RevBrasAnestesiol.2014;64(3):173---176
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Official Publication of the Brazilian Society of Anesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
the
effects
and
complications
of
unilateral
spinal
anesthesia
versus
standard
spinal
anesthesia
in
lower-limb
orthopedic
surgery
Seyyed
Mostafa
Moosavi
Tekye,
Mohammad
Alipour
∗DepartmentofAnesthesiology,MashhadUniversityofMedicalSciences,Mashhad,Iran
Received15April2013;accepted10June2013 Availableonline25October2013
KEYWORDS
Spinalanesthesia; Unilateral; Bupivacaine; Lowerlimb
Abstract
Introduction:Arestrictedsympatheticblockduringspinalanesthesiamayminimize hemody-namic changes.This prospectiverandomizedstudy compared unilateralandbilateral spinal anesthesiawithrespecttotheintra-andpostoperativeadvantagesandcomplicationsofeach technique.
Materialandmethods: Spinalanesthesiawasinducedwith0.5%hyperbaricbupivacaineanda 25-GQuinckeneedle(Dr.J)intwogroupsofpatientswithphysicalstatusASAI---IIwhohadbeen admittedfororthopedicsurgeries.IngroupA,duralpuncturewasperformedwiththepatient inaseatedpositionusing2.5cm3ofhyperbaricbupivacaine.Eachpatientwasthenplacedin
thesupineposition.
IngroupB,duralpuncturewasperformedwiththepatientinthelateraldecubitusposition with 1.5cm3 ofhyperbaricbupivacaine.The lowerlimb wasthe targetlimb.The speed of
injectionwas1mL/30s,andthedurationoftimespentinthelateraldecubituspositionwas 20min.
Results:Thedemographicdataweresimilarinbothgroups.Thetimetotheonsetofthesensory andmotorblockwassignificantlyshorteringroupA(p=0.00).Thedurationofmotorandsensory blockwasshorteringroupB(p<0.05).
The successratefor unilateral spinalanesthesia ingroupB was 94.45%.In twopatients, thespinalblockspreadtothenon-dependentside.Theincidenceofcomplications(nausea, headache,andhypotension)wasloweringroupB(p=0.02).
Conclusion: Whenunilateralspinalanesthesiawasperformedusingalow-dose,low-volumeand low-flowinjectiontechnique,itprovidesadequatesensory-motorblockandhelpstoachieve stable hemodynamicparameters during orthopedicsurgery ona lower limb.Patients were more satisfied with thistechnique asopposed to theconventional approach. Furthermore, thistechniqueavoidsunnecessaryparalysisonthenon-operatedside.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](M.Alipour).
174 S.M.MoosaviTekye,M.Alipour
Introduction
Thepatientswhoundergoorthopedicsurgeryonthelower limb differin terms ofage aswell asthetype ofsurgery performed.Regionalanesthesia, especiallyspinal anesthe-sia,isbeneficialformost ofthesepatients.Overthepast fewyears,bupivacainehasbeenusedroutinelyforepidural andspinalanesthesia.1,2Unilateralandbilateralspinal
anes-thesiarequiredifferentvolumesanddosesofbupivacaine.3
Unilateralspinalanesthesiaisusedduringmostsurgical proceduresperformedonthelowerlimbs.4Therearemany
benefits to this technique including fewer hemodynamic changes,5 less urinary retention, more satisfied patients,
bettermotilityduringrecoveryandtherestrictionof selec-tivenerveblocktotherelevantlimb.6
Several factors are required for successful unilateral spinalanesthesia,including:thetypeofneedleanditsbevel direction, the speed of injection,7 volume, baricity, the
concentrationoflocalanesthesiaaswellasthepositionof thepatientontheoperatingtable.8
Tocomprehensivelyinvestigatethebenefitsofunilateral ascomparedwithbilateralspinalanesthesia,weevaluated the effects on sufficient sensory and motor block, opti-mum analgesia, hemodynamic changes, nausea, vomiting andheadache.
Materials
and
methods
Thepatientsweredividedintworandomizedgroupsof36 patients:AandB.
IngroupA,standardspinalanesthesiawasusedoneven days.In groupB,unilateral spinalanesthesiawasusedon odd days. Patient age ranged from 18 to 50 years. The patientswereinASAclassIorII.ThedurationofNilperos (NPO)timeandthesedationregimenwerethesameinboth groups.Anypatientwhohadahistoryofcardiovascular dis-ease,hypertension,neuropathy,addiction,orsmockingwas excludedfromthestudy.Patientswhocouldnotbeplaced in a lateralposition (e.g., due toa pelvisfracture) were alsoexcludedfromthestudy,aswerepatientswhorequired generalanesthesiaduringsurgeryorasurgeryrequiringover 2h.
Ethicalapprovalforthisstudy(protocolnumber:891001) wasprovidedbytheMashhadUniversityethicscommittee, Mashhad,Iran(ChairpersonDr.TavakkolAfshar)on18June 2011.Informedconsentwasobtainedfromeachpatientto ensurethatheorshe understoodthatthe techniqueused forspinalanesthesiawouldbemodified.
AnIVcannulawasinserted,thena10mL/kgintravenous infusion of lactated Ringer’s solution was administered over 20min. All patients underwent standard monitoring, includingelectrocardiography, non-invasiveblood-pressure measurementsandpulsoximetry.
In group A, spinal anesthesia wasperformed with the patientinthesittingpositionattheL3---L4interspaceusinga 25-GQuinckespinalneedle(Dr.J)insterilecondition.Once intrathecalplacementhadbeenconfirmed,2.5mLof hyper-baricbupivacaine0.5%wasinjected.Thepatientwasthen placedinthesupineposition.
IngroupB,thepatientswereplacedinthelateral decu-bitus position withthe target limb in the lower position.
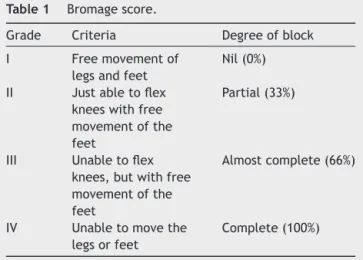
Table1 Bromagescore.
Grade Criteria Degreeofblock
I Freemovementof
legsandfeet
Nil(0%)
II Justabletoflex kneeswithfree movementofthe feet
Partial(33%)
III Unabletoflex knees,butwithfree movementofthe feet
Almostcomplete(66%)
IV Unabletomovethe legsorfeet
Complete(100%)
SimilartothetechniqueusedforgroupA,theL3---L4 inter-vertebralspace wasdetected, then spinalanesthesiawas performed with a 25-G Quincke spinal needle. After the confirmation of intrathecal needle placement, 1.5mL of hyperbaricbupivacaine0.5%wasinjectedataspeedof1cm3
every30s.Thebeveloftheneedlepointeddownwardduring theinjection.Thepatientswerekeptinthelateralposition for20minandthenplacedinthesupinepositionforsurgery. To reduce patient anxiety, 2mg of midazolam was injectedI.V.
Hemodynamicvariablessuchasbloodpressureandheart ratewerecheckedbeforespinalanesthesiaandthenevery 5min inbothgroups. Ifblood pressuredecreased bymore than 25% of baselineand heart ratedropped toless than 50beats/min, the patient was considered to suffer from hypotensionorbradycardia,respectively.
The hypotension was managed by rapid IV infusion of 250mLoflactatedRinger’ssolution.Bradycardiawas man-agedusing0.5---1mgofintravenouslyadministeredatropine. If the hypotensive patient did not respond totreatment, ephedrine5mgwasinjected.Avisualanalogscaleranging from0to10wasusedforevaluationofnauseaandthe num-berofvomitingepisodeswereusedtoevaluatetheextent ofpatientvomiting.
Tocheck thelevel of sensoryblock,a cold objectwas heldincontactwiththeskin.TheBromagescalewasused tochecktheaccuracyofthemotorblock(seeTable1).9
Theclinicaldataincludingtheonsetofsensoryandmotor block,hemodynamic changes,thedurationofsensoryand motorblockandthecomplicationsofspinalanesthesiawere evaluatedusingSPSSversion19.6.
Inthisstatisticalanalysis,apvalueof<0.05was consid-eredassignificant.
Forstatisticalanalysisofthehemodynamicchanges,the pairedt-testwasused.
Theindependentt-testwasusedtocomparetheefficacy ofthesensoryandmotorblocks.TheMann---WhitneyU-test wasusedtoevaluatethelevelofpatientsatisfaction.
Results
Spinalanesthesiaforlower-limborthopedicsurgery 175
Table2 Demographicdata.
Specification Bilateral group n=36
Unilateral group n=36
p-Value
Age 31.5±5.37 26.7±7.55 >5%
Sex
Male 25 27 >5%
Female 11 9 >5%
Weight 74.7±11.60 75.71±9.30 >5% Durationof
surgery(min)
95.15±10.07 94.20±9.67
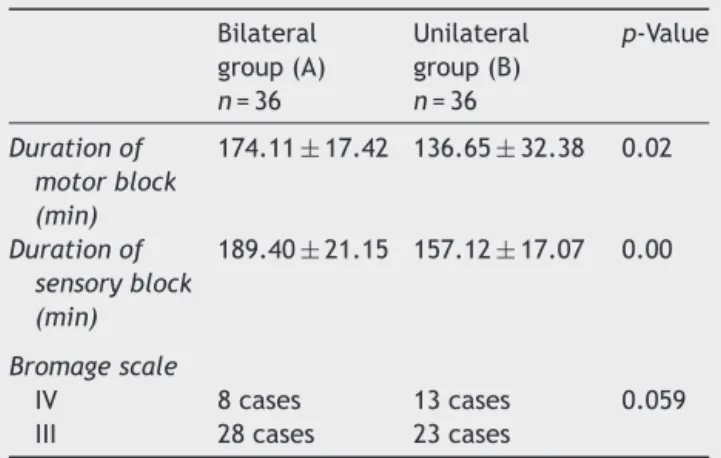
---Table3 Durationofmotorandsensoryblock.
Bilateral group(A) n=36
Unilateral group(B) n=36
p-Value
Durationof motorblock (min)
174.11±17.42 136.65±32.38 0.02
Durationof sensoryblock (min)
189.40±21.15 157.12±17.07 0.00
Bromagescale
IV 8cases 13cases 0.059
III 28cases 23cases
was 4.47±1.3min. In the bilateral group, this value was 2.44±0.41min(pvalue=0.00).
Theaveragetimetotheonsetofimmobilityinthe uni-lateralgroupwas6.17±1.5min.Inthebilateralgroup,this ratewas4.35±1.25min(pvalue=0.00).Sensoryandmotor block lastedlongerin the bilateral group ascomparedto theunilateralgroup(Table3).AnaverageBromagescoreof 4wasachievedforthemotorblockinbothgroups(p=0.59). Noneofthepatientsintheunilateralgroupexperienced nauseaor vomiting.In the bilateral group, eightpatients hadnauseaandoneofthemexperiencedepisodesof vomi-ting(p=0.02).Twopatientsintheunilateralgroupandeight patients in the bilateral group had headaches (p=0.03). The average time to voiding after spinal anesthesia was 4.9hintheunilateralgroupand5.3hinthebilateralgroup (p>0.05).Thelevelofpatientsatisfactionwas91.2%inthe unilateralgroupand85.3%inthebilateralgroup(p>0.05).
TheratesofcomplicationsarepresentedinTable4.
Table4 Complications.
Complications Unilateral (number)
Bilateral (number)
p-Value
Nauseaand vomiting
0 8 0.02
Headache 2 8 0.03
Hypotension 0 6 0.02
Bradycardia 0 5 0.02
The successrate for unilateralspinal anesthesiainour study was 94.45%, but in two cases, the anesthetic drug spreadtotheothersideofthecanal,resultinginbilateral anesthesia.
Discussion
Thepatient’spositionduringandimmediatelyafterspinal anesthesiainfluencesthespinaldistributionofdrugs.Ifan anestheticdrugsolutionishypo-orhyperbaricwithrespect tothe cerebrospinal fluid, it is possible to create a uni-lateralblock.Moreover,thedistancebetweentheleftand rightnerverootsinthelumbarandthoracicregionsisabout 10---15cm, which makes it possible to achieve unilateral spinalanesthesia.10
Kuusniemi et al. reported that hyperbaric bupivacaine ismore effective in achievingunilateral spinal anesthesia thanplainbupivacaine.11However,determiningtheoptimal
timeforlateralpositioningisdifficultwhenahighdoseof hyperbaric bupivacaine (12---20mg) is used.12,13 The
anes-theticdrugmaymigrateevenwhenthepatientisplacedin thelateralpositionfor30---60min.Conversely,ifalowdose (5---8mg)ofanestheticsolutionisused,puttingthepatient inthelateralpositionfor10---15minmaypreventmigration oftheanestheticdrug.
In this study, we injected 1.5cm3 of hyperbaric
bupi-vacaine0.5% toachieve unilateral spinal anesthesia. The patientwaskeptin the lateralposition for 20min, which ledtounilateralspinalanesthesiain94.45%ofcases.Intwo cases,theanestheticdrugspreadtotheotherside, result-inginbilateralspinal anesthesia.In astudyperformed by Esmaoglu,thepatientwasinthelateralpositionfor10min. Thisapproachyieldedan85.7%success rate.This discrep-ancyintermsofthesuccessrateseemstobedependenton thedurationoftimespentinthelateralposition.4
Notably,noneofthepatientsintheunilateralspinal anes-thesia groupexperienced hypotension, but six patients in thebilateralgrouphadhypotension(p<0.05).Chohanand Afshan administered unilateral spinal anesthesia prior to lower-limbsurgeryinelderlypatientswithASAclassification ofIIIorIV(averageage,60).Theauthorsfoundnosignificant hemodynamic changes.They used hyperbaric bupivacaine 0.5%(1.1---1.8mL).14
Inourstudy,therewasnobradycardiaintheunilateral group,butinthebilateralgroup,5patientshadbradycardia (p=0.04).Onaverage,thetimetotheonsetofanesthesia andimmobilitywasfaster inthebilateral ascomparedto theunilateralspinalanesthesiagroup(p=0.00).Thesensory andmotorblocklastedforlesstimeintheunilateralas com-paredtothebilateralgroup.Unilateralspinalanesthesiais thereforesuitableforout-patientsurgery.
Valanneused4or6mgofbupivacainetoinduceunilateral spinalanesthesiain106patientsscheduledtoundergoknee arthroscopy. While both doses were sufficient for sensory andmotorblock,4mgofbupivacaineachievesamorerapid regressionofmotorfunction.15
Headache after spinal anesthesia wasreported in two and eightpatients in the unilateral and bilateral groups, respectively.Incontrast,Smaoglueused1.5cm3and3cm3
176 S.M.MoosaviTekye,M.Alipour
experiencedheadache.Thisdiscrepancymayberelatedto thetypeof needleused(Quincke)or therelatively young ageofthepatientpopulation.16
Notably,spinal anesthesiacandisturb bladderfunction bydisablingthemicturitionreflex.Kamphuisandcolleagues reportedthatvoidingdisturbancecontinuesuntilthenerve blockhasregressedtothethirdsacralroot.17
In our investigation, theaverage timetovoiding after spinal anesthesia was 4.9 and 5.3h in the unilateral and bilateralgroups, respectively.This differencewasnot sig-nificant. Atef et al. reported no urinary retention after unilateral spinal anesthesiawith5mgof hyperbaric bupi-vacaine,while intheirstudy,afterinductionwith12.5mg dosage, thiscomplication observed in five percentof the subjects. So, it appears that a reduction in the bupiva-cainedosagedecreasesthelikelihoodofurinaryretention, aswell.18
Conclusion
Unilateralspinalanesthesiawithalowdose(7.5mg),limited volume(1.5cm3)andlow-flowinjection(1cm3/30s)
tech-nique induces sufficient sensory and motor block with an appropriatelevelofanalgesia.The techniqueis therefore suitableforlower-limbsurgery.Thistechniqueachieves sta-ble hemodynamics, particularly in elderly and ASA class III/IVpatients.Italsoresultsinrapidrecoveryandgreater satisfactionamong outpatients, in addition to preventing unnecessarynerveblockinthecontralaterallimb.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.TuominenM.Bupivacainespinalanaesthesia.ActaAnaesthesiol Scand.1991;35:1.
2.Stanton-Hicks M, Murphy TM, Bonica JJ, et al. Effects of extradural block: comparison of the properties, circulatory effects andpharmacokinetics ofetidocaineand bupivacaine. BrJAnaesth.1976;48:575.
3.LiuSS,WarePD,AllenHW, etal.Doseresponse characteris-ticsofspinal bupivacaineinvolunteers.Clinicalimplications forambulatoryanesthesia.Anesthesiology.1996;85:729---36.
4.EsmaogluA,BoyaciA,Ersoy O,etal. Unilateralspinal anes-thesiawithhyperbaricbupivacaine.ActaAnaesthesiolScand. 1998;42:1083---7.
5.CasatiA,FanelliG,AldegheriG,etal.Frequencyofhypotension duringconventionalorasymmetrichyperbaricspinalblock.Reg AnesthPainMed.1999;24:214---9.
6.BorghiB,StagniF,BugamellisS,etal.Unilateralspinalblock foroutpatientkneearthroscopy: adose findingstudy.JClin Anesth.2003;15:351---6.
7.CasatiA,FanelliG,CappelleriG,etal.Doesspeedofintrathecal injectionaffectthedistributionof0.5%hyperbaricbupivacaine? BrJAnaesth.1998;81:355---7.
8.AlMalyanM,Becchi C,Falsini S,et al. Roleofpatient pos-tureduringpunctureonsuccessfulunilateralspinalanaesthesia in outpatient lower abdominal surgery. Eur J Anaesthesiol. 2006;23:491---5.
9.BromagePR. Epidural Analgesia.Philadelphia: WB Saunders; 1978.p.144.
10.EduardoImbelloniL, BeatoL, AntonioT.Carderiro-unilateral spinalanesthesiawithlow%0.5hyperbaricbupivacainedose. Anestesiology.2004;54.
11.KuusniemiKS,PihlajamakiKK,PitkanenMT.Alowdoseofplain orhyperbaricbupivacaineforunilateralspinalanesthesia.Reg AnesthPainMed.2000;25:605---10.
12.LotzSMN,CrosgnacM,KatayamaM,etal.Anestesia subarac-noideacombupivacainaa0.5%hiperbarica:influenciadotempo depermanenciaemdecubitolateralsobreadispersaocefalica. RevBrasAnestesiol.1992;42:257---64.
13.Povey HM, Jacobsen J, Westergaard-Nielsen J. Subarach-noid analgesia with hyperbaric 0.5% bupivacaine: effect of a 60-minutes period of sitting. Acta Anaesthesiol Scand. 1989;33:295---7.
14.ChohanU,AfshanG,HodaMQ.Hemodynamiceffectsof unilat-eralspinalanesthesiainhigh riskpatients.JPak MedAssoc. 2002:52---66.
15.ValanneJV,KorhoneuA-M, JakelaRM,etal. Selectivespinal anesthesia: a comparison of hyperbaric bupivacaine 4mg versus 6mg for outpatient knee arthroscopy. Anesth Analg. 2001;93:1377---9.
16.EsmaogluA,Karaoglus,MizrakA,etal.Bilateralvsunilateral spinalanesthesiaforoutpatientkneearthroscopies.KneeSurg SportsTraumatolArthrosc.2004;12:155---8.
17.KamphuisET,IonescuTI,KuipersPWG,etal.Recoveryof stor-ageandemptyingfunctionsoftheurinarybladderafterspinal anesthesiawithlidocaineandwithbupivacaineinmen. Anes-thesiology.1998;88:310---6.