REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
A
comparison
of
different
densities
of
levobupivacaine
solutions
for
unilateral
spinal
anaesthesia
Özgür
Ya˘
gan
a,∗,
Nilay
Tas
¸
a,
Ahmet
Küc
¸ük
b,
Volkan
Hancı
caOrduUniversity,SchoolofMedicine,DepartmentofAnesthesiology,Ordu,Turkey
bHarranUniversity,SchoolofMedicine,DepartmentofAnesthesiology,Sanlıurfa,Turkey
cDokuzEylülUniversity,SchoolofMedicine,DepartmentofAnesthesiology,Izmir,Turkey
Received31May2014;accepted7August2014 Availableonline26November2014
KEYWORDS
Hyperbaric levobupivacaine; Unilateralspinal anaesthesia; Arthroscopicknee surgery
Abstract
Backgroundandobjectives: Theaimofthestudywastocomparetheblockcharacteristicsand
clinicaleffectsofdextroseaddedtolevobupivacainesolutionsatdifferentconcentrationsto provideunilateralspinalanaesthesiainlowerextremitysurgery.
Methods:Thisprospective,randomised,double-blindstudycomprised75ASAI---IIriskpatients
forwhomunilateraltotalkneearthroscopywasplanned.Thepatientswereassignedtothree groups: inGroup I, 60mg dextrosewas added to7.5mg of0.5%levobupivacaine, inGroup II,80mgandinGroupIII,100mg.Spinalanaesthesiawasappliedtothepatientinthelateral decubituspositionwiththeoperatedsidebelowandthepatientwaskeptinpositionfor10min.
Results:Thetimefor thesensorialblocktoachieveT12levelwas slowerinGroupIthanin
GroupsIIandIII(p<0.05,p<0.00).Thetimetofullrecoveryofthesensorialblockwas136min in Group I, 154min inGroup II and170min inGroup III.The differences were statistically significant(p<0.05).Themeandurationofthemotorblockwas88mininGroupI,105minin GroupII,and139mininGroupIIIandthedifferenceswerestatisticallysignificant(p<0.05). ThetimetourinationinGroupIwasstatisticallysignificantlyshorterthanintheothergroups (p<0.00).
Conclusions: Theresultsofthestudyshowed thattogetherwithanincreaseindensity,the
sensoryandmotorblockdurationwaslengthened.Itcanbeconcludedthat30mgmL−1
concen-trationofdextroseaddedto7.5mglevobupivacaineissufficienttoprovideunilateralspinal anaesthesiainday-casearthroscopickneesurgery.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](Ö.Ya˘gan). http://dx.doi.org/10.1016/j.bjane.2014.08.009
PALAVRAS-CHAVE
Levobupivacaína hiperbárica; Raquianestesia unilateral;
Artroscopiadojoelho
Umacomparac¸ãodasdiferentesdensidadesdassoluc¸õesdelevobupivacaína
pararaquianestesiaunilateral
Resumo
Justificativaeobjetivos: Oobjetivodesteestudofoicompararascaracterísticasdobloqueio
e os efeitos clínicos da adic¸ão de dextrose às soluc¸ões de levobupivacaína em diferentes concentrac¸õesparaproporcionarraquianestesiaunilateralemcirurgiadeextremidadeinferior.
Métodos: Estudoprospectivo,randômico eduplo-cego conduzidocom75 pacientes, estado
físicoASA I-II,programadospara artroplastia unilateraltotal dojoelho.Ospacientesforam divididosem trêsgrupos:noGrupo-I,60mgdedextroseforamadicionadosa7,5mgde lev-obupivacaínaa0,5%;noGrupoII,80mgenoGrupoIII,100mg.Araquianestesiafoiaplicadaao pacienteposicionadoemdecúbitolateral,comoladooperadoabaixo,eopacientefoimantido emposic¸ãodurante10minutos.
Resultados: OtempoparaobloqueiosensorialatingironívelT12foimaislentonoGrupo-Ique
nosgruposIIeIII(p<0,05,p<0,00).Otempoderecuperac¸ãototaldobloqueiosensorialfoi de136minutosnoGrupo-I,154minutosnoGrupo-IIe170minutosnoGrupoIII.Asdiferenc¸as foramestatisticamentesignificativas(p<0,05).Amédiadadurac¸ãodobloqueiomotorfoide88 minutosnoGrupo-I,105minutosnoGrupo-II,e139minutosnoGrupo-III,easdiferenc¸asforam estatisticamentesignificativas(p<0,05).Otempodemicc¸ãofoisignificativamentemenorno Grupo-Iquenosoutrosgrupos(p<0,00).
Conclusões:Osresultadosdoestudomostraramque,juntocomumaumentodadensidade,a
durac¸ãodosbloqueiossensorialemotorfoiprolongada.Pode-seconcluirqueumaconcentrac¸ão 30mgmL−1dedextroseadicionadaa7,5mgdelevobupivacaínaésuficienteparaproporcionar
raquianestesiaunilateralparaartroscopiadojoelhoemregimeambulatorial.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
In vitro studies have shown that differences in the spe-cificdensitiesoflocalanaestheticsolutioncansignificantly affect the clinical presentation of spinal block.1 Better controloftheblocklevelisprovidedwithhyperbaric solu-tionscomparedtoisobaric solutionsand therefore,fewer sideeffects,suchashypotensionanduncontrollableblock height, are expected.2 Other advantages of hyperbaric formsarethataunilateralblockcanbecreatedandthere isalowerrateoffailedblocks.2
Previousstudieshavecomparedthehyperbaricformof levobupivacainewiththeisobaricformandotherhyperbaric localanaesthetics.Ithasbeenreportedinliteraturethata hyperbaricsolution is obtainedby addingdextrose at dif-ferent concentrations to levobupivacaine.3---6 However, to the bestof our knowledge, there is no previous compar-ativestudy on themost appropriate dextrose contentfor unilateralspinalanaesthesia.
The hypothesis of this study wasthat with the lowest dextrose content to achieve unilateral block, more sta-ble haemodynamics and shorter duration of sensory and motorblockcanbeobtained.Withtheaim oftestingthis hypothesis, in this prospective, randomised, double-blind study,acomparisonwasmadeoftheblockcharacteristicsof levobupivacainemLformscontaining30,40and50mg dex-trosefor unilateral spinal anaesthesiain lower extremity surgery and their suitability for day procedure anaesthe-sia.
Methods
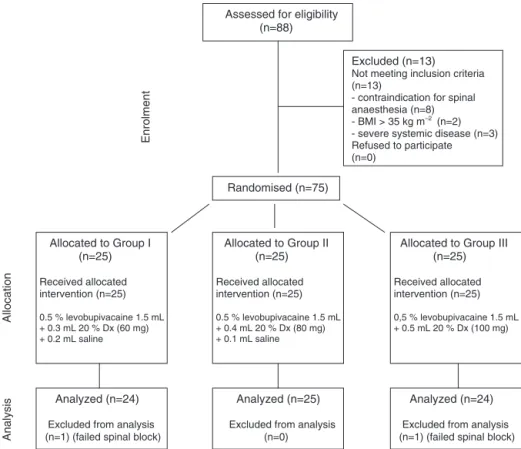
AfterEthicsCommitteeapprovalandClinicalTrials registra-tion(NCT01938755),75 ASA I---IIrisk patients,aged 18---65 years,for whomelective unilateral knee arthroscopywas plannedwereincludedinthestudy.TheConsolidated Stan-dardsof Reporting Trials(CONSORT) recommendationsfor reporting randomised, controlled clinical trials were fol-lowed (Fig. 1).7 Informed consent was obtained from all the patients. Exclusion criteria were contraindication for spinalanaesthesia,severesystemicdisease,allergytolocal anaesthetic,peripheralneuropathy,bodymassindex(BMI) >35kgm−2, psychiatric disorders and chronic pain treat-ment.
Assessed for eligibility (n=88)
Excluded (n=13)
Not meeting inclusion criteria (n=13)
- contraindication for spinal anaesthesia (n=8) - BMI > 35 kg m–2
(n=2) - severe systemic disease (n=3) Refused to participate (n=0)
Randomised (n=75)
Allocated to Group I (n=25)
Received allocated intervention (n=25)
0.5 % levobupivacaine 1.5 mL + 0.3 mL 20 % Dx (60 mg) + 0.2 mL saline
Allocation
Enrolment
Allocated to Group II (n=25)
Received allocated intervention (n=25)
0.5 % levobupivacaine 1.5 mL + 0.4 mL 20 % Dx (80 mg) + 0.1 mL saline
Analysis
Analyzed (n=25)
Excluded from analysis (n=0)
Analyzed (n=24)
Excluded from analysis (n=1) (failed spinal block)
Allocated to Group III (n=25)
Received allocated intervention (n=25)
0,5 % levobupivacaine 1.5 mL + 0.5 mL 20 % Dx (100 mg)
Analyzed (n=24)
Excluded from analysis (n=1) (failed spinal block)
Figure1 CONSORTflowdiagramofthisrandomisedtrial.7
waterandinGroupIII(n=25),0.5mL20%dextrose(100mg) atotalamountof2mLwasdefined.Thedensitiesmeasured at37◦Cofthelevobupivacainewith30mgmL−1,40mgmL−1 and50mgmL−1dextrosewere1.008,1.014and1.019gL−1, respectively.MeasurementsweremadewithiQ200(Iris Diag-nostics,Chatsworth,CA).
Spinalanaesthesiawasappliedwithamidlineapproach fromthe3rdand4thintervertebralspacewiththepatient inthelateraldecubituspositionwiththesidetobeoperated onbelow.AQuinketipped25Gspinalneedle(Spinocan,B. Braun,Melsungen, Germany)wasusedwiththetipfacing downwards and,without barbotage, theanaesthetic solu-tion was administered to all the patients at the rate of 0.1mLs−1. Patients were kept in position for 10min and thenmovedintoasupinepositionand0.03mgkg−1iv mida-zolamwasadministered.Whenthesensoryblockachieved T12levelontheoperationside,theoperationwasstarted. Thesensoryandmotorblockofthepatientswas evalu-atedevery5minstartingfromthetimeofapplication(0min) by a researcher blind tothe group distribution. The sen-soryblockwasevaluatedwiththepinpricktestwitha22G hypodermic needletouching thedermatomes onthe mid-clavicularlinebilaterallyandthemotorblockwasevaluated withthemodifiedBromagescale(0=nomotorblock,1=only thekneeand footcanbemoved,2=onlythefootcan be moved,3=full motorblock).At theendofthe operation, theblocklevelswerecheckedat15-minintervalsuntilthe blockwascompletelyremoved.
Atthetimesofsensoryandmotorblockevaluations,the haemodynamicdatawererecorded. Accordingtothe pre-operative value, a drop of 30% in mean arterial pressure
(MAP)wasacceptedashypotensionandrapidivfluid infu-sion(200mL lactated Ringer’s solution) wasadministered and in cases where noresponse could be achieved, 5mg iv ephedrine was planned. Heart beat rate falling below 50bpm−1 was accepted as bradycardia, for which it was plannedto administer0.01mgkg−1 iv atropine.The qual-ityofthespinalblockanaesthesiawasevaluatedaccording to the need for iv sedative or analgesia support.8 Suffi-cientspinalblock=norequirementforsedativeoranalgesia untilthesurgerywascompleted,insufficientspinalblock=a requirement for additional analgesia (1mcgkg−1 iv bolus fentanyl)orsedative(1mgkg−1ivboluspropofol)for com-pletionofsurgery,failedspinalblock=generalanaesthesia requiredto complete surgery.Additional tothespread of theblock, arecordwasmadeof thetimetofullrecovery ofthesensoryblock(evaluated asnoremainingfeelingof numbnessintheleg),timetodurationofthemotorblock (timeof Bromage=0) and thetime of the first urination. Postoperative analgesia consisted of 75mg im diclofenac sodium(Diclomec,AbdiIbrahim,Istanbul,Turkey)every12h onrequestontheoperationday.
Poweranalysis
Table1 Patientscharacteristicsanddurationofsurgery.Dataarepresentedasmean±SDorfrequencies.
GroupI(n=24) GroupII(n=25) GroupIII(n=24) p
Age(year) 36.1±8.3 36.0±8.4 35.8±8.4 NS
BMI(kgm−2) 25.2
±3.3 24.7±3.4 24.5±3.5 NS
Gender(F/) 14/10 12/13 13/11 NS
ASAI/II 15/9 18/7 17/7 NS
Durationofsurgery(min) 38.5±6.5 38.6±5.8 37.2±6.4 NS
NS,notsignificant;BMI,bodymassindex;F/M,female/male;ASA,AmericanSocietyofAnesthesiologist.
effectsize tostandard deviationratio of 0.9 accepting a two-tailed˛errorof5%andaˇerrorof20%.12
Statisticalanalysis
Statisticalanalysiswasperformed usingthe programSPSS 20.0 (IBM SPSS Statistics, Chicago, IL, USA). Continu-ous variables are presented as mean±SD or as median (range); categorical data are presented as number (%). Kruskal---Wallis test and Mann---Whitney U test were used toassess thedemographicdata,maximum sensorialblock level,timetoreachmaximumsensorialblocklevelandtime toreachmaximummotorblocklevel.TheWilcoxontestwas usedfor repeatedmeasurementsingroups.ASA classifica-tions,gender, Bromage scale, numberof hypotensionand bradycardiaepisodesingroupswereassessedwiththe chi-squaretest.Valueofp<0.05wasconsideredasastatistically significant.
Results
Atotalof 73patients wereenrolledin thestudy(Fig.1). Patientswhowererequiredgeneralanaesthesia(1patient inGroupIand1inGroupIII)asaresultoftechnicalfailure wereexcludedfromthestudy.Additionaldosesoffentanyl andpropofolwereadministeredtothreepatientsinGroup I and one patient in Group II during surgery. No statisti-callysignificantdifferenceswereobservedamongthethree groups.
The groups were comparable with regard to age, sex, BMI, ASA status and duration of surgery (Table 1). The onsettimeofT12level ofsensorial blockwasmorerapid in Group II and Group III compared to Group I (p=0.03 and p=0.003 respectively). No significant difference was observedbetweenGroupIIandGroupIII.Maximumsensorial blockheightwassignificantlydifferentbetweenGroupIand GroupIII (p=0.02).The timetoreachmaximum sensorial blocklevel andtwo-segment regressiontimes ofsensorial blockdidnotdiffersignificantlyamongallgroups(Table2). InGroupIII,at theminute150,theoperativeside sen-sorialblock level wassignificantly higher than in Group I (p=0.043). No significant differencebetween groups was observedfortheoperativesidesensorialblocklevelsatthe othertimepoints(Fig.2).Thenonoperativesidesensorial blockdidnotsignificantlydifferamongthethreegroupsat the all time points (Fig. 3). In Group I, the time to full recovery of sensorial block was significantly shorter than othergroups andGroup II significantlyshorter thanGroup
III(Table2).
The operative side degree of motor block was signifi-cantly less in the Group Icompared withthe Group III in theminutes10,30,45,and120.Grade3motorblockwas not observedon thenonoperative side of thecases in all groups. The duration ofmotor block wassignificantly dif-ferentamongthethreegroups(Table2).Thefirsturination timewassignificantlyshorterinGroupIcomparedtoother groups(Table2).
Cardiovascular changes were minimal in groups. MAP levelsofallmeasurementsequencesweredecreased signif-icantlywhencomparedtopreoperativevalueswhichwere obtainedinthreegroups.Incomparisonsamongthegroups, therewerestatisticaldifferencesbetweentheGroupsIIand IIIattheminute5,betweentheGroupsIandIIIattheminute 210(Fig.4).InitialHRsweredecreasedduringthefollow-up period(Fig.5).Therewerenostatisticaldifferencesamong thethreegroups in incidenceofhypotensionor bradycar-dia.Theadverseeventsduringthestudyperiodareshown
T10
T12
L2
L4
S1
10 15 20 30 45 60 90 120 150
Bloc
kheight (der
matome)
Operative side
Group I Group II Group III
Time (min)
Figure 2 Median level of operative side sensory block in groups.
T10
T12
L2
L4
S1
10 15 20 30 45 60 90 120 150
Bloc
kheight (der
matome)
Nonoperative side
Group I Group II Group III
Time (min)
Table2 Characteristicsofintrathecalblockswithdifferentdextroseconcentration.Dataarepresentedasmean±SD,median (min---max)orfrequencies.
GroupI(n=24) GroupII(n=25) GroupIII(n=24) pIvsII pIvsIII pIIvsIII
Sensoryblock
OnsettoT12(min) 12.5±2.2 10.6±2.9 10.4±1.6 0.03 0.00 NS Maximumcephaladspread(dermatome) T12(L1---T10) T11(L1---T8) T10(T12---T7) NS 0.02 NS Timetomaximumcephaladspread(min) 22.7±4.8 23.8±6.9 21.8±4.6 NS NS NS Timetotwosegmentregression(min) 50.4±13.2 55.2±13.5 56.8±14.6 NS NS NS Timetofullrecovery(min) 136.2±24.5 154.8±28.3 170.0±26.0 0.02 0.00 0.03
Motorblock
Grade3blockoperativeside(%) 19(79%) 21(84%) 21(87.5%) NS NS NS Grade0or1blocknonoperativeside(%) 14(58%) 15(60%) 9(37.5%) NS NS NS Timetodurationofmotorblock(min) 88.7±21.1 105.0±22.5 139.3±33.5 0.02 0.00 0.00 Timetourination(min) 218.7±31.2 262.8±41.7 281.2±45.8 0.00 0.00 NS
NS,notsignificant.
Table3 Frequencyofadverseevents,sideeffectsandusedephedrine,fentanylorpropofolingroups.Dataarepresentedas
frequencies(%).
GroupI(n=24) GroupII(n=25) GroupIII(n=24) p
Hypotension --- 1(4) 2(8.3) NS
Ephedrine --- 1(4) 2(8.3) NS
Bradycardia --- --- --- NS
Headache --- --- --- NS
Mildbacktenderness 1(4.2) 1(4) 2(8.3) NS
Nausea---vomiting 1(4.2) --- 1(4.2) NS
Urinaryretention --- --- 1(4.2) NS
Supplementfentanyl 3(12.5) 1(4) --- NS
Supplementpropofol 3(12.5) 1(4) --- NS
NS,notsignificant.
inTable3.Therewerenosignificantdifferencesamongall
groupsforanyoftheadverseevents.
Discussion
As a result of this study comparing levobupivacaine solu-tionswithdifferingdextrosecontentsfor unilateralspinal anaesthesia,shortersensoryandmotorblockdurationsand
105
95
85
75
0 5 10 15 20 30 45 60 90 120 150 180 210
MAP (mmHg)
Group I Group II Group III
Time (min)
Figure 4 Mean arterial blood pressure changes in groups (mmHg).Dataarepresentedasmean.*p=0.02GroupIIvsIII. †p=0.04GroupIvsIII.
timetofirsturinationweredeterminedwitha30mgmL−1 dextrosecontent.
Levobupivacaine hydrochloride is an S(−) enantiomer of racemic bupivacaine which is less toxic on the heart andcentralnervoussystem.13,14Clinicalstudieshaveshown both agents to be effective at equal doses in spinal anaesthesia.15---18 In a study which compared 5, 7.5, 10 and12.5mgdosesof0.5%bupivacaineforunilateralspinal anaesthesia in knee arthroscopy, the optimal dose was
60 65 70 80
75
0 5 10 15 20 30 45 60 90 120 150 180 210
HR (bpm)
Group I Group II Group III
Time (min)
reportedtobe7.5mg.19Therefore,thesamedosewasused inthecurrentstudy.
The difference in density between cerebrospinal fluid (CSF)andlocalanaestheticisanimportantfactorin deter-miningthedistributionofthesolutioninthesubarachnoid area. Local anaesthesia density reduces with increased temperature and increases with an increase in glucose concentration.20---22 At 37◦C the mean density of CSF is
1.0003gL−1,rangingfrom1.0000to1.0006gL−1(
±2SD).23 Solutions at a density below 0.9990 can be accepted as hypobaricandthoseabove1.0010 ashyperbaric.23 Onthe commercialmarket, theonly hyperbaric formavailable is bupivacainecontaining 8% dextrose. It hasbeen reported thatsolutioncontainingdextroseatahigherconcentration than8%willhavehyperbaricbehaviour.23 This unnecessar-ily high concentration of 8% has been reported to allow the usage of low dose and additional adjuvants.9 How-ever, in literature, local anaestheticscontaining dextrose at 8% concentration are often used for unilateral spinal anaesthesia.8,10,24 Inthe current study, thedensity of the solution containing 3% concentration dextrose in Group I wasmeasured as1.008gL−1 at 37◦C. Fromthe results of
thestudy,itwasdeterminedthatthisdifferencefromCSF indensitywassufficienttoformaunilateralblock.
Local anaesthesia which is used to provide unilateral spinalblockdependsondose,density andthedurationof thelateraldecubitusposition.9Ithasbeenreportedthatthe bestresultforunilateral blockisachievedwith10---20min waitingin thelateraldecubitus positionafter usingalow doseof localanaesthesia.25 Inthe currentstudy,a 10min waitingperiodaftertheprocedure waspreferred. Follow-ing the 10min waiting period, Grade 3 motor block was notseeninanypatientonthenonoperativeside.Thiscan beconsideredtobeduetotheuseof alowdose oflocal anaesthetic.
At the end of the current study, a sufficient level of unilateralspinalanaesthesiawasachievedwithoutleading toany seriousside effects withlevobupivacaine solutions containing dextrose at rates of 3%, 4% and 5% (30, 40 and 50mgmL−1, respectively). In Group I with the low-est dextrose content, the time to sensory block onset was longer compared to the other groups and the max-imum block level was lower than that in Group III. In literature it has been reported that an increase in local anaesthesia solution density has the effect of accelerat-ingonset6,9,26,27 and causesan increaseinmaximum block level.4,27
In thecurrent study,the timetofull recovery of both sensoryandmotorblockswasshorterinGroupI.Therehave been variousstudies onthe effectof an increase inlocal anaestheticsolutiondensityonthedurationofsensoryand motorblock. In a study byJanik etal.28 comparing bupi-vacainesolutions containingglucose at 8%and 5%,higher glucosecontentwasreportedtosignificantlylengthenthe durationofsensoryblock.Similarly,inthecurrentstudy,the resolutionofthemotorblockwasdelayed.Bannisteretal.29 compared0.5% bupivacaine solutions containingdifferent concentrationsofglucoseanddeterminedalongersensory blockdurationinthegroupwiththesolutioncontaining8% glucose.
InastudybySanansilpetal.,30 isobaricandhyperbaric solutions of levobupivacaine were compared in spinal
anaesthesia and no difference was determined in the regressiontimesofthemotorandsensoryblock.However, Sen et al.6 compared intrathecal isobaric and hyperbaric levobupivacaineinurologysurgeryandthedurationofthe motor and sensory block was found to be longer in the hyperbaric group. It can be concluded that the current study differed from that of Sanansilp in not using the isobaric form and was also different from these studies in thatunilateral spinalanaesthesiawasprovided.Similar resultstothoseofthecurrentstudywerereportedbyJanik andBannisterwherelocalanaesthesiasolutionscontaining differentconcentrationsofdextrosewereused.28,29
Ithasbeen reportedthat hyperbaricsolutionscanlead to an increase in the incidenceof cardio respiratory side effectsdepending ontheconcentrationofdextrose inthe solution.23,31Critchleyetal.32comparedthehaemodynamic effects of bupivacaine solutions, plain and containing 8% and 4% dextrose andreported that in the groupwith the solution containing 8% dextrose, haemodynamic changes startedsignificantlymorequickly.Therewasasimilarrapid onset of sensory block but the maximum sensory block level wasdetermined tobesimilarin all thegroups. The haemodynamicdataofthecurrentstudyweresimilar.In1 patientinGroupIand2patientsinGroupIII,hypotension developedandephedrinewasadministered.Itisknownthat inunilateral spinalanaesthesialowdoselocalanaesthesia canbeusedandmorestablehaemodynamicsarepresented becauseoftheselectiveblockagecreatedontheoperative side.25,33,34
In day-case surgical procedures, the time of first uri-nation and time to mobilisation are important in respect of hospitaldischarge.Postoperative mobilisationtimecan be affected by some surgical characteristics. The most frequently encountered factor restricting the meeting of discharge criteria has been reported to be the return to spontaneousurination.8Therefore,inthecurrentstudy,the timetoreturnofspontaneousurinationwastakenasa crite-riaratherthantimeofdischarge.InGroup Ithistimewas 128min,which wassignificantlyshorterthan thetimes of bothGroupIIandGroupIII.InastudybyCappellerietal.,8 in which hyperbaric forms of levobupivacaine and ropiva-caine were compared in unilateral spinal anaesthesia for kneearthroscopy,thisperiodwasreportedas238mininthe groupwith7.5mglevobupivacaineincluding8.2%glucose. Thetimetodischargeofthisgroupwasdefinedasthetime offirsturination.
Themainlimitationofthecurrentstudyisthatno com-parisonwasmadeof thetimes tomobilisationandactual discharge. The reason for this is that mobilisation and discharge of the patients may be affected by patient or surgery-relatedfactorsthatareindependentofthe anaes-thesia.
Inthisstudy,whichcomparedlevobupivacainesolutions containing3%,4%or5%dextroseforunilateralspinal anaes-thesia,whilesuccessfulunilateralspinalblockwasprovided inallthreegroups togetherwithalowside-effectprofile, extended duration of both sensory and motor block was determinedwithanincreaseindensity.Forunilateralspinal anaesthesiainday-casearthroscopickneesurgery,the addi-tionof 30mgmL−1dextroseto7.5mglevobupivacainecan beconsideredsufficient.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.StienstraR,GielenM,KroonJW,etal.Theinfluenceof tem-peratureandspeedofinjectiononthedistributionofasolution containingbupivacaineandmethyleneblue ina spinalcanal model.RegAnesth.1990;15:6---11.
2.BreitkreutzR, KesslerP.Hyperbariclevobupivacaine formula-tionforfasttrackurologicaloroutpatientsurgery:anewmagic bullet?MinervaAnestesiol.2010;76:5---6.
3.KazakZ,EkmekciP,KazbekK.Hyperbaric levobupivacainein analsurgery:spinalperianalandspinalsaddle blocks. Anaes-thesist.2010;59:709---13.
4.DjenoIT,DuzelV,AjdukM,etal.Increaseinspecificdensityof levobupivacaineandfentanylsolutionensureslowerincidence ofinadequateblock.CollAntropol.2012;36:375---80.
5.HakanErbayR,ErmumcuO, HanciV,etal.A comparisonof spinalanesthesiawithlow-dosehyperbariclevobupivacaineand hyperbaricbupivacainefortransurethralsurgery:arandomized controlledtrial.MinervaAnestesiol.2010;76:992---1001. 6.SenH,PurtulogluT,SizlanA,etal.Comparisonofintrathecal
hyperbaricandisobariclevobupivacaineinurologicalsurgery. MinervaAnestesiol.2010;76:24---8.
7.MoherD,SchulzKF,AltmanDG,CONSORT.TheCONSORT state-ment:revised recommendationsfor improvingthequality of reports of parallel group randomized trials. BMC Med Res Methodol.2001;1:2.
8.CappelleriG,AldegheriG,DanelliG,etal.Spinalanesthesia withhyperbariclevobupivacaineandropivacaineforoutpatient knee arthroscopy: a prospective, randomized, double-blind study.AnesthAnalg.2005;101:77---82.
9.ImbelloniLE, Gouveia MA, CarneiroAF, et al. Reducing the concentrationto0.4%enantiomericexcesshyperbaric levobupi-vacaine(s75:r25)providesunilateralspinalanesthesia.Study withdifferentvolumes.RevBrasAnestesiol.2012;62:654---64. 10.CasatiA,MoizoE,MarchettiC,etal.Aprospective,
random-ized,double-blind comparisonofunilateral spinalanesthesia withhyperbaricbupivacaine,ropivacaine,orlevobupivacaine foringuinalherniorrhaphy.AnesthAnalg.2004;99:1387---92. 11.LuckJF,FettesPD,WildsmithJA.Spinalanaesthesiafor
elec-tivesurgery:acomparisonofhyperbaricsolutionsofracemic bupivacaine,levobupivacaine,andropivacaine.BrJAnaesth. 2008;101:705---10.
12.Browner WS, Black D, Newman B, et al. Estimating sam-ple size and power. In: Hulley SB, Cummings SR, editors.
Designingclinicalresearch:anepidemiologicapproach. Balti-more:Williams&Wilkins;1988.p.139---50.
13.GlaserC,MarhoferP,ZimpferG, etal.Levobupivacaine ver-sus racemicbupivacaine forspinal anesthesia.AnesthAnalg. 2002;94:194---8.
14.Cuvas O, Er AE, Ongen E, et al. Spinal anesthesia for transurethral resection operations: bupivacaine versus lev-obupivacaine.MinervaAnestesiol.2008;74:697---701.
15.ErdilF,BulutS,DemirbilekS,etal.Theeffectsofintrathecal levobupivacaine andbupivacaine intheelderly.Anaesthesia. 2009;64:942---6.
16.MorrisonSG,DominguezJJ,FrascarolaP,etal.Acomparisonof theelectrocardiographiccardiotoxiceffectsofracemic bupiva-caine,levobupivacaine,andropivacaineinanesthetizedswine. AnesthAnalg.2000;90:1308---14.
17.Cox CR, Faccenda KA, Gilhooly C, et al. Extradural S(− )-bupivacaine: comparison with racemic RS-bupivacaine. Br J Anaesth.1998;80:289---93.
18.BardsleyH,GristwoodR,BakerH,etal.Acomparisonofthe cardiovasculareffectsoflevobupivacaineandrac-bupivacaine followingintravenousadministrationtohealthyvolunteers.Br JClinPharmacol.1998;46:245---9.
19.Atef H, El-Kasaby Ael-D, Omera M, et al. Optimal dose of hyperbaric bupivacaine 0.5% for unilateral spinal anesthesia duringdiagnostickneearthroscopy.MiddleEastJAnesthesiol. 2012;21:591---8.
20.PitkänenM,RosenbergPH.Localanaestheticsandadditivesfor spinalanaesthesia---characteristicsandfactorsinfluencingthe spreadanddurationoftheblock.BestPractResClin Anaesthe-siol.2003;17:305---22.
21.StienstraR,VeeringBT.Intrathecaldrugspread:isit control-lable?RegAnesthPainMed.1998;23:347---51,discussion384---7. 22.McLeod GA. Density of spinal anaesthetic solutions of bupi-vacaine, levobupivacaine, and ropivacaine with and without dextrose.BrJAnaesth.2004;92:547---51.
23.HockingG,WildsmithJA.Intrathecaldrugspread.BrJAnaesth. 2004;93:568---78.
24.Sönmez B, Akc¸ay M, Akc¸aboy EY, et al. Effects of uni-lateral spinal anesthesia with low dose bupivacaine and bupivacaine---fentanyl combination on recovery. J Clin Exp Invest.2011;2:22---9.
25.KuusniemiKS,PihlajamäkiKK,PitkänenMT.Alowdoseofplain orhyperbaricbupivacaineforunilateralspinalanesthesia.Reg AnesthPainMed.2000;25:605---10.
26.Whiteside JB, Burke D, Wildsmith JA. Spinal anaesthesia with ropivacaine 5mgml(−1) in glucose 10mgml(−1) or 50mgml(−1).BrJAnaesth.2001;86:241---4.
27.FettesPD,HockingG,PetersonMK,etal.Comparisonofplain andhyperbaricsolutionsofropivacaineforspinalanaesthesia. BrJAnaesth.2005;94:107---11.
28.Janik R, DickW, Stanton-Hicks MD. Effects ofdifferent glu-coseconcentrationsonspinalanaesthesiawithbupivacaineand tetracaine.EurJAnaesthesiol.1989;6:215---21.
29.BannisterJ,McClureJH,WildsmithJA.Effectofglucose concen-tration on the intrathecal spreadof 0.5% bupivacaine. Br J Anaesth.1990;64:232---4.
30.Sanansilp V, Trivate T, Chompubai P, et al. Clinical charac-teristicsofspinallevobupivacaine:hyperbariccomparedwith isobaricsolution.SciWorldJ.2012;2012:169076.
31.TsaiYJ,TsoHS,ChangCL.Spinalanesthesiawithbupivacainefor transurethralresectionofprostate:effectsofspecificgravity, volumeanddose.MaZuiXueZaZhi.1989;27:111---6.
32.Critchley LA, Morley AP, Derrick J.The influence ofbaricity onthehaemodynamiceffectsofintrathecalbupivacaine0.5%. Anaesthesia.1999;54:469---74.
34.Pittoni G, ToffolettoF,CalcarellaG,et al.Spinal anesthesia inoutpatientkneesurgery:22-gaugeversus25-gaugeSprotte needle.AnesthAnalg.1995;81:73---9.
35.BeardsleyD, Holman S, Gantt R, et al. Transientneurologic deficitafterspinalanesthesia:localanestheticmaldistribution
with pencil point needles? Anesth Analg. 1995;81: 314---20.