingmotorfunctionatlow concentra-tionsprovidesanadvantagetolevobupivacaine.9Adjuvants suchas fentanyl and sufentanyl reduce the dose of local anestheticsandprolongthesensoryblockwithoutdelaying timetovoid.The recommended intrathecal dosesof fen-tanylasadjuvanttolocalanestheticsis10---25g.10,11 Also
theseadjuvantsimprovetolerancetovisceralsensationslike bladder distensionand peritoneal stretch. However adju-vantssuchasfentanyltolocalanestheticsdoesnotprolong thedurationofmotorblockade.10,11So,twodifferentdoses offentanylcombinedwithlow-doselevobupivacainewere usedinthisstudy.Bothoftheanestheticcombinations pro-videdgoodqualityofspinalanesthesiawithoutmotorblock. Cuvas etal.5 compared 5mg0.5% plainbupivacaine in 1mLvolumewith5mg0.5%plainlevobupivacaine in1mL volumefor pilonidal cyst/sinussurgery in the prone posi-tion.Theyfoundsimilarresultswithregardtosensoryand motor blockade in both of the groups. The median maxi-mumlevelofsensoryblock reachedtoT10dermatome in thelevobupivacainegroup.Allthepatientsinthe levobupi-vacainegrouphad motorblockade equivalenttoBromage score1or2.Patientsatisfactionwas92%inthe levobupi-vacainegroup. Inthe present study,we used2.5mg dose ofhyperbaric levobupivacainewithtwodifferentdosesof fentanyl.Wealsofoundsimilarresultsforthetimeofonset ofthesensoryblockinthetwogroupsandmotorblockwas notobservedinanyofthepatients.Weusedsmalldoseof levobupivacainethan Cuvas etal.usedin their studyand maximumsensoryblock waslimitedtotheS1dermatome inbothofthegroups.Thesensoryblocklevelwassufficient for anorectal surgeryand allthe patients expressedtheir anestheticsatisfactionasgoodorverygood.
Erbay et al.12 compared the effects of spinal anes-thesia provided by 7.5mg hyperbaric bupivacaine plus 25gfentanylwith7.5mghyperbariclevobupivacaineplus
25g fentanyl for transurethral surgery. They found that
hyperbaric levobupivacaineplus25gfentanylprovideda
shorter motorblock timeandalonger sensoryblocktime than7.5mghyperbaricbupivacaineplus25gfentanyl.In
another study, Girgin et al.13 suggested that intrathecal administrationof25gfentanyladdedto5mg
levobupiva-caine0.5%foringuinalherniorrhaphyincreasedthequality ofspinalanesthesiaandallowedtouseasub-anesthetic lev-obupivacainedose.Inthepresentstudy,levobupivacainein combination with25gfentanyl providedasensory block
withlonger duration than the hyperbaric levobupivacaine in combination with 12.5g fentanyl. Also first analgesic
requirementtimewassignificantlylongerinthespinal anes-thesia group provided by hyperbaric levobupivacaine plus 25gfentanyl.Assimilartoother studies,combining
fen-tanylwithlevobupivacaineprolongedsensoryblockwithout affectingmotorrecoveryortimetovoid.10,11
Hyperbariclocalanestheticsolutionshaveahigher den-sity compared with CSF. Forthis reason, hyperbaric local anesthetic solutionstend tomove inacephaled direction andmayproducemotorblockadeintheanteriorrootsofthe thoracicregionintheproneposition.6,7Ithasbeenshown that usingsmall dosesof local anesthetics withadequate basicityandappropriatepatientpositioning,onlythenerve roots supplying a specific area is affected.6,7 Also admin-istrationof localanesthetics withahigh speedaffectsits distributionoflevobupivacainetothevertexpositioninthe thecal cavity and causes hemodynamic changes.14 In this studyweusedhyperbaricsolutionsoflevobupivacaineand measuredthedensitiesofthesolutionsat37◦C.Local anes-thetics were administered at a rateof 1mL/60s in order tominimizethedistributionofhyperbariclevobupivacaine dependingontheconversionofpatientposturefromsitting positiontoproneposition.Motorblockadewasnotobserved inbothofthestudygroups.Noclinicallysignificant hemo-dynamicchangessuchasbradycardiaortreatmentrequiring hypotensionoccurredinanyofthepatients.
The minimal recommended dose of spinal hyperbaric bupivacaineis4---5mgforanorectalsurgery.15.Gurbetetal.3 compared 5mg 0.5% spinal hyperbaric bupivacaine and 2.5mg 0.5%hyperbaric bupivacaine plus 25gfentanyl in
outpatientanorectal surgery. They found that addition of 25g fentanyl to 2.5mg 0.5% bupivacaine prolonged the
duration of sensory blockade and reduced postoperative analgesic requirement. Upper limit of the sensory block reached to T9 (T4-L1) dermatome and median maximum motor blockade score was 21---3 in hyperbaric bupivacaine plusfentanylgroup.Weused2.5mgofhyperbaric levobupi-vacaine0.5%withtwodifferentfentanylcombinationsfor spinal anesthesia in anorectal surgery. The median upper limit of thesensoryblock wasS1in the spinalanesthesia group provided by hyperbaric levobupivacaine plus 25g
fentanyl.MediantimetoS4sensoryblockadewas3minand motorblockadewasnotobservedintheanyofthepatients. Bradycardia or hypotension was not observed during the surgery.Wesuggestthat2.5mghyperbariclevobupivacaine with25gfentanylcanbepreferredforspinalanesthesiain
anorectalsurgerywithhighriskpatientsbecauseofbetter hemodynamicstabilityandwithoutdelayininitiationofthe surgery.
concluded that spinal perianal block produced by 1.5mg bupivacaineprovidedasignificantlyrestrictedsensoryblock levels (median maximum=S4), and motor block was not observedinanyofthepatientinthisgroupcomparedwith the groupwhich was6mg bupivacaine used.Alsotimeto ambulationandvoidingwereshorterinthelowdose bupi-vacainegroup.Theyconcludedthat,maintainingtheseated positionisessentialforrestrictionofblockadetothemost caudalspinalnerverootswhichsupplytheperianalarea.15 Inanotherstudy,Kazaketal.comparedtheefficacyofspinal 1.5mghyperbariclevobupivacainewith6mghyperbaric lev-obupivacaineforanalsurgery.Sensoryblockwaslimitedto S4dermatomeintheperianalblockgroupprovidedby1.5mg hyperbaric levobupivacaine.They stated that1.5mgdose of intathecal hyperbariclevobupivacaine providedshorter duration andfaster regression of sensoryblock compared with 6mg hyperbaric levobupivacaine.4 Kazak et al. kept thepatientsinthesittingpositionatleast20mininorder toconfinethesmallbolus oflevobupivacainetothelower endoftheduralsac.Asdifferentfromthestudyperformed byKazaketal.,inthepresentstudy,thepatientswerekept in the sitting positionfor 5min. The S4sensory blockade wasachievedin3minandmaximumblockedsensorylevel reachedtoS1level,soitcanbesaidthattherewasnodelay inreadinessforsurgery.
Inconclusion,wefoundthatthetworegimensprovided goodqualityspinalanesthesiainanorectalsurgerywithout affecting the motor functions and hemodynamic stability. Howeverthe additionof 25fentanyl increased duration
ofsensoryanalgesiawithlongerfirstanalgesicrequirement time without prolonging time to void or intensifying the motorblockade.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MaroofM,KhanRM,SiddiqueM,etal.Hypobaricspinal anasthe-sia(0.1%)givesselectivesensoryblockforano-rectalsurgery. CanJAnaesth.1995;42:691---4.
2.Burlacu CL,Buggy DJ.Updateonlocalanesthetics: focuson levobupivacaine.TherClinRiskManage.2008;4:381---92.
3.GurbetA,TurkerG,GirginNK,etal.Combinationofultra-low dose bupivacaineand fentanyl for spinal anaesthesiain out-patientanorectalsurgery.JIntMedRes.2008;36:964---70.
4.KazakZ,EkmekciP,KazbekK.Hyperbariclevobupivacainein analsurgery.Anesthetist.2010;59:709---13.
5.Cuvas O, GulecH, KaraaslanM, et al. The useof low dose plainsolutionsoflocalanaestheticagentsforspinalanaesthesia intheproneposition:bupivacainecomparedwith levobupiva-caine.Anaesthesia.2009;64:14---8.
6.Gouveia MA, Imbelloni LE. Understanding spinal anesthesia. ActaAnaesthesiolScand.2006;50:260.
7.Povey HM,Jacobsen J, Westergaard-Nielsen J. Subarachnoid analgesiawithhyperbaric0.5%bupivacaine:effectofa60-min periodofsitting.ActaAnaesthesiolScand.1989;33:295---7.
8.Goel S, Bhardwaj N, Grover VK. Intrathecal fentanyl added tointrathecalbupivacainefordaycasesurgery:arandomized study.EurJAnaesthesiol.2003;20:294---7.
9.CamorciaM,CapognaG,BerrittaC,etal.Therelativepotencies formotorblockafterintrathecalropivacaine,levobupivacaine, andbupivacaine.AnesthAnalg.2007;104:904---7.
10.HuntCO,NaultyJS,BaderAM,etal.Perioperativeanalgesia withsubarachnoidfentanyl-bupivacaineforcesareandelivery. Anesthesiology.1989;71:535---40.
11.Akerman B,Arweström E,Post C.Localanesthetics potenti-atespinal morphineantinociception. AnesthAnalg. 1988;67: 943---8.
12.ErBay RH, Ermumcu O, Hancı V, et al. A comparison of spinalanesthesiawithlow-dosehyperbariclevobupivacaineand hyperbaricbupivacainefortransurethralsurgery:arandomized controlledtrial.MinervaAnestesiol.2010;76:992---1001.
13.GirginNK,GurbetA,TurkerG,etal.Thecombinationof low-dose levobupivacaine and fentanyl for spinal anaesthesia in ambulatory inguinal herniorrhaphy. J Int Med Res. 2008;36: 1287---92.
14.Simon L, Boulay G, Ziane AF, et al. Effect ofinjection rate onhypotensionassociatedwithspinalanesthesiaforcesarean section.IntJObes.2000;9:10---4.
15.GudaityteJ, MarhertieneI,Pavalkis D,etal. Minimal effec-tivedoseofspinalhyperbaricbupivacaineforadultanorectal surgery:adoubleblind,randomizedstudy.Medicine(Kaunas). 2005;41:675---84.