www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Parotid
gland
tumors:
a
retrospective
study
of
154
patients
夽
,
夽夽
Gerson
Schulz
Maahs
a,∗,
Paula
de
Oliveira
Oppermann
b,
Lucas
Gerhard
Peter
Maahs
a,
Geraldo
Machado
Filho
a,
André
Dajori
Ronchi
aaUniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
bDivisionofOtorhinolaryngology,HospitaldeClínicasdePortoAlegre,PortoAlegre,RS,Brazil
Received23March2014;accepted6July2014 Availableonline30March2015
KEYWORDS
Parotidneoplasms; Parotidgland; Salivaryglands
Abstract
Introduction:Benign tumors of the parotid gland comprise the majority of salivary gland tumors.
Objective: Toreviewtheclinicalcharacteristicsofparotidglandtumorssubmittedtosurgical treatmentbythesamesurgeon.
Methods:Retrospectivestudy with154patients who hadparotid glandtumors.Clinical and histologicaldata,typeofsurgery,andcomplicationswereassessedanddescribed.
Results:Themainmanifestationwasamasswithamedianevolutionof12monthsforbenign tumors andfivemonths formalignanttumors.Ultrasonographywasthemostfrequent com-plementary exam. Pleomorphicadenomawas themost commonofthe benigntumors, and mucoepidermoidcarcinomawasthemostfrequentmalignanttumor.Superficialparotidectomy withpreservationofthefacialnervewasthemostcommonsurgicalprocedureandreversible paresisofbranchesofthefacialnervewasthemostcommoncomplication.
Conclusions: Pleomorphicadenomaisthemostcommonparotidglandtumorandsuperficial parotidectomy with preservation of the facial nerve is the most common and appropriate treatmentformostlow-morbiditytumors.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:MaahsGS,OppermannPO,MaahsLGP,MachadoFilhoG,RonchiAD.Parotidglandtumors:aretrospective studyof154patients.BrazJOtorhinolaryngol.2015;81:301---6.
夽夽
Institution:UniversidadeFederaldoRioGrandedoSul(UFRS),PortoAlegre,RS,Brazil.
∗Correspondingauthor.
E-mail:[email protected](G.S.Maahs).
http://dx.doi.org/10.1016/j.bjorl.2015.03.007
PALAVRAS-CHAVE
Neoplasias parotídeas; Glândulaparótida; Glândulassalivares
Tumoresdeglândulaparótida:estudoretrospectivode154pacientes
Resumo
Introduc¸ão:Ostumoresdeparótidasãofrequentementedenaturezabenignaecorrespondem àmaioriadostumoresdeglândulassalivares.
Objetivo:Revisarascaracterísticasclínicasdeneoplasiasdeparótidassubmetidasatratamento cirúrgicopelomesmocirurgião.
Método: Estudoretrospectivo,ondeforamavaliados154pacientescomneoplasiadeparótida. Dadosclínicos,histológicos,tipodecirurgiaecomplicac¸õesforamcompiladosedescritos.
Resultados: Aprincipalmanifestac¸ãofoiadeumamassatumoralcomumamedianadetempo deevoluc¸ãode12 mesesparaos tumoresbenignose5mesespara ostumores malignos.A ecografiafoioexamecomplementarmaisindicado.Dentreostumoresbenignos,oadenoma pleomórfico foiomaiscomum eocarcinomamucoepidermóideomaisfrequente dentreos malignos.A parotidectomiasuperficial compreservac¸ão donervo facial foia cirurgia mais indicadaeaparesiareversívelderamosdonervofacial,acomplicac¸ãomaisprevalente.
Conclusões:Oadenomapleomórficoéotumormaiscomumdaglândulaparótidaea parotidec-tomiasuperficialcompreservac¸ãodonervofacialéotratamentomaisadequadoparaamaioria dostumoresdebaixamorbidade.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Parotidtumorsaffect1:100,000people,representing2---3% of tumors of the head and neck and 80% of salivary glandtumors.1,2In1991,parotidtumorswerehistologically
classifiedintomorethan30typesbytheWorldHealth Orga-nization(WHO).2
Thecurrentliteratureestimatesthatapproximately80% of these tumors are benign, with pleomorphic adenoma beingthemostcommonandoccurringbetweenthefourth andsixthdecadesoflife.3Clinically,themostcommon
man-ifestation of pleomorphic adenoma is the presence of a solitary,solid,firm, lobulated, mobilenodularlesion with well-definedmargins,thatispainless,topalpation,andof longevolution. Thistypeof tumor canbequite largeand invariablysparesthefunctionofthefacialmusculature.The secondmostcommonbenigntumorisWarthin’stumor,which mostlyaffectsmenafterthefifthdecadeoflifeandmaybe bilateral.
Themostprevalentmalignanttumoristhe mucoepider-moidcarcinoma,followedbyadenoidcysticcarcinoma.The presenceofpain,facialparalysis,rapidgrowth,ill-defined margins, and skin infiltration are characteristics that are suspiciousformalignancy.2
The first diagnostic imaging assessment for parotid tumors is usually ultrasonography, but this assessment does notdetermine the indicationfor surgical treatment. Computed tomography or magnetic resonance imaging assessmentisnotessential,butmaybeindicatedinselected cases to plan appropriate treatment.2 Fine-needle
aspi-ration (FNA), whether or not guided by ultrasound, can be used as a complementary diagnostic test, especially when a non-characteristic manifestation of pleomorphic adenomaissuspected. The purposeofFNAis to differen-tiatebenignfrommalignanttumors,asitusuallydoesnot establish thedefinitive histologicaldiagnosis.1---3 Incisional
biopsy is contraindicated,asit is oftenthe causeof neo-plastic implantation and consequently, of recurrences of pleomorphicadenomasandmalignantneoplasms.Itis estab-lishedthatmultiple recurrencesofpleomorphicadenomas increasethepossibilityofmalignanttransformationofthe tumor(carcinomainapleomorphicadenoma)andpatients withthesetumorsoftenhaveundergoneabiopsyor inade-quatesurgicalexcisioninthepast.1
The parotid gland has a superficial lobe, lateral to the facial nerve, that comprises 4/5 of the glandular parenchyma,andasmallerdeeplobe.Superficial parotidec-tomy with facial nerve preservation is the most often indicated surgical procedure, as 90% of the tumors are locatedin theglandularsuperficiallobe and,thus,donot affectthefacialnerve.2Althoughtumorsmoreoftenaffect
thesuperficiallobe,thetermsubtotalparotidectomyseems moreappropriatethansuperficialparotidectomy.
Theassociationbetweenthefacialnerveandthegland is responsible for most of the technical difficulties and complicationsofthesurgicalapproaches.Becauseofa par-ticular tumor histologicaltypeor extension,a decisionto perform a parotidectomy withdeliberate sacrifice of the facial nerve trunk or branches, possibly with an associ-ated neck dissection, is sometimes made during surgery. Therefore, the pathologist’s contribution of frozen sec-tionexaminationduringsurgeryisessential.Thetreatment of malignant tumors of the parotid can be supplemented with adjuvant radiotherapy, but chemotherapy is rarely indicated.Theprognosisisdeterminedaccordingtothe his-tologicaltypeandthepre-andpost-surgicalstaging.2
Method
We reviewed the current literature and did a retrospec-tivestudyof154patientswithaprevioushistoryofparotid tumors,surgicallytreatedfrom1990 to2011bythe same surgeon,performedbydatabaseanalysis.Weincludedonly those patients with complete records and whose surgical indicationwasnotassociatedwithinflammatorydiseaseof theparotidormedicalconditionsotherthantumor-related. Allhistologicalfindingswereperformedbythesame pathol-ogistfromareferralhospital.
DatawerecomputedinanExcelspreadsheetand classi-fiedasvariablesoftheanalysis,whichinturnwereclassified as qualitative, with a numerical scale code, or as quan-titative. Qualitative variables included gender (male or female), disease symptoms, initial physical examination, preoperative tests, chosen surgical technique, postopera-tivecomplications,andhistologicaldiagnosis.Quantitative variableswereage(inyears),diseaseevolution,and follow-up(inmonths).Asfortheinitialsymptoms,thecaseswere classified as incidental mass, incidental lesion in imaging exams,localpain/inflammation,andpreviousbiopsy.Each ofthevariableswasgroupedaccordingtoanumericalscale. Regardingthephysicalexamination,caseswererecorded according to the initial clinical impression, which consid-ered lesion location (superficial or deep), size (≤2cm or
>2cm),and histologicalhypothesis according topalpation (non-palpable,adenoma,benignnon-adenoma,malignant). Regardingthe preoperative data,weverifiedwhether the patient had undergone computed tomography (CT), mag-neticresonanceimaging(MRI),orultrasound;theresultwas evaluatedandthetumorwasclassifiedasasolidorcystic lesion.FNAwasassessedforthegroupsasfollows:no exami-nation,benignresult,ormalignantresult.Asforthesurgical technique,theoperationswereclassifiedastotalor subto-talparotidectomy anddermalparotidectomy, dividedinto groupsrepresentedbyanumericalscalefrom0to2.
Thepresenceofintraoperativefrozensectionswas con-sidered. When present, the results were separated into two groups: benign and malignant. The presence of FNA and the definitive histological diagnosis were correlated. Regarding the surgical preservation of the facial nerve, thesamplecomprisedtwogroups:onesubmittedto inten-tionalsurgicalresectionandtheother inwhichitwasnot necessary.Postoperativecomplicationswerealsoanalyzed: transientparesis,transientparalysis,salivaryfistula,Frey’s syndrome,andpermanentfacialparalysis.Patientswhohad recurrenceduringtheperiodwereanalyzedregarding the histologicaltype.
ThedatabasewastransferredtoIBMStatisticalPackage fortheSocialSciences,PSS20software,wheredata anal-yseswere performed. The program wasusedtocalculate frequencies, means,medians,andstandard deviations, as wellastosetthedistributionasymmetryofscalarvariables. Frequencies were obtained for the nominal variables and crossoverswere evaluatedfor significanceusing Pearson’s
2test,withp<0.001consideredsignificant.
Results
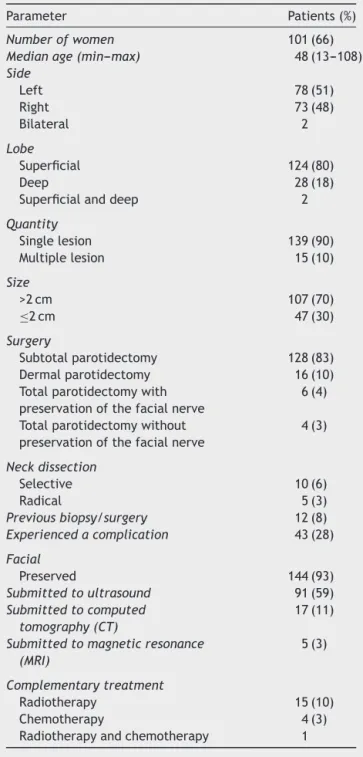
A total of 159 surgeries performed in 154 patients were selectedbetween1990and2011(Table1)and124 benign
Table1 Demographicanalysisofthesample.
Parameter Patients(%)
Numberofwomen 101(66)
Medianage(min---max) 48(13---108)
Side
Left 78(51)
Right 73(48)
Bilateral 2
Lobe
Superficial 124(80)
Deep 28(18)
Superficialanddeep 2
Quantity
Singlelesion 139(90)
Multiplelesion 15(10)
Size
>2cm 107(70)
≤2cm 47(30)
Surgery
Subtotalparotidectomy 128(83)
Dermalparotidectomy 16(10)
Totalparotidectomywith preservationofthefacialnerve
6(4)
Totalparotidectomywithout preservationofthefacialnerve
4(3)
Neckdissection
Selective 10(6)
Radical 5(3)
Previousbiopsy/surgery 12(8)
Experiencedacomplication 43(28)
Facial
Preserved 144(93)
Submittedtoultrasound 91(59)
Submittedtocomputed tomography(CT)
17(11)
Submittedtomagneticresonance (MRI)
5(3)
Complementarytreatment
Radiotherapy 15(10)
Chemotherapy 4(3)
Radiotherapyandchemotherapy 1
Table2 Histologicalassessmentofparotidtumors.
Histology Patients(%)
Benigntumors 121(79)
Pleomorphicadenoma 89(58)
Warthin’stumor 10(6)
Monomorphicadenoma 6(4)
Lymphoid-epithelialcyst 5(3)
Parotidductcyst 2
Lipoma 2
Oncocytoma 2
Branchialcyst 1
Epidermalcyst 1
Multiloculatedparotidcysts 1
Hemangioma 1
Melanocyticschwannoma 1
Malignanttumors 33(21)
Mucoepidermoidcarcinoma 9(6)
Squamouscellcarcinoma 7(4)
Lymphoma 6(4)
Aciniccellcarcinoma 3(2)
Undifferentiatedcarcinoma 2
Adenoidcysticcarcinoma 1
Ex-adenomapleomorphiccarcinoma 1
Fibrohistiocytoma 1
Fibrosarcoma 1
Myoepithelioma 1
Fibromyxoidsarcoma 1
Total 154(100)
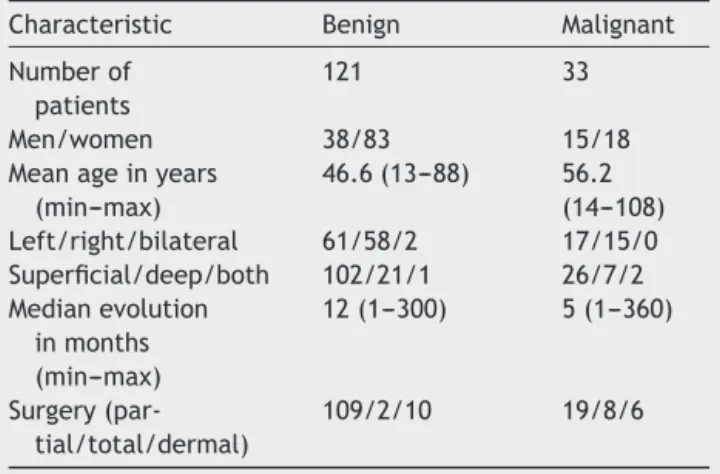
Table3 Clinicalcharacteristicsofbenign andmalignant tumors.
Characteristic Benign Malignant
Numberof patients
121 33
Men/women 38/83 15/18
Meanageinyears (min---max)
46.6(13---88) 56.2 (14---108) Left/right/bilateral 61/58/2 17/15/0 Superficial/deep/both 102/21/1 26/7/2 Medianevolution
inmonths (min---max)
12(1---300) 5(1---360)
Surgery (par-tial/total/dermal)
109/2/10 19/8/6
malignanttumors,59years.Regardingtheclinical examina-tion,theaccuracy ofpreoperativepalpationtodetermine theaffectedlobeandtoinferthehistologicaltypewas ana-lyzed.Theidentification oftumor depthonpalpationwas comparedwiththeintraoperative diagnosis andshoweda sensitivityof95.2%andspecificityof66.7%inthediagnosis oftumorsofthesuperficial lobe,whileit showeda sensi-tivityof64.3%andspecificityof96.8%forthoseinthedeep lobe.Incaseswherepalpationresultedinsuspected superfi-cialanddeepinvolvement,theexaminationsensitivitywas 100%andspecificitywas98.7%comparedtointraoperative diagnosis.
Toevaluate the accuracy ofclinical assumptionof his-tologicaltype,histologicalanalysiswasdefinedasthegold standardinthefollowingcategories:pleomorphicadenoma, benignnon-pleomorphicadenoma,andmalignant.Palpation identifiedcasesofpleomorphicadenomawithasensitivity of92.1%andspecificityof76.9%toruleoutother histologi-caltypes.Attheidentificationofbenigntumorsotherthan pleomorphicadenoma,palpationshowedasensitivityof75% andspecificityof89.3%whenrulingoutothercauses.Asfor thediagnosisofmalignancy,palpationshowedasensitivity of57.6%toidentifymalignantcasesandspecificityof100%. Followingthediagnosticflow,FNAindicationcaseswere reviewed. Forty-two patients underwent FNA, of which 66.7%werebenign,asopposedto26.2%malignantand7% inconclusivefindings.Consideringthepostoperativeresults of the histopathological assessment asthe gold standard, FNAhadasensitivityof90.9%toidentifycasesofmalignancy andspecificityof87.1%.TherewerethreeinconclusiveFNA reports,butallwerebenignatthehistologicalassessment. Regarding imaging studies, 17 CT and five MRI assess-ments were performed. Ultrasound was used in 91 cases and alterationswere observed in 98.9%of the cases.The most common alterationat the ultrasound was the pres-ence of solid lesion (77 cases), followed by cystic lesion (13 cases).The main solid pathologieswere: pleomorphic adenoma(47solid,twocystic,andonelesionwithout partic-ularities),monomorphicadenoma(foursolidlesionsfoundin fourtests),squamouscellcarcinoma(4/5),mucoepidermoid carcinoma (4/4), lymphoma (4/4), acinar cell carcinoma (2/2),oncocytoma(2/2),andlipomas(2/2).Themain cys-ticpathologieswere:Warthin’s tumor(fourcysticfindings infourtests),lympho-epithelialcyst(3/3),andparotidduct cyst(2/2).
The analysis of the surgical technique demonstrated a predominance ofsubtotalparotidectomies(83%),followed bydermalparotidectomies(10%),totalparotidectomywith preservation of the facial nerve (4%), and finally, total parotidectomywithoutpreservationofthefacialnerve(3%). Fifteen cases of neck dissection (ten selective and five radical)wereperformed.Theradicaldissectionswere per-formedinonecaseofsuperficialparotidectomy,onecaseof totalparotidectomywithpreservationofthefacialnerve, one case of total parotidectomy without preservation of the facialnerve,andtwo casesof dermal parotidectomy. Selectivedissectionswereperformedintwocasesof super-ficialparotidectomy,twocasesoftotalparotidectomywith preservation offacialnerve,twocasesoftotal parotidec-tomywithoutpreservationofthefacialnerve,andfourcases ofdermalparotidectomy. Thesensitivityandspecificityof theintraoperativefrozensectionanalysis,withpermanent histologyrepresentingthegold standardtoidentify malig-nancy,was66.7%and99.1%,respectively.
histology.Regardingcomplications,themainfindingswere: paralysisortransientparesis(21cases),salivaryfistula(six cases),Frey’ssyndrome(fivecases),andpermanentfacial paralysis(fivecases).
Discussion
Knowledgeinparotidtumorsisanessentialtoolforthe sur-geonatthetimeofdiagnosisandtreatment.Thescientific literatureincludessomeinstitutionalexperienceinthis mat-ter,withmostresultsindicatingthatbenigntumorsarethe mostfrequent.Thepresentstudyconfirmedtheprevalence ofbenigntumorsin81.4%ofthepopulationstudied,closeto theproportionreportedinotherstudies,whichdemonstrate consensusregardingpleomorphicadenomaasthemost fre-quentdiagnosisofparotidtumors.1---3
As formalignancy,mucoepidermoidcarcinoma and sec-ondarymetastaseseachrepresent5%ofthestudiedcases, andlymphoma,4.3%.In2002,Sungur found anequivalent proportion of malignant tumors, 17%, but reported ade-noid cystic carcinoma as the primary malignant tumor in hissample.In2008,studiesshowedahigherprevalenceof mucoepidermoidcarcinoma,equivalentto3%ofmalignant tumors of the sample.3 Taking these results in
considera-tion,webelievethatbothmucoepidermoidcarcinomaand adenoidcysticcarcinomashouldbeconsideredin casesof suspectedmalignancyofthetumor.
Masspalpationatparotidglandtopographywasthemain manifestationatthephysicalexaminationinthestudy pop-ulation,in93.9%ofcases,inagreementwiththeliterature. Therehave alsobeen isolatedreports of incidentallesion in imaging exams, local pain, or referral from another specialist. Palpation is established as an excellent clini-calparameterfortopographiclocationandclassificationof lesionsregardingmalignancy,withprovensignificanceinthe samplethroughitshighsensitivityfordemonstratingnodules inthesuperficiallobe(95.3%)andhighspecificityfor nod-ulesinthedeeplobe.Moreover,it showedasensitivityof 92.3%forclassificationofnodulesinpleomorphicadenoma and100%specificityforclassificationofnodulescompatible withmalignancy.Themeanevolutiontimeofbenigntumors wasapproximatelythreetimesgreaterthanthatof malig-nanttumors.Thesedataagreewiththeclinicalexperience that malignant tumorsare moreaggressive and have fast evolution,whereasbenignones,inturn,havean insidious onsetandslowgrowth.
Considering that clinical examination seems to be a good diagnostic method for benign tumors, it is under-stoodthattheindicationofcomplementarydiagnostictests occurspredominantly incases where thereissuspicionof malignancy, which occurred in 27.3% of cases, in accor-dance with previous studies.1 Compared to postoperative
anatomopathological results, FNAshowed excellent sensi-tivityandspecificityforthediagnosisofmalignanttumors, especially when associated with appropriate assessment of clinical criteria associated with malignancy. In 2004, Bova et al. showed that FNA had significant sensitivity andspecificityformalignanttumorsintheirsample4;
how-ever,anotherrecentstudyfrom2013demonstratedthrough retrospective analysis that FNA is also a reliable method for preoperative analysis for benign tumors, with higher
sensitivityandspecificitynotjustforbenign,butboththan imagingtests.Inthesamestudy,thesensitivityand speci-ficityassociatedwithFNAwas85.7%and99.5%,respectively, similartotheresultofthe154patientsinthissample,90.9% and87.1%,respectively.Thesametrendwasobservedinthe studiedsample;i.e.,imagingtestswererequestedonlyin caseswheretherewasasignificantsuspicionofmalignancy or involvement of adjacent structures, showing adequate sensitivityinthesecases.5
Therefore, this sample was similar to recent studies regarding the request for additional tests. CT was uti-lizedmorefrequentlythanMRIasitwasamoreaccessible examination in Brazil, especially considering the years comprising this study. As for the surgical management of parotidtumors, both subtotal andtotal parotidectomy aresafe procedures in experienced hands,with transient facialnerveparalysis representingthemaincomplication, whichappearslessfrequentlyinmoreconservativesurgical procedures.6
This sample showed marked prevalence of subtotal parotidectomy(83.9%),inwhichlymphnoderesectionwas necessaryin only2.2% ofcases.This is justifiedby a pre-viouslynoted higher frequency of benign tumors,such as pleomorphicadenoma. Cases in which full parotidectomy wasindicatedhadaconclusivemalignanthistopathological diagnosisin 75% ofcases. When decidingthemost appro-priate surgical procedure, intraoperative frozen section evaluation showed high sensitivity (90.9%) and specificity (100%)foridentifyingmalignancyinagreementwiththe lit-erature,which indicates that it is a good method in this surgicalchoice.6
Highspecificity is desirablein an intraoperative exam-ination,asit canreliablyrule outmalignancy, preventing unnecessaryradicalinterventions. Anotherprocedurethat hasbeen studied in the managementof benign tumors is dermalparotidectomy,whichaccordingtoAlbergottietal., 2012,intheirmeta-analysis,showedrecurrencerates simi-lartosuperficialparotidectomy,albeitwithlowerincidence ofmajorcomplications.7Inthepresentstudy,thechoiceof
thisprocedurewasmainly associatedwithcasesof recur-rence,andin50%ofcases,patientswithaprevioushistory ofbiopsy(performedatotherservices).
The most-feared postoperative complication after parotidsurgery is facial paralysis, which occurs at a fre-quencyof20---40% in theliterature, withonly 4% ofcases beingdefinitive.6---8Thepresentstudyshowedanincidence
of 15% of cases with postoperative facial paralysis and only 1.9% of cases with permanent paralysis. Thus, it is concluded that cases of permanent paralysis are rare, andareassociatedwithseveremalignantcases withprior involvementofadjacentstructures.
Conclusions
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ShashinderS,TangIP,VelayuthamP,PrepageranN,GopalaKG, KuljitS,etal.Areviewofparotidtumorsandtheirmanagement: aten-year-experience.MedJMalasia.2009;64:31---3.
2.Sungur N,Akan IM,Ulusoy MG, OzdemirR, Kilinc¸ H, OrtakT. Clinicopathologicalevaluationofparotidglandtumors:a retro-spectivestudy.JCraniofacialSurg.2002;13:26---30.
3.LinCC,TsaiMH,HuangCC,HuaCH,TsengHC,HuangST.Parotid tumors:a10yearexperience.AmJOtolaryngol.2008;29:94---100.
4.BovaR,SaylorA,ComanWB.Parotidectomy:reviewoftreatment andoutcomes.ANZJSurg.2004;74:563---8.
5.TryggvasonG,GaileyMP,HulsteinSL,KarnellLH,HoffmanHT, FunkGF,etal.Accuracyoffineneedleaspirationandimagingin thepreoperativeworkupofsalivaryglandmasslesionstreated surgically.Laryngoscope.2013;123:158---63.
6.Upton DC, McNamar JP, Connor NC, Harari PM, Hartig GK. Parotidectomy:tem-yearreviewof237cases atasingle insti-tution.OtolaryngolHeadNeck.2007;136:788---92.
7.AlbergottiWG,NguyenSA,ZenkJ,GillespieMB.Extracapsular dissectionforbenignparotidtumors:ameta-analysis. Laryngo-scope.2012;122:1954---60.