Relationship between exercise capacity and quality
of life in adolescents with asthma*
Relação da capacidade de exercício com a qualidade de vida de adolescentes asmáticos
Renata Pedrolongo Basso, Mauricio Jamami, Ivana Gonçalves Labadessa, Eloisa Maria Gatti Regueiro, Bruna Varanda Pessoa, Antônio Delfino de Oliveira Jr,
Valéria Amorim Pires Di Lorenzo, Dirceu Costa
Abstract
Objective: To determine whether the quality of life of adolescents with asthma correlates with parameters obtained prior to and after the six-minute step test (6MST); spirometric results after the 6MST; and level of physical activity. Methods: Nineteen adolescents with asthma, ranging from 11-15 years of age, were assessed with spirometry, 6MST, the International Physical Activity Questionnaire (IPAQ), the Pediatric Asthma Quality of Life Questionnaire (PAQLQ), and the 10-point Borg category-ratio scale. Results: Sensation of dyspnea correlated negatively with the total PAQLQ score (r = −0.54) and with the scores of its activity limitation (AL) and symptoms domains (r = −0.64 and r = −0.63, respectively), leg fatigue also correlating negatively with those same domains (r = −0.49 and r = −0.56, respectively). The total IPAQ score correlated with the total PAQLQ score (r = 0.47) and with the PAQLQ AL domain (r = 0.51); IPAQ time spent walking correlated with the PAQLQ symptoms domain (r = 0.45); and IPAQ time spent in vigorous activity correlated with the AL domain (r = 0.50). In the regression analysis, only sensation of dyspnea remained significantly correlated with the total PAQLQ score and the PAQLQ AL domain; leg fatigue remained significantly correlated with the symptoms domain. Conclusions: Higher levels of physical activity indicate better quality of life, as do lower perception of dyspnea and less leg fatigue. The 6MST proved to be a viable option for evaluating exercise capacity in adolescents with asthma, because it reflects the discomfort that asthma causes during activities of daily living.
Keywords: Asthma; Quality of life; Dyspnea.
Resumo
Objetivo: Determinar se parâmetros obtidos antes e após a realização do teste do degrau de seis minutos (TD6), respostas espirométricas após o TD6 e o nível de atividade física se correlacionam com a qualidade de vida de adolescentes asmáticos. Métodos: Foram avaliados 19 adolescentes asmáticos, com idades variando de 11-15 anos, por meio de espirometria, TD6, International Physical Activity Questionnaire (IPAQ, Questionário Internacional de Atividade Física), Questionário sobre a Qualidade de Vida na Asma Pediátrica (QQVAP) e escala CR10 de Borg. Resultados: Houve correlações negativas entre sensação de dispneia e pontuação total do QQVAP (r = −0,54) e de seus domínios limitação nas atividades (LA) e sintomas (r = −0,64 e r = −0,63, respectivamente), assim como entre fadiga nos membros inferiores (MMII) e os mesmos domínios (r = −0,49 e r = −0,56, respectivamente). O escore total do IPAQ correlacionou-se com a pontuação total do QQVAP (r = 0,47) e o domínio LA (r = 0,51), enquanto o tempo de caminhada correlacionou-se com o domínio sintomas (r = 0,45), e o tempo de atividade intensa correlacionou-se com o domínio LA (r = 0,50). Na análise de regressão, somente a sensação de dispneia associou-se significativamente ao escore total e o domínio limitação nas atividades do QQVAP, e o mesmo ocorreu entre a fadiga dos MMII e o domínio sintomas. Conclusões: Quanto maior for o nível de atividade física e menor for a dispneia e a fadiga nos MMII, melhor é a qualidade de vida. O TD6 mostrou-se uma opção na avaliação da capacidade ao exercício desses indivíduos por refletir o incômodo que a asma provoca na prática das atividades da vida diária.
Descritores: Asma; Qualidade de vida; Dispneia.
* Study carried out at the Universidade Federal de São Carlos – UFSCar, Federal University of São Carlos – São Carlos, Brazil. Correspondence to: Renata Pedrolongo Basso. Rodovia Washington Luiz, km 235, Laboratório de Espirometria e Fisioterapia Respiratória – DFisio, CEP 13565-905, São Carlos, SP, Brasil.
Tel. 55 16 3351-8343. E-mail: renata.fisio@gmail.com
Financial support: This study received financial support from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES, Office for the Advancement of Higher Education).
Introduction
Asthma is a chronic inflammatory disease that can have a considerable impact on the daily lives of adolescents.(1) Asthma is characterized by
recurrent episodes of wheezing, chest tightness, breathlessness, and cough due to a variety of stimuli, the most common of which is physical
exercise.(2,3) Exercise-induced bronchospasm
(EIB) occurs in 40-90% of all individuals with
asthma(3) and can reduce exercise tolerance, leading
individuals with asthma to adopt a more sedentary
lifestyle than that adopted by those without.(4)
Asthma severity and reduced exercise capacity can affect the social, educational, and emotional lives of children and adolescents with asthma, the quality of life of such individuals being significantly worse than that of those without asthma.(5,6) Therefore, it is important to identify
and address the factors affecting the quality of life of children and adolescents with asthma in order
to provide comprehensive asthma treatment.(7)
Clinical parameters such as symptoms, frequency of medication use, and airflow measurements are not strongly related to quality of life and therefore fail to provide a complete picture of how children and adolescents with asthma perceive the disease and of how asthma limits
their activities of daily living.(7,8) Therefore,
it important to determine whether objective measurements of exercise capacity reflect the impact of asthma on quality of life in order to evaluate such individuals more comprehensively and prescribe a rehabilitation program suited to their limitations and disease severity.
Various tests have been used in order to assess functional capacity in patients with lung disease.
(9-12) However, because submaximal exercise tests
are safe, easy to apply, and readily available for routine clinical assessment and because they can predict the ability to perform activities of
daily living,(13) submaximal exercise testing has
been suggested as an option to evaluate asthma
patients, given that it can detect EIB and aid in
the early diagnosis of physical activity limitation.
(9,10) However, we found no studies evaluating
whether submaximal exercise responses as elicited by a submaximal test such as the six-minute step test (6MST) reflect the impact of asthma on quality of life.
Therefore, the primary objective of the present study was to determine whether the quality of life of adolescents with asthma correlated with
parameters obtained prior to and after the 6MST (i.e., physical performance, cardiorespiratory responses, sensation of dyspnea, and leg fatigue) and with spirometric results after the 6MST. A secondary objective was to determine whether the quality of life of those adolescents correlated with their level of physical activity.
Methods
The present study was conducted between
March and October of 2010 at the Federal
University of São Carlos Respiratory Therapy Unit, located in the city of São Carlos, Brazil. We evaluated 19 adolescents with asthma who were recruited through active community surveillance
and who were in the 11-15 year age bracket. The
parents or legal guardians of the adolescents who participated in the present study gave written informed consent, and the study was approved by the local research ethics committee (Ruling no. 119/2008).
We included adolescents with a diagnosis of asthma (a clinical diagnosis, a spirometric diagnosis, or both), the diagnosis having been confirmed by pre- and post-bronchodilator spirometry performed
under the supervision of a pulmonologist.(14)
The participants were clinically stable, having
had no respiratory infections or asthma attacks for at least three weeks. We excluded patients
who were clinically unstable because of acute
respiratory infections or asthma attacks in the three weeks preceding the evaluation, as well
as those with other respiratory diseases, heart
disease, rheumatic disease, musculoskeletal disease,
orthopedic disease, or neurological sequelae that prevented them from performing the proposed tests.
Initially, the adolescents were interviewed. During the interview, an anamnesis form and the short version of the International Physical
Activity Questionnaire (IPAQ)(15) were completed
in order to characterize the level of physical activity, the Pediatric Asthma Quality of Life
Questionnaire (PAQLQ)(16) being also completed.
Subsequently, the participants underwent general physical examination and respiratory system examination, as well as receiving instructions regarding the proposed protocol.
On the same day, the participants underwent spirometry with a portable spirometer (EasyOne™;
ndd Medizintechnik AG, Zurich, Switzerland).
and reproducibility criteria were in accordance
with the American Thoracic Society/European
Respiratory Society guidelines.(17) We obtained
three technically acceptable curves for slow vital capacity, FVC, and maximal voluntary ventilation. The values obtained were compared with those
proposed by Polgar & Promadhat.(18)
For functional capacity evaluation, the 6MST was performed on a different day.
The 6MST was performed in accordance with
methods described elsewhere.(19) At the end of
every minute, standard phrases of encouragement were provided. At the end of every two minutes,
SpO2 was measured with a pulse oximeter (Model
2500; Nonin Medical Inc., Minneapolis, MN, USA), HR was measured with an HR monitor
(Model Vantage NV™ 1901001; Polar, Kempele,
Finland), and sensation of dyspnea and leg fatigue were measured by the 10-point Borg category-ratio scale. Those measurements, together with measurements of systolic blood pressure, diastolic blood pressure, and RR, were performed at rest and immediately after the test, as well as at recovery minutes 1, 3, and 6.
In addition to the abovementioned measurements, FVC maneuvers were performed at various time points: before the test; immediately after the test; and within 5, 10, 15, and 30 minutes after the test, the better of two maneuvers being selected. The participants performed FVC maneuvers at post-test minutes 15 and 30 only
if the FEV1 at post-test minute 10 decreased by ≥
15% in comparison with the pre-test FEV1 value. (9,20) Performance on the 6MST was determined by
the total number of times that the individual being tested went up and down the step, and maximal HR (HRmax) was calculated by the following
formula: HRmax = 210 − (0.65 × age in years).(21)
For the present study, we chose to use the short version of the IPAQ, previously translated
to Portuguese and validated for use in Brazil.(15)
The questionnaire consists of 7 open questions, the answers to which provide information that
allows us to estimate the weekly time spent in
different activities. The questions address the duration and frequency of moderate to vigorous
activities and the time spent walking in the previous week. On the basis of the information
obtained, the IPAQ allows us to classify individuals as sedentary, insufficiently active, active, or very active.(15)
We also used the Brazilian Portuguese-language version of the PAQLQ, previously
adapted and validated for use in Brazil.(16) The
PAQLQ was developed for children and adolescents
in the 7-17 year age bracket and consists of
23 questions distributed into three domains: symptoms, comprising 10 questions; activity limitation, comprising 5 questions; and emotional function, comprising 8 questions. Children are
asked to report how they felt in the previous week and to answer each of the 23 questions
on a 7-point scale (7 = not bothered at all and 1 = extremely bothered). The score for each of the PAQLQ domains is calculated by summing the scores for each question and dividing the sum by the total number of questions, the total PAQLQ score being calculated by summing the individual domain scores.
In the statistical analysis, we used the
Shapiro-Wilk test in order to evaluate the normality
of the data. In addition, we used descriptive statistics for variables with parametric distribution,
the data being expressed as mean ± standard
deviation, and for those with nonparametric distribution, the data being expressed as median (interquartile range). Subsequently, we used Pearson’s correlation coefficient (for variables with parametric distribution) or Spearman’s correlation coefficient (for variables with nonparametric
distribution) and performed backward multiple
linear regression analysis of correlated variables in order to find the independent variable determining quality of life, the PAQLQ scores being therefore considered dependent variables.
We used the Statistical Package for the Social
Sciences, version 13.0 (SPSS Inc., Chicago, IL, USA). The power of the study was calculated using the GraphPad StatMate software, version 2.0 for Windows (GraphPad Software Inc., San Diego, CA, USA), and the sample corresponded
to a power of 80% for the study variables, in
accordance with a pilot study involving healthy adolescents. The level of significance was set
at 5%.
Results
We evaluated 19 asthma patients (15 boys
and 4 girls), who were classified as having mild
intermittent asthma or mild persistent asthma in accordance with the Global Initiative for Asthma criteria.(14) All of the patients were clinically stable.
inhaled corticosteroids regularly (mean dose, 200
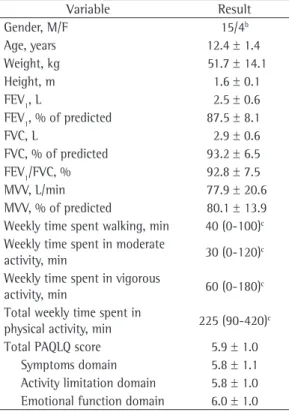
µg) and 14 used a β2 agonist for symptom relief. Table 1 shows the following: demographic, anthropometric, and spirometric data at baseline; the level of physical activity, as determined by
the time (in min) spent walking, the time (in
min) spent in moderate activity, the time (in min) spent in vigorous activity, and the total time spent in physical activity in the previous
week; the scores for each PAQLQ domain; and
the total PAQLQ scores. The level of physical activity in the study sample was determined on
the basis of the answers to the IPAQ.(15) Of the
19 participants, 7 were classified as insufficiently active, 7 were classified as active, and 5 were classified as very active.
There were no significant differences between
pre-test FEV1 and post-test FEV1 (as measured immediately after the test and at post-test minutes
5, 10, and 15), and post-test FEV1 did not decrease by ≥ 15% in comparison with pre-test FEV1,
which would have characterized EIB.(20) Of the
19 participants, 3 had to stop the 6MST for approximately 20 s, on average, because of leg fatigue, resuming the test.
Neither the total PAQLQ score nor the PAQLQ domain scores correlated with the total number of times that the individual being tested went up and down the step during the 6MST or with pre- or post-test RR, HR, systolic blood pressure,
diastolic blood pressure, and FEV1. The values obtained at the end of the 6MST are shown in Table 2. Sensation of dyspnea correlated negatively with the total PAQLQ score and with the scores of the PAQLQ activity limitation and symptoms domains, leg fatigue also correlating negatively with those same domains (Table 3).
Regarding the impact of the level of physical activity on quality of life, we found that the time spent in physical activity correlated positively with the total PAQLQ score and the PAQLQ activity
limitation domain. Likewise, the time spent walking correlated with the PAQLQ symptoms
domain, and the time spent in vigorous activity correlated with the PAQLQ activity limitation domain (Table 3).
In the multiple regression analysis, only sensation of dyspnea remained significantly
correlated with the total PAQLQ score (β = −0.27;
p = 0.003) and the PAQLQ activity limitation
domain (β = −0.33; p ≤ 0.001), sensation of
dyspnea having explained 42% of the variation in the total PAQLQ score and 63% of the variation
in the activity limitation domain score; leg fatigue remained significantly correlated with the PAQLQ
symptoms domain (β = −0.22; p = 0.003), having
Table 1 - Demographic variables, anthropometric variables, spirometric variables, level of physical activity, and quality of life questionnaire scores for 19 adolescents with mild intermittent asthma or mild persistent asthma.a
Variable Result
Gender, M/F 15/4b
Age, years 12.4 ± 1.4
Weight, kg 51.7 ± 14.1
Height, m 1.6 ± 0.1
FEV1, L 2.5 ± 0.6
FEV1, % of predicted 87.5 ± 8.1
FVC, L 2.9 ± 0.6
FVC, % of predicted 93.2 ± 6.5
FEV1/FVC, % 92.8 ± 7.5
MVV, L/min 77.9 ± 20.6
MVV, % of predicted 80.1 ± 13.9
Weekly time spent walking, min 40 (0-100)c
Weekly time spent in moderate
activity, min 30 (0-120)c
Weekly time spent in vigorous
activity, min 60 (0-180)
c
Total weekly time spent in
physical activity, min 225 (90-420)c
Total PAQLQ score 5.9 ± 1.0
Symptoms domain 5.8 ± 1.1
Activity limitation domain 5.8 ± 1.0 Emotional function domain 6.0 ± 1.0
MVV: maximal voluntary ventilation; and PAQLQ: Pediatric Asthma Quality of Life Questionnaire. aData expressed as
mean ± SD, except where otherwise indicated. bData expressed
as n/n. cData expressed as median (interquartile range).
Table 2 - Physical performance, sensation of dyspnea, leg fatigue, respiratory variables, and cardiovascular variables at the end of the six-minute step test.a
Variable Value
T-6MST 146.6 ± 30.4
SpO2, % 97 (96-97)
RR, breaths/min 21.0 ± 2.7
HR, bpm 148.5 ± 21.6
HRmax, % 73.0 ± 10.0
SBP, mmHg 120 (110-130)
DBP, mmHg 70 (60-80)
Borg scale (dyspnea) 2.0 (0.8-4.3) Borg scale (leg fatigue) 3.0 (1.0-4.3)
T-6MST: total number of times that the individual being tested went up and down the step during the six-minute step test; HRmax: maximal HR; SBP: systolic blood pressure; and DBP: diastolic blood pressure. aData expressed as
explained 37% of the variation in the symptoms
domain score.
Discussion
The objective of the present study was to determine whether the quality of life of adolescents with asthma correlated with physical performance, cardiorespiratory responses, sensation of dyspnea, leg fatigue, and spirometric results after the 6MST, as well as with the level of physical activity. The 6MST has been used and recommended as a method for evaluating patients with lung
disease.(12) Because it is a submaximal exercise
test, the 6MST assesses functional capacity in terms of the ability to perform activities of daily
living.(12,13) The 6MST was found to be a test of
moderate intensity for the asthma patients in the present study, having allowed the participants
to achieve 73% of their HRmax (Table 2) and
having caused, on average, mild dyspnea and moderate leg fatigue or pain, although some of the participants experienced severe dyspnea and leg fatigue or pain.
In the present study, the 6MST was self-paced, meaning that the stepping rate did not remain constant throughout the test. Therefore, a high
(> 80%) HR was not achieved or maintained
throughout the test. This prevented the occurrence
of EIB despite mouth breathing having contributed
to turning the inhaled air drier and colder, which
can cause EIB.(11,20)
In one study,(9) a step test performed at an
intensity that was sufficient to maintain an
HR > 150 bpm for 5 min caused EIB. In the
present study, however, the 6MST was self-paced in order to be as functional as possible and reflect possible limitations in the ability to perform activities of daily living.
In the present study, we found no correlation between quality of life and cardiorespiratory
responses to the 6MST or between quality of life and spirometric results after the 6MST. This finding is consistent with those of studies showing
a weak correlation between clinical variables
and quality of life in asthma patients.(7,8) Such
a weak correlation is due to the multifaceted
nature of quality of life, which has physical, emotional, and social aspects and is therefore difficult to assess by means of objective parameters. However, sensation of dyspnea and leg fatigue during the 6MST, which are subjective sensations, correlated with the symptoms domain score and the activity limitation domain score, dyspnea having also correlated with the total PAQLQ score. A more intense perception of dyspnea and a greater degree of leg fatigue during the 6MST translated to worse quality of life in our sample of adolescents with asthma.
It is of note that the questions on the quality of life questionnaire used in the present study
refer to the previous week, and, because the study
participants were clinically stable, the score was high for all domains, especially the emotional function domain. This result is consistent with those of a study showing that patients with controlled asthma have a better quality of life than
do those with uncontrolled asthma.(22) However,
although the mean score for the activity limitation domain and that for the symptoms domain were equal, the activity limitation domain showed the lowest scores; this constitutes evidence that the asthma patients had lower exercise tolerance, which affected their quality of life.(4-6)
Studies have shown that physical activity improves the quality of life of asthma patients.
(23-25) Therefore, we quantified the level of physical
activity and classified the adolescents under study in accordance with their level of physical activity, having subsequently determined whether the level of physical activity correlated with quality of life.
Table 3 - Correlations of the quality of life questionnaire with the six-minute step test variables and with the level of physical activity.
Variable PAQLQ
Total Symptoms AL EF
Borg scale (dyspnea) −0.54* −0.63* −0.64* −0.39
Borg scale (leg fatigue) −0.41 −0.56* −0.49* −0.21
Weekly time spent walking, min 0.44 0.45* 0.37 0.34
Weekly time spent in moderate activity, min 0.22 0.08 0.22 0.17
Weekly time spent in vigorous activity, min 0.30 0.31 0.50* 0.05
Total weekly time spent in physical activity, min 0.47* 0.33 0.51* 0.38
PAQLQ: Pediatric Asthma Quality of Life Questionnaire; AL: activity limitation domain; and EF: emotional function domain.
None of the adolescents under study were classified as sedentary, most having been classified as active or insufficiently active.(15) This, together
with the fact that the adolescents were clinically stable, might have contributed to the high scores obtained on the quality of life questionnaire. In addition, we found positive correlations between the time spent in physical activity and the score on the questionnaire, a finding that is consistent
with those of studies(23-25) showing that physical
activity is beneficial to the quality of life of asthma patients. However, our regression analysis
showed that the weekly time spent in physical
activity was not an independent predictor of quality of life, although sensation of dyspnea and leg fatigue were, underscoring the importance of functional assessment of asthma patients in order to evaluate their symptoms and limitations. The correlations of sensation of dyspnea and leg fatigue with the PAQLQ variables, together with our regression analysis, showed that the sensation of dyspnea and leg fatigue reported at the end of the 6MST reflected the extent to which patients are bothered (term used in the PAQLQ) by asthma and its symptoms, such as cough, fatigue, breathlessness, and chest tightness, and the extent to which the disease limits their
ability to perform activities of daily living. Our
findings are also consistent with those of studies showing that sensation of dyspnea is one of the major factors limiting the ability of asthma
patients to perform physical activity.(4,26)
One limitation of the present study is the
fact that the study sample consisted exclusively of adolescents with mild intermittent asthma or mild persistent asthma. Had we evaluated a more diverse sample of asthma patients, the results of the present study might be generalizable. However, our results are important because those are the most prevalent types in the spectrum of asthma severity.
The quality of life of adolescents with mild intermittent asthma or mild persistent asthma correlates with the level of physical activity, as well as with sensation of dyspnea and leg fatigue during the 6MST. These subjective sensations reflect the extent to which asthma symptoms limit the ability of patients to perform moderate to vigorous activities of daily living, therefore reflecting the impact of asthma on the quality of life of adolescents. In addition, given the relationship between exercise capacity and
quality of life and the importance of the latter for comprehensive asthma treatment, the 6MST is a viable option for evaluating exercise capacity in asthma patients in clinical practice.
References
1. Walker J, Winkelstein M, Land C, Lewis-Boyer L, Quartey
R, Pham L, et al. Factors that influence quality of life in rural children with asthma and their parents. J Pediatr
Health Care. 2008;22(6):343-50.
2. Sociedade Brasileira de Pneumologia e Tisiologia. V Diretrizes brasileiras para o manejo da asma. J Bras
Pneumol. 2006;32(Suppl 7):S447-S474.
3. Rubin AS, Pereira CA, Neder JA, Fiterman J, Pizzichini MM. Hiperresponsividade brônquica. J Pneumol. 2002;28(Suppl.3):S101-S121.
4. Pianosi PT, Davis HS. Determinants of physical fitness in
children with asthma. Pediatrics. 2004;113(3 Pt 1):e225-9.
5. van Veldhoven NH, Vermeer A, Bogaard JM, Hessels MG,
Wijnroks L, Colland VT, et al. Children with asthma and
physical exercise: effects of an exercise programme. Clin
Rehabil. 2001;15(4):360-70.
6. Everhart RS, Fiese BH. Asthma severity and child quality
of life in pediatric asthma: a systematic review. Patient
Educ Couns. 2009;75(2):162-8.
7. Juniper EF. How important is quality of life in pediatric
asthma? Pediatr Pulmonol Suppl. 1997;15:17-21. 8. Juniper EF, Wisniewski ME, Cox FM, Emmett AH, Nielsen
KE, O’Byrne PM. Relationship between quality of life and clinical status in asthma: a factor analysis. Eur Respir J. 2004;23(2):287-91.
9. Feinstein RA, Hains CS, Hemstreet MP, Turner-Henson A, Redden DT, Martin B, et al. A simple “step-test” protocol for identifying suspected unrecognized
exercise-induced asthma (EIA) in children. Allergy Asthma Proc.
1999;20(3):181-8.
10. Battilani VM, Sologuren MJJ, Gastaldi AC. Crianças com asma leve caminham menor distância que crianças não
asmáticas, no mesmo período de tempo. Rev Bras Educ Fís Esp. 2004;18(1):117-24.
11. Souza AC, Pereira CA. Bronchial provocation tests using methacholine, cycle ergometer exercise and free running in children with intermittent asthma [Article in Portuguese]. J Pediatr (Rio J). 2005;81(1):65-72.
12. Dal Corso S, Duarte SR, Neder JA, Malaguti C, de Fuccio MB, de Castro Pereira CA, et al. A step test to assess exercise-related oxygen desaturation in interstitial lung
disease. Eur Respir J. 2007;29(2):330-6.
13. Li AM, Yin J, Yu CC, Tsang T, So HK, Wong E, et al. The six-minute walk test in healthy children: reliability and validity. Eur Respir J. 2005;25(6):1057-60.
14. Global Initiative for Asthma [homepage on the Internet]. Bethesda: Global Initiative for Asthma [cited 2012 Sep 9]. Global Strategy for Asthma Management and Prevention. Update 2007. Available from: http://www.ginasthma.
org/documents/5/documents_variants/34
15. Matsudo S, Araújo T, Marsudo V, Andrade D, Andrade E, Oliveira L, et al. Questionário Internacional de Atividade Física (IPAQ). Estudo de validade e reprodutibilidade no
Brasil. Rev Bras Ativ Fís Saúde. 2001;6(2):5-18. 16. La Scala CS, Naspitz CK, Solé D. Adaptation and validation
(PAQLQ) in Brazilian asthmatic children and adolescents.
[Article in Portuguese] J Pediatr (Rio J). 2005;81(1):54-60.
17. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur
Respir J. 2005;26(2):319-38.
18. Polgar C, Promadhat V. Pulmonary Function Testing in Children: Techniques and Standards. Philadelphia: Sanders; 1971.
19. Basso RP, Jamami M, Pessoa BV, Labadessa IG, Regueiro
EMG, Di Lorenzo VAP. Avaliação da capacidade de
exercício em adolescentes asmáticos e saudáveis. Rev
Bras Fisioter. 2010:14(3):252-8.
20. Neder JA, Nery LE. Fisiologia clínica do exercício. Teoria
e prática. São Paulo: Artes Médicas; 2003.
21. Clark CJ, Cochrane LM. Assessment of work performance
in asthma for determination of cardiorespiratory fitness
and training capacity. Thorax. 1988;43(10):745-9.
22. Pereira ED, Cavalcante AG, Pereira EN, Lucas P, Holanda
MA. Asthma control and quality of life in patients
with moderate or severe asthma. J Bras Pneumol. 2011;37(6):705-11.
23. Basaran S, Guler-Uysal F, Ergen N, Seydaoglu G, Bingol-Karakoç G, Ufuk Altintas D. Effects of physical exercise on
quality of life, exercise capacity and pulmonary function in children with asthma. J Rehabil Med. 2006;38(2):130-5.
24. Fanelli A, Cabral AL, Neder JA, Martins MA, Carvalho
CR. Exercise training on disease control and quality of life in asthmatic children. Med Sci Sports Exerc. 2007;39(9):1474-80.
25. Gonçalves RC, Nunes MP, Cukier A, Stelmach R, Martins MA, Carvalho CR. Efeito de um programa de condicionamento
físico aeróbio nos aspectos psicossociais, na qualidade de vida, nos sintomas e no óxido nítrico exalado de portadores de asma persistente moderada ou grave. Rev Bras Fisioter. 2008;12(2):127-35.
26. Cavalcante TM, Diccini S, Barbosa DA, Bittenourt AR. The use of Borg’s modified scale in asthma crises. Acta
Paul Enferm. 2008;21(3):466-73.
Sobre os autores
Renata Pedrolongo Basso
Substitute Professor. Department of Physical Therapy, Universidade Federal de São Carlos – UFSCar, Federal University of São Carlos – São Carlos, Brazil.
Mauricio Jamami
Adjunct Professor. Graduate Course in Physical Therapy and Graduate Program in Physical Therapy, Universidade Federal de São Carlos – UFSCar, Federal University of São Carlos – São Carlos, Brazil.
Ivana Gonçalves Labadessa
Master’s in Physical Therapy. Universidade Federal de São Carlos – UFSCar, Federal University of São Carlos – São Carlos, Brazil.
Eloisa Maria Gatti Regueiro
Professor. Undergraduate and Graduate Courses in Physical Therapy, UNIFAFIBE University Center, Bebedouro, Brazil, and Claretian University Center, Batatais, Brazil.
Bruna Varanda Pessoa
PhD in Physical Therapy. Universidade Federal de São Carlos – UFSCar, Federal University of São Carlos – São Carlos, Brazil.
Antônio Delfino de Oliveira Jr
Preceptor. Undergraduate Medical Course, Universidade Federal de São Carlos – UFSCar, Federal University of São Carlos – São Carlos, Brazil.
Valéria Amorim Pires Di Lorenzo
Adjunct Professor. Graduate Course in Physical Therapy and Graduate Program in Physical Therapy, Universidade Federal de São Carlos – UFSCar, Federal University of São Carlos – São Carlos, Brazil.
Dirceu Costa