Brazilian
Journal
of
OTORHINOLARYNGOLOGY
www.bjorl.org
ORIGINAL
ARTICLE
Anatomical
study
of
minor
alterations
in
neonate
vocal
folds
夽
Adriano
Rezende
Silva,
Almiro
José
Machado
Júnior
∗,
Agrício
Nubiato
Crespo
DisciplineofOtorhinolaryngology,FaculdadedeCiênciasMédicas,UniversidadeEstadualdeCampinas(FCM-UNICAMP), Campinas,SP,Brazil
Received14June2013;accepted10November2013 Availableonline11June2014
KEYWORDS
Laryngealdiseases; Vocalfolds; Anatomy
Abstract
Introduction:Minorstructuralalterationsofthevocalfoldcoverarefrequentcausesofvoice abnormalities.Theymaybedifficulttodiagnose,andareexpressedindifferentmanners.Cases ofintracordalcysts,sulcusvocalis,mucosalbridge,andlaryngealmicro-diaphragmformthe groupofminorstructuralalterationsofthevocalfoldcoverinvestigatedinthepresentstudy. Theetiopathogenesisandepidemiologyofthesealterationsarepoorlyknown.
Objective: Toevaluatetheexistenceandanatomicalcharacterizationofminorstructural alter-ationsinthevocalfoldsofnewborns.
Methods:56larynxesexcisedfromneonatesofbothgenderswerestudied.Theywere exam-inedfresh,ordefrostedafterconservationviafreezing,underamicroscopeatmagnifications of25×and40×.Thevocalfoldswereinspectedandpalpatedbytwoexaminers,withtheaim offindingminorstructuralalterationssimilartothosedescribedclassically,andother unde-termined minorstructuralalterations. Laryngespresentingabnormalitiesweresubmitted to histologicalexamination.
Results:Sixcasesofabnormalitieswerefoundindifferentlarynges:one(1.79%)compatible withasulcusvocalisandfive(8.93%)compatiblewithalaryngealmicro-diaphragm.Nocases ofcystsormucosalbridgeswerefound.Theobservedabnormalitieshadcharacteristicssimilar tothosedescribedinotheragegroups.
Conclusion: Abnormalitiessimilartosulcusvocalisormicro-diaphragmmaybepresentatbirth. © 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:SilvaAR,MachadoJúniorAJ,CrespoAN.Anatomicalstudyofminoralterationsinneonatevocalfolds.BrazJ Otorhinolaryngol.2014;80:311---7.
∗Correspondingauthor.
E-mail:[email protected](A.J.MachadoJúnior).
http://dx.doi.org/10.1016/j.bjorl.2014.05.019
PALAVRAS-CHAVE
Doenc¸asdalaringe; Pregasvocais; Anatomia
Estudodealterac¸õesanatômicasmenoresempregasvocaisdeneonatos
Resumo
Introduc¸ão:Asalterac¸õesestruturaismínimas(AEM)dacoberturadaspregasvocaissãocausas frequentesdealterac¸ões vocais. Podemserde diagnósticodifícil, e expressam-sede modo variável.Ocistointracordal,osulcovocal,apontedemucosaeomicrodiafragamalaríngeo constituem ogrupo dasAEM da coberturadaspregas vocaispesquisadas nesteestudo.Sua etiopatogeniaeepidemiologianãosãobemconhecidas.
Objetivo:Avaliar a existência e a caracterizac¸ão anatômica das AEM em prega vocal de neonatos.
Métodos: Foramestudadas56laringesexcisadasdeneonatos,deambosossexos.Aslaringes foramexaminadas afrescoou descongeladasapós conservac¸ão por congelac¸ão,sob micro-scopiacomaumentode25e40×.Aspregasvocaisforaminspecionadasepalpadaspordois examinadores,comointuitodeencontrarAEMsemelhantesàsclassicamentedescritaseoutras indeterminadas.Aslaringescomalterac¸õesforamsubmetidasaexamehistológico.
Resultados: Foramencontradasseisalterac¸õesemlaringesdistintas:uma(1,79%)compatível comsulcovocalecinco(8,93%)compatíveiscommicrodiafragmalaríngeo.Nãoforam encon-trados cistos e pontes de mucosa. As alterac¸ões presentes apresentavam características semelhantesàsdescritasemoutrasfaixasetárias.
Conclusão:Alterac¸õessemelhantesaosulcovocaleaomicrodiafragmalaríngeopodemestar presentesaonascimento.
©2014Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
In the contemporary world, the human voice is increas-inglyusedin professionalrelationships,inthemedia,and in specific professions such as telemarketing operators, salesclerks, teachers, singers, actors, and others. Voice alterationscanresultfromvocalbehavior,throughincorrect orimproperuseofthevoice.Organicfactors,suchassmall anatomicalalterationsofthelarynx,mayalsopredisposeto dysphoniaandvocalfatigue.
These small anatomical alterations of the larynx were first mentioned in the literature by Arnold in 1958, who described them as ‘‘minor anatomical changes’’ of the larynx.1Whilestudyingpatientswithdysphonia,he classi-fiedsmallchangesofthevocalfolds,suchassulcusvocalis and asymmetries in a group, known as minor changes in the vocal folds.1 In 1994, Pontes and Behlau regrouped and classified these changes into four categories: laryn-gealasymmetries, incompleteposterior fusion, deviations inglottalproportions,andchangesinthevocalfoldcover, underthenameofminorstructuralalterations(MSAs).2,3
MSAsof thevocalfoldsaredefinedassmallchangesin configuration and structure of the larynx, which includes everything from simple anatomical variations to minor defectsthatdonothaveanimpactonvitallaryngeal func-tions, but that may or may not have an impact on the voice,accordingtotheirnature,location,extent,andvocal demands of the individual.3---6 These changes affect both menand women, adults and children, and include sulcus vocalis,epidermoidcysts,mucosalbridges,laryngeal micro-diaphragms,andvascularalterations.6---9
Therearenoepidemiologicalstudiesontheirprevalence inthepopulationand,sincetheyconstitutelesionsthatare
difficulttodiagnoseclinicallyandareexpressedatvarying intensities, it is estimatedthat theyareoften underdiag-nosed,butconstituteoneofthemaincausesofdysphonia intheadultpopulation.10---12
Even considering all current studies and technological advances,manyquestionsremainregardingMSAs,including thoserelatedtotheiretiology.13,14
Twotheories,thecongenitalandtheacquired,havebeen describedtoexplainitsetiopathogenesis.Thefirst hypoth-esis considers that these lesions are congenital.15 During laryngeal development,congenital anomalies arisingfrom changesinthefourthandsixthbranchialarchesgiveriseto thealterationsinvocalfoldcover.16AccordingtoBouchayer etal.cysts, sulcus vocalis,andmucosalbridgesareoften observedassociatedwithoneanother,andmightrepresent differentstagesofthesamecongenitalentity.17,18
The second hypothesis is that these alterations are acquired secondary to a chronic inflammatory process in responsetomicro-traumaanddiseasesaffectingthevocal folds.19 However, neither of the two theories completely explainstheoriginofMSAs.Therearenostudiesinthe lit-eratureonMSAsinnewborns,andthefindingofalterations inthisagerangecouldtestthehypothesisthattheymaybe congenital.Therefore,the aimof thisstudywastoverify thepresenceofMSAsinneonatallarynges.
Methods
Thisstudyincludedfreshlaryngesfromautopsiesof new-borns up to seven days of life, of both genders, and all thespecimenswerepreserved.Laryngesthathadapinkish color, withintact, bright,and homogeneousmucosa were considered well preserved. Macerated larynges and those withlacerations and severe alterations in normal mucosa colorwereclassifiedasinadequate.
Larynges of neonates whose time between death and autopsy was greater than 24h, those with prior tracheal intubationwithmacroscopicallyidentifiablemalformations, thosepreservedinformaldehyde,andthoseinpoor preser-vationconditionwereexcludedfromthesample.
A total of 70 larynges were evaluated; seven were excludedduetopreservationinformalin,fivedueto lacera-tionsinthevocalfoldscausedbyinadequateremovalduring necropsy, one due to prior intubation, and one showed macroscopicallyidentifiablelaryngeal malformation.Thus, 56 larynges were included in this study. Of the 56 laryn-gesassessed,23werefromamalechildand33werefrom afemalechild.Allwereexcisedfromstillbirths.The esti-matedgestationalagerangedfrom20to34weeks,witha meanof27.2weeks.Thetimebetweendeathandautopsy rangedfromtwoto24h.
Thelaryngeswereassessedfresh,orwerefrozen imme-diatelyafterautopsyandkeptunderrefrigerationat−8◦C foranalysiswithina30-dayperiod.Thefrozenlaryngeswere thawed at room temperature one hour beforethe analy-sis. Of the 56 larynges assessed, nine were fresh and 47 wereanalyzedafterfreezingandthawing.Thefreezingtime variedfromoneto30days.
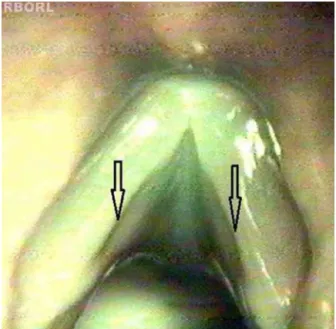
Forthephysicalexaminationofthevocalfoldsunderthe microscope, the sulcus vocalis wasconsidered as a longi-tudinal fusiform depression parallel tothe free borderof thevocal folds, ofvarying extension anddepth;the cyst, as a circumscribed submucosal nodular structure of vari-ablesizewithsimilarappearancetotheclassicallydescribed cyst;themucosalbridge,asamucosalhandleinsertedalong the vocal folds, and the laryngeal micro-diaphragm, as a smallmembrane between the twovocal folds, locatedin thecommissureandnotexceedingonethirdoftheirlength. CohenclassifiesastypeImembranesaffectinglessthan 35% of the glottal length.20 There is noprecise delimita-tionbetweenamicro-diaphragm andmembranesthat can beclassifiedasCohentypeI.Therefore,thisstudygrouped micro-diaphragmswithcharacteristicappearance(Fig.1b) and largerdiaphragms extending up to1/3 of the glottal length(CohentypeI---Fig.1a).
The examination of the larynges involved two stages: inspectionandinstrumentalpalpation.
Inspection
1 Larynges were arranged on the dissecting bench and inspectedunderlightmicroscopywith6×magnification, assessingtheupperportionofthevocalfolds,theanterior commissure, the posterior commissure, the ventricles, andthesupraglotticregion;
2 Laryngeswerethenopenedinthemidline,posteriorly,to exposethevocalfolds,aimingtopreservethesofttissues; 3 Amethodicalinspectionof theupperportion,free bor-der,andlowerportionofthevocalfoldswasperformed,
Epiglottis
A
B
LVF
LVF
RVF
RVF
Figure1 Laryngealmicro-diaphragm(arrow).(A)Shows lar-ynx52,and(B)showslarynx54.(LVF,leftvestibularfold;RVF, rightvocalfold).
as well as of the anterior commissure, under optical microscopywithmagnificationof25×and40×,whichwas alsorepeatedusingagreenlightfiltertohighlightvessels.
Instrumentalpalpation
Thevocalfoldswerepalpatedusingasurgicalbladewitha blunttipandasurgicaldissector.Palpationwasperformed bycarefullyslidingtheinstrumentalongtheupperportion, thefreeborder, thelowerportionof thevocal folds,and theanteriorcommissure,aimingtodetect changes inthe homogeneity,consistencyofshape,andsurfaceuniformity. Inspectionandpalpationwererepeatedafterinstillationof onedropofmethylenebluesolution,usedtohighlight pos-sible surface irregularities, throughthe deposition of the coloredliquid.
Laryngeswerealwaysevaluatedbytwoexaminers simul-taneously,comparingtheirobservationsandacceptingtheir commonopinion.
Uponinspectionandinstrumentalpalpation,thelarynges wereexaminedregarding:
a) thepresenceofMSAs;
b) the characterizationof alterations found,compared to thoseclassicallydescribed:sulcusvocalis,cysts,mucosal bridges,andlaryngealmicro-diaphragms;
c) the characterization of other alterations eventually found,otherthanthoseclassicallydescribed;
d) the location of alterations in the membranousportion ofthevocalfoldwhendividedintothreeequalpartsof thevocalprocessattheanteriorcommissure,asanterior, middle,andposteriorthirds(Fig.2);
e) numberofalterations;
f) associationbetweentwoormorealterations.
Figure2 Longitudinaldepression,similartothesulcusvocalis (arrows)observedatthesurgicalmicroscopeat40times mag-nification.
comparativepurposes.The resultswererecordedinforms that were specifically prepared for this study, containing gender, newborn weight, gestational age, time between deathand autopsy, cause of death, condition of the lar-ynx,preservationmethod,andschematicrepresentationof membranousportionofthevocalfolds andevaluated seg-ments.Theimagesofthelaryngesthatshowedalterations weredigitized and editedona computer,using theCorel Photo-Paintprogram,release10,applyingtheeffectto high-lighttherelief.
Laryngesthatshowedminoranatomicalalterationswere selectedforhistologicalstudy.Theywerefixedin10% for-malinforonetoeightweeksandembeddedinparaffin.The serialcross-sectionswerecarriedoutinthelongitudinalaxis ofthevocalfolds,with6-mthicknessandat1-mmintervals fromtheposteriortotheanteriorcommissure.Thesamples werestained withhematoxylin-eosin. The slidesobtained werestudiedtogetherwiththepathologist.
The histologicalanalysis of the sulcusvocalis usedthe criteria defined by Nakayama et al. (1994).21 The sulcus vocalis wasconsidered as an isolated invagination of the squamousepitheliuminthevocalfoldmucosa,withgreater
depth than the total epithelium thickness. Irregularities near the areas of transition of squamousepithelium with respiratoryepitheliumweredisregarded.Onlyinvaginations deeper thanthe epitheliumthicknesswereconsidered, in order to prevent incorrect interpretations resulting from artifactscausedbyslidepreparation.
Vocalcystwashistologicallyconsideredasaclosed cav-ity,locatedinthelaminapropriaofthevocalfoldmucosa, linedbystratifiedsquamousepitheliumandcontaining kera-tinizedmaterial.Mucosalbridge washistologicallydefined asabandofconnectivetissuelinedbystratifiedepithelium. Nohistologicalcriteriaintheliteratureforlaryngeal micro-diaphragmwerefound.Thus,theanatomicalaspectofthis alteration wasused asa diagnostic criterion. As this was adescriptiveandqualitativestudy,statisticalassessments were performed aspercentages. This study wasapproved bytheResearchEthicsCommitteeofFaculdadedeCiências MédicasofUNICAMP.
Results
Alterationswerefoundinsixlarynges(Table1). Thealterationswere:
a) Larynx9:longitudinal depressionalongthefreeborder ofbothvocalfolds,observedunderthemicroscopeasa broad, fusiform, darkened band, similar totype I sul-cus vocalis. The instrumental palpation showed relief alterationwhenthelongitudinaldepressionwaspalpated (Fig.2).
The distribution of the alterations found according to theirlocationisshowninTable2.ThedistributionofMSAs foundaccordingtogenderisshowninTable3.
The methylene blue solution was embedded, in most cases, on the laryngeal ventricles and anterior commis-sure, enhancing their anatomy. In larynx 9, the solution highlighted the sulcus vocalis,which had been previously visualized.Intheotheranalyzedlarynges,thesolutiondid nothelpintheidentificationofsurfacealterationsthathad notbeenpreviouslyvisualized.
Histologicalexamination corroborated the examination byinspectionandpalpationoflarynx9,whosehistological analysiswascompatiblewithtypeIsulcusvocalisintheleft vocalfold,accordingtothecriteriasuggestedbyNakayama etal.(1994)21 (Fig.3AandB).Thesulcusvocalisobserved
Table1 Numericaldistributionofminorstructuralalterationsfoundinsixlarynxes,regardingtypeandlocation,leftorright vocalfold,andcommissure(n=56).
ECL MBL SVL OTL CommissureMD ECR MBR SVR OTR
Larynx9 0 0 1 0 0 0 0 1 0
Larynx13 0 0 0 0 1 0 0 0 0
Larynx20 0 0 0 0 1 0 0 0 0
Larynx36 0 0 0 0 1 0 0 0 0
Larynx52 0 0 0 0 1 0 0 0 0
Larynx54 0 0 0 0 1 0 0 0 0
Total 0 0 1 0 5 0 0 1 0
Table2 Distributionofthesixalterationsfoundaccordingtotheirlocationintheanterior,middle,andposteriorthirdsofthe membranousportionofthevocalfolds,leftandright,anteriorcommissure,upperandlowerportion,andfreeborderofthe vocalfolds(n=56).
AnteriorL MiddleL PosteriorL Commissure AnteriorR MiddleR PosteriorR
Larynx9 Absent Freeborder Absent Absent A Freeborder A
Larynx13 Absent Absent Absent Present A A A
Larynx20 Absent Absent Absent Present A A A
Larynx36 Absent Absent Absent Present A A A
Larynx52 Absent Absent Absent Present A A A
Larynx54 Absent Absent Absent Present A A A
TOTAL 1 5 1
L,left;R,right.
Table3 Numericaldistributionofminorstructuralchanges foundregardinggender(n=56).
EC MB SV MD OT Total
Male 0 0 1 2 0 3
Female 0 0 0 3 0 3
Total 0 0 1 5 0 6
EC,epidermoidcyst;MB,mucosalbridge;SV,sulcusvocalis;MD, Micro-diaphragm;OT,others.
in the right vocal fold couldnot behistologically demon-strated.Fig.3Cshows thehistologicalaspect ofthevocal foldinnewborns.Noalterationassociationswerefound.
The alterationsimilarto typeI sulcus vocalisfound in larynx9wascharacterizedhistologicallybyaninvagination
Figure3 (A)Frontalhistologicalsectionoflarynx9,HE stain-ing.Inthedetail,(B)leftsulcusvocalis,indicatedbythearrow (upto20×). (C)Frontalhistologicalsectionofleft vocalfold
without alterations, inlarynx 2, which showed noalteration attheinspectionandinstrumental palpationexamination,HE staining,12×magnification.
of the stratified epithelium in the lamina propria, in the region of contact between the vocal folds, far from the regionof transitionbetweenthestratifiedandrespiratory epithelium,andcouldbeobservedonlyintheleftvocalfold inseveralsectionsperformedinthemiddlethirdofthevocal folds.Sectionsperformedintheanteriorandposteriorthirds showedinvaginationsinthesameregion,albeitsuperficial, whichdidnotmeetthecriteriaofNakayama etal.(1994) forsulcusvocalis.21
Of the fivediaphragms, four had the classic aspect of micro-diaphragmand onehadtheclassic aspectof Cohen typeIdiaphragm.
The histological study of the larynges with laryngeal micro-diaphragmswasnotsatisfactory,duetothetechnical difficultiesin obtaining perfect parallelismin longitudinal sections,necessary todemonstratethemicro-diaphragms. Nocysts and mucosalbridges were found in the larynges studied.
Discussion
Literature is still limited in relation to the presence of sulcusvocalis, mucosalbridge, cyst, andlaryngeal micro-diaphragm,andalthoughtherearesomestudiesdatingfrom thelate19thcenturyandearly 20thcentury,most ofthe publicationsdatefromthe1980stothepresentday.5Thisis duetothedevelopmentofdiagnostictechniques,withthe emergenceofflexibleendoscopy,andthedevelopmentand disseminationofstroboscopy.12Evenwiththetechnological advancesandtheintensificationofstudies,manyquestions remaintobeansweredaboutMSAsofthelarynx.
AccordingtoBouchayeretal.(1985),thereleaseofthe keratinizedcontentsoftheepidermoidcystonthefree bor-derof thevocal foldresultsinagroove,whileitsopening atthesuperiorandinferiorportionsofthevocalfoldresults intheformationofthemucosalbridge.Thishypothesiscan explainthe genesisof unilaterallesions,butitappears to beunlikelyinbilaterallesionsofsulcusvocalisormucosal bridge,asitwouldrequirethebilateralruptureofthecysts, symmetrically.18
TheacquiredtheorypresupposesthattheMSAsoriginate inresponsetoexternalstimuli.Thishypothesisisbasedon thefollowingobservations:lesionssuchasepidermoidcysts aremostlyfoundinthetransitionareabetweenthe ante-riorandtheposteriorthirdofthevocalfold,consideredthe segmentof greater functional activity of the vocal fold7; thepresenceofinflammatoryreactionaroundthelesions, suchassulcusvocalisandepidermoidcystsobservedinthe histologicalassessment18;thefrequentassociationofabuse and/ormisuseof thevoiceinpatients withtheselesions; thelateonsetofdysphoniaobservedinsomepatients8;and thepresenceofalterationssuchassulcusvocalisfoundin excisedlaryngesduringlaryngectomyinpatientswith malig-nant neoplasm of the larynx, suggesting that the chronic inflammatoryprocessrelatedtoneoplasmscanleadto sul-cusvocalisformation.18
Asshownintheliterature,neitherofthetwotheoriesof theetiopathogenesisofMSAsofthevocalfoldscanexplain theoriginofeachindividuallesion.Therearenoconclusive epidemiologicalstudies onMSAs inthepopulation. This is duetothe greatvariability of thesealterations andtheir presentation,astheyareoftennearlyasymptomatic. More-over,theirdiagnosisisalsodifficult.Themucusthatcovers thevocalfoldsflattensthesurfaceirregularitiesandmakes itdifficulttoidentifyalterations,requiringevaluationunder microscopyandpalpationofthevocalfoldstoidentifythe alteration.
Monday et al. stated that intracordal cysts are not unusual,althoughtheyarenotfrequentlymentionedinthe literature; but with the evolution of diagnostic methods, theselesionshavebecomemoreeasilyidentified.5Arnold, in1958,found12individualswithsulcusvocalisinagroup of 1250 adult soldiers withdysphonia. He commentsthat it is mucheasier to find individuals with laryngeal alter-ationsinagroupofdysphonicpatients,andconcludesthat statistical studies can be greatly influenced by selective factors.1
Milutinovic andVasiljevic (2001)found only11casesof sulcusvocalisin1550patientssubmittedtosurgery,which representsonly0.7%.Therefore,itispossiblethatalarge numberofMSAsarenotdiagnosedduringroutineendoscopic assessment.9
There are no studies in the literature on MSAs in neonates. The only reported case of cystic lesion was describedbySmithetal.in2000,whilereportingthe pres-enceof a cyst, described as having mucosal contentand therefore not compatible with an epidermoid cyst in a neonate.5Theembryologicaltreatisesarevaguein describ-ing the mechanisms of vocal fold formation,13 and most authors,althoughtheymentionthatthesulcusvocalis, epi-dermoid cysts, and mucosal bridge can be generated by defects of the fourth and sixth branchial arches, do not providethetheoreticalbasistosupportthishypothesis.5,8,18
The formation of the larynx is completed around the tenthgestationalweek;asthepresentsampleconsistedof neonates older than 20 weeksof gestation,stillborn, this fact practically eliminates the influence of external fac-tors, demonstratingthattheseresults areimportantfrom the etiopathogenic point of view, suggesting a congenital etiology.
In this study, the finding of sulcus vocalis in larynx 9, excisedfromaneonate,reinforcesthehypothesisthatthis alterationisofcongenitalorigin.Thisisthefirstdescription ofa sulcusvocalisinaneonate.Inthiscase, the possibil-itythatitwasapseudo-sulcusvocalis,whichconsistsofa grooved imagein themucosa throughout theentire vocal fold,resultingininfra-glotticedema,wasconsidered; how-ever, evidenceofthelesionandhistologicalfindingsruled outthispossibility.
Bouchayeretal.(1985)alreadysupportedthe congeni-taltheorytoexplaintheoriginofthesulcusvocalis.They suggestthattheyoriginatefromintracordalcysts,through theexteriorizationoftheircontent.18However,thepresent resultssuggestthattheselesionsmayalreadybepresentat birth,constitutinganindependententity,regardlessofthe epidermoidcyst.
Onedifficulty found in this study was the lack of his-tological standardization for MSAs in neonatevocal folds, asthe studiesonthe histologicalaspectsof theMSAs are rare and refer to adults.20 Hirano and Sato (1993),10 in theirhistologicalatlasofthehumanlarynx,reportthatthe layerstructureinneonatesdifferssignificantlyfromthatof adults.Thebiggestdifferenceisobservedinthelamina pro-priaofthemucosa.Inneonates,theentirelaminapropria isveryrudimentaryandhasadisarrayedaspect. It resem-blesthesuperficiallayerofthevocalfoldlaminapropriaof theadult,andconsistsin amorphoussubstance, scattered fibroblasts,collagenandelasticfibers.Therearefewer col-lagen fibers,andmorefibroblastsin thelaminapropriaof neonates than in the superficial lamina propriaof adults. Fromthismechanicalpointofview,theentiremucosacan beconsideredasandthevocalmuscleasbody.
Therefore,thehistologicalclassificationofsulcusvocalis in neonates,aswell asin adults,is notpossible. Because itisaninvaginationthatlacksadherencetothevocal mus-cle,theabnormalityinlarynx9wasclassifiedassuggestive oftypeIsulcusonlyintheleftvocalfold.Theauthorsdid notobservehistologicalchangesintherightvocalfold.This is probablydue to the difference in depth of the invagi-nation of theepithelium in thelamina propria. Thus, the importance of relating the macroscopic findings with the histologicalanalysisisalsoemphasized.
The studiesonsulcusvocalis,basedonautopsies,have verydifferentpatientpopulations.In1967,Ishiietal. iden-tified five cases of sulcus vocalis in 200 larynges excised at autopsy (2.5%).14 In 1976, Shin also found five cases of sulcus vocalis, but in 1200 excised larynges (0.42%). In 1994, Nakayama et al.21 reported 48% of histological alterationscompatiblewithsulcusvocalisinexcised laryn-ges of patients with cancer of the larynx. In 2000, Ming etal.reported thatamongthe 72laryngesexamined his-tologically,23%showedalterationscompatiblewithsulcus vocalis.15Inthepresentstudyof56neonatelarynges,sulcus vocaliswasfoundinone(1.78%).Similarstudieswithlarger samplesareneededtocomplementthisstudy.
The finding of MSAs in neonates reinforces the theory that they are congenital alterations. However, there are congenitallesionswithlateclinicalexpression,suchasthe thyroglossalcystandbranchialcyst.ThefactthatMSAswere notfoundin neonates,suchasmucosalbridgesandcysts, doesnotruleoutthepossibilitythatthesealterationsare congenital,astheymayhavealateclinical expression. It isalsopossiblethatthealterationsshowdistinct character-isticsatbirth andundergomodificationsover timedueto externalfactorsthatcausetissueinflammation. Thesmall samplesizedoesnotallowthecongenitaltheorytoberuled outforothertypesofMSAsthatwerenotfoundinthisstudy. There are few studies in the literature on laryngeal micro-diaphragms(Fordetal.1994).8However,thiswasthe mostfrequentalterationinthepresentstudy,occurringin 8.93%of56laryngesevaluated.Aspreviouslymentioned,it islikelythatthesechanges,aswellasotherMSAs,oftengo undiagnosed.AccordingtoWang(2000),thevocalfoldsare formedinadductionandaremediallyunitedbythe epithe-lial lamina; alterations in the cavitation process and cell necrosisoftheepitheliallamina,whichiscompletedaround the eighthweek ofthe gestational process,can generate smalldefectssuchaslaryngealmembranes.19Thefindingof fivelaryngeal micro-diaphragmsin the present study con-firmsthecongenitaloriginofthesealterations.
Conclusions
Based on the assessment of 56 excised larynges from neonates,it isconcludedthattherearealterationsin the vocalfoldsthatresembleMSAsdescribedinadultlarynges insomeoftheirforms,andwhentheyarestudiedbyoptical microscopy,theyshowthesamecharacteristicsasthosein adults.OftheMSAsselectedforthestudy,laryngeal micro-diaphragmandsulcusvocaliswerefound,andthefirstwas themostfrequentalteration.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Arnold GE. Dysplastic dysphonia: minor anomalies of the vocal cords causing persistent hoarseness. Laryngoscope. 1958;68:142---58.
2.PontesP,BehlauM.Disfonias funcionais.In:Lopes F,Campos CAH,editors.Tratadodeotorrinolaringologia.SãoPaulo:Roca; 1994.p.1014---26.
3.Pontes P,Behlau M,Gonc¸alvesI. Alterac¸ões estruturais mín-imas da laringe (AEM): considerac¸ões básicas. Acta AWHO. 1994;13:2---6.
4.Lee STS, Niimi S. Vocal fold sulcus. J Laryngol Otol. 1990;104:876---8.
5.Monday LA, Cornut G, Bouchayer M, Roch JB. Epidermoid cysts ofthevocal cords.Ann OtolRhinol Laryngol.1983;92: 124---7.
6.BernzMCN,HaasLJ,NemetzMA.Alterac¸õesestruturais míni-masmúltiplasesincrônicasdelaringeempacienteprofissional de voz falada: relato de caso. Rev Bras Otorrinolaringol. 1998;64:636---8.
7.Smith OD, Callana V, Harcourt J, Albert DM. Intracordal cyst in a neonate. Int J Pediatr Otorhinolaryngol. 2000;52: 277---81.
8.FordCN,BlessMD,GilchristWK,InagiK,KhidrA.Sulcusvocalis: arationalanalyticalapproach todiagnosisand management. AnnOtolRhinolLaryngol.1996;105:189---200.
9.MilutinovicZ,Vasiljevic J.Contributiontotheunderstanding oftheetiologyofvocalfoldcysts:afunctionalandhistologic study.Laryngoscope.1992;102:568---71.
10.HiranoM,TanakaS,TetsujiY,HibiS.Sulcusvocalis:functional aspects.AnnOtolRhinolLaryngol.1990;99:679---83.
11.HiranoM.Phonosurgical anatomyofthelarynx.In: FordCN, BlessDM,editors.Phonosurgery:assessmentandsurgical man-agement ofvoicedisorders.NewYork:RavenPress; 1991.p. 25---42.
12.HiranoM,ChuiwaK,TanakaS.Someaspectsofvocalfold bow-ing.AnnOtolRhinolLaryngol.1994;103:357---62.
13.Moore KL. Embriologia clínica. Rio de Janeiro: Guanabara Koogan;1995.p.74.
14.IshiiH,BabaT,KawabataI.Clinicalobservationsonthesulcus vocalis.JOtolaryngolJpn.1967;70:911---9.
15.Ming WH,Woo P,HsingWW,WenYS.Aclinicalclassification andhistopathologicalstudyofsulcusvocalis.EurArch Otorhi-nolaryngol.2000;257:466---8.
16.CrespoAN.FonocirurgianainfânciainNOVOROM[CD-ROM],vol. 1.SociedadeBrasileiradeOtorrinolaringologia;1999.
17.BouchayerM,CornutG,WitzigE,LoireR,RochJB,BastianRW. Epidermoidcysts,sulci,andmucosalbridgesofthetruevocal cord:areportof157cases.Laryngoscope.1985;95:1087---94.
18.BouchayerM,CornutG.Lesulcusglottidis.RevLaryngolOtol Rhinol.1987;108:391---2.
19.Wang RC. Three-dimensionalanalysis ofcricoarytenoid joint motion.Laryngoscope.1998;108Suppl.89:1---17.
20.CohenSR.Congenitalglottiswebsinchildren.Aretrospective reviewof51patients.AnnOtolRhinolLaryngol.1985;Suppl. 121:2---16.