Cent ro de Neurologia Pediát rica - CENEP, Depart ament o de Pediat ria, Hospit al de Clínicas de Curit iba, Universidade Federal do Paraná UFPR Curit iba, PR, Brazil: 1Pediat ra do Depart ament o de Pediat ria da UFPR; 2Neuropediat ra, Prof essor Assist ent e do Depart ament o
de Pediatria da UFPR; 3Neuropediatra, Professora Adjunta do Departamento de Pediatria da UFPR; 4Neonatologista, Professor Assistente
do Depart ament o de Pediat ria da UFPR; 5Cirurgião Pediát rico, Prof essor Adjunt o do Depart ament o de Cirurgia da UFPR; 6Neuropediat ra; 7M édico Cirurgião Pediát rico.
Received 12 February 2004, received in f inal f orm 2 June 2004. Accept ed 6 July 2004.
Dr. Isac Bruck - Rua Floriano Essenf elder 81 - 80060-270 Curit iba PR - Brasil. E-mail: ibruck@t erra.com.br
M YELOM ENINGOCELE
A Brazilian Universit y Hospit al experience
M aria M .M . Ulsenheimer
1, Sérgio A. Ant oniuk
2,
Lúcia H.C. dos Sant os
3, M arcos P. Ceccat t o
4,
Ant ônio Ernest o da Silveira
5, Ana Paula Ruiz
6, Paulo Egger
7, Isac Bruck
2ABSTRACT - We analyzed 31 children with myelomeningocele born between July 1990 and July 2000. Follow-up median w as 24 mont hs (6-68mont hs). Only 2 mot hers had a know n et iologic f act or (diabet es mellit us). Tw elve had t he correct prenat al diagnosis. All children w ere born at t erm; 23 by cesarean; 13 had rupt ure of t he membrane. Surgical correct ion had a 4 days median (1 t o 44 days). Lumbosacral lesions w ere t he most f requent (46% ). Thirt y pat ient s w ere hydrocephalic, shunt w as placed in 27. M eningit is w as 4 t imes more f requent in shunt ed pat ient s. Seven became epilept ic (19.4% ). Denver II t est show ed signif icant delay in gross mot or development . Neurogenic bladder w as diagnosed in 12 pat ient s. Congenit al clubf oot w as t he main ort hopedic malf ormat ion (53% ). Six inf ant s died. Now adays, 17 pat ient s are being f ollow ed. A mult idisciplinary approach probably helps f or a bet t er qualit y of lif e.
KEY WORDS: meningomyelocele, neural t ube def ect s, neurological disabilit ies.
M ielom eningocele: experiência de um hospit al universit ário brasileiro
RESUM O - Avaliamos 31 crianças com mielomeningocele nascidas ent re julho de 1990 e julho de 2000. A mediana de acompanhament o f oi 24 meses (6-68m). Duas mães possuíam conhecido f at or de risco (dia-bet es mellit us). Doze obt iveram corret o diagnóst ico pré-nat al da pat ologia. Todas as crianças nasceram a t ermo; 23 via cesariana; 13 apresent aram rupt ura de membrana. A mediana de correção cirúrgica f oi 4 dias (1-44d). Lesões lombosacras f oram as mais f reqüent es (46% ). Trint a pacient es apresent aram hidroce-f alia, sendo a derivação vent rículo perit oneal (DVP) necessária em 27. M eningit e hidroce-f oi 4 vezes mais hidroce-f requent e em pacient es com DVP. Set e pacient es eram epilépt icos (19,4% ). O t est e de Denver II most rou at raso mot or signif icant e. Bexiga neurogênica f oi diagnost icada em 12 pacient es. Pé t ort o congênit o f oi a malf ormação ort opédica mais comum (53% ). Seis pacient es morreram. At é o moment o, 17 pacient es são acompanhados. Uma abordagem mult idisciplinar provavelment e colabora para melhor qualidade de vida.
PALAVRAS-CHAVE: mielomeningocele, def eit os do t ubo neural, def iciências neurológicas.
M yelomeningocele has a f requency of approx-imat ely 1:1000 new born alive, w it h preponderan-ce in f emales and w hit e rapreponderan-ce1,2. It is a neural t ube
def ect (NTD) t hat result s f rom a f ailure of closure of t he neural t ube during t he f ourt h w eek of em-bryogenesis. It can occur since cervical unt il sacral region. Depending on t he level of t he lesion can cause dif f erent grades of neurological dysf unct i-on2. Et iology is variable, involving bot h genet ic and
environment al f act ors, as f or inst ance an inade-quat e level of f olic acid during embryonary
neuru-lat ion2-8. The cyst ic appearance not ed at t he spinal
cord is easy to diagnose at newborn period and must be repaired w it hin 24 t o 48 hours t o reduce t he risk of inf ect ion. How ever, t reat ment is not limit ed t o t he closure of t he NTD, since ot her syst ems show abnormalit ies, as urinary syst em, f or example2.
ob-served. Thus, it is import ant t hat t he healt h care inst it ut ions and t he societ y as a w hole, be prepare t o receive t hese children and of f er t hem a bet t er qualit y of lif e.
On t his basis, w e review ed t he pat ient s w it h myelomeningocele born or t ransf erred t o t he ma-t ernima-t y of our hospima-t al, ma-t o dema-t ermine ma-t heir clinical prof ile, t he t reat ment approach of f ered t o t hem, and t heir f ollow -up. Special at t ent ion w as paid t o neurological perf ormance, and t o det erminig w e-t her e-t he children w ere able e-t o w alk and e-t o acquire sphinct er cont rol.
M ETHOD
We review ed t he f ollow -up of neonat es born in t he mat ernit y of Universit y Hospit al of Universidade Federal do Paraná bet w een July 1990 and July 2000, as w ell as new borns w it h myelomeningocele t ransf erred t o Neo-nat al Int ensive Care Unit (ICU) of our Hospit al during t he same period. The Et hical Commit t ee of t his Hospit al ap-proved t he st udy.
Prenatal and neonatal data were reviewed from Neona-tal ICU registers. Other data were collected from outpati-ents care register, accomplished by neurologic and surgi-cal teams, composed by resident of third and fouth years under supervision of teachers of the respective disciplines. We analyzed gender, race, f amily hist ory, and mat er-nal aspect s t hat could have some relat ion w it h t he occur-rence of t he disease (drugs in use, age, parit y, educat ion-al level, prenat ion-al care, and basic diseases), as w ell as t ime of diagnosis (pre or post -nat al), perinat al dat a (t ype of delivery, gest at ional age by Parkin, new born w eight , Ap-gar score, head circumf erence, ort hopedic abnormali-ties), characteristics of the lesion (location, presence or not of membrane rupt ure, use of prophylact ic ant ibiot ics) and cent ral nervous syst em (CNS) abnormalit ies, seen t h-rough comput ed t omography (CT) scan or ult rasonogra-phy (US), dat e of surgical correct ion and insert ion of ven-t ricle periven-t oneal shunven-t (VPS). The Denver II Screening ven-t esven-t w as used t o assess t he neuropsychomot or development of t hese pat ient s up t o t he age of 2 years9,10. Ot her dat a
relat ed t o neurological complicat ions have also been indicat ed, such as: epilepsy, meningit is, VPS changes).
Urological f ollow -up est abilished at t he out pat ient clinic of pediat ric surgery w ere also evaluat ed by means of imaging exams such as urography, echography or urodynamic evaluat ion; presence or not of neurogenic bladder, prophylact ic use of ant ibiot ics f or inf ect ion of urinary tract, use of catheterization or not, sphincter con-t rol, abilicon-t y con-t o w alk and renal f unccon-t ion monicon-t orizacon-t ion. Ort hopedic def ormat ions w ere also described.
RESULTS
A total of 36 cases of myelomeningocele were de-t ecde-t ed bede-t w een 20369 liveborn inf ande-t s ade-t our
ma-ternity between July 1990 and July 2000, equivalent t o a prevalence of 1.8 cases/1000 liveborn inf ant s.
The ef f ect ive number of pat ient s in t he st udy w as 31.26 of t hem originally f rom our mat ernit y and 5 born in ot her mat ernit ies in t he st at e and t ransf erred t o t he neonat al ICU of our Hospit al in t he f irst f ew days of lif e. Ten pat ient s born in our mat ernit y w ere excluded because t hey didnot re-t urn re-t o oure-t pare-t ienre-t clinic f or f ollow -up.
There w as a f rank preponderance of w hit e race (29 pat ient s = 93.5% ) but no dif f erence in gender (16 f emales: 15 males). M ean mat ernal age w as 25 years old (SD7.3 years). Educat ional level ranged f rom 1 t o 11 years of st udy (mean ± SD= 7.7 ± 3.7years). Wit h respect t o f amily origin, 10 w ere f rom Curit iba, 10 f rom met ropolit an region of t he city and 11 from other towns in the State of Parana. Tw o mot hers had diabet es mellit us during preg-nancy, 1 epilepsy, 2 rheumat ic disease, 2 cancer and 2 syst emic hypert ension. None of t hem made use of medicat ion considered t o cause myelomeningo-cele during pregnancy. Tw ent y f ive (80.6% ) cases occurred bet w een t he f irst and second pregnan-cy, and t here w as one case w it h f amily hist ory of first degree relatives. None of the women used folic acid as a mean t o prevent NTD.
Tw elve cases (39% ) w ere diagnosed prenat al-ly. Ten ot her cases (32.2% ) had pre-nat al diagno-sis of hydrocephalus only, as part of NTD. Just one pregnant w oman didnot receive prenat al care. In other 8 (25%), there wasnot information about pre-nat al care on t heir regist ers.
Cesarean sect ion w as t he pref erent ial rout e of delivery (23 cases = 74%). Similar percentage of rup-t ures of rup-t he myelomenigocele membrane occurred w het her delivery w as vaginal or cesarean sect ion (10 among 23 cesarean sect ions = 43% and 3 in t he 8 vaginal delivery = 37.5% ). M ean gest at ional age w as 39 and a half w eeks (SD 1 w eek), and mean inf ant w eight w as 3009gr (SD 573gr). The Apgar score w as below 6 at 5 minut es in only one case.
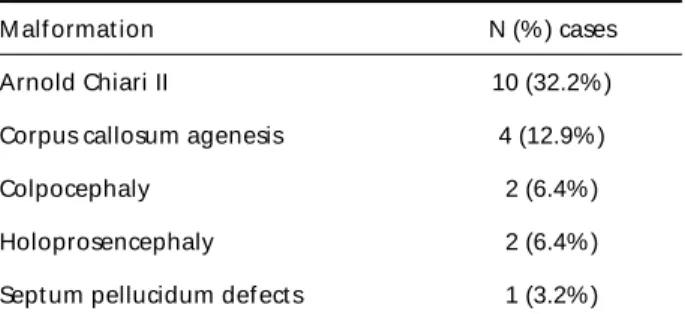
Table 1. Associat ed cent ral nervous syst em malf ormat ions.
M alf ormat ion N (% ) cases
Arnold Chiari II 10 (32.2% )
Corpus callosum agenesis 4 (12.9% )
Colpocephaly 2 (6.4% )
Holoprosencephaly 2 (6.4% )
M ean head circumf erence at birt h w as 35.5cm (SD 3.6cm). The level of t he lesion w as cervical in 2 cas-es (6% ), t horacolumbar in 10 (32% ), lumbar in 4 (13% ), lumbo-sacral in 14 (46% ) and sacral in one (3% ). Sevent een pat ient s had associat ed clubf oot (53% ), 5 st rabismus (16% ) and 2 congenit al sub-luxat ion of t he hips (6.4% ).
Morphological evaluation of the CNS was perfor-med by cranial US in 20 cases (64.5% ) and CT scan in 11 cases (35.4% ), t he exams being carried out , on average, at 1.5 days of lif e (1-60 days). Thirt y pa-t ienpa-t s show ed apa-t leaspa-t some degree of hydroce-phalus (97%) and ten of them had Chiari type II mal-f ormat ion (32% ). There w ere also ot her kinds omal-f associat ed malf ormat ions, as seen in Table 1.
Correct ion of myelomeningocele w as in medi-an at f our days of lif e (1 t o 44 days). A VPS w as nec-essary in 27 of t he pat ient s (90% ), in a second sur-gical st ep at a median age of 15 days (3 – 270 days), except f or one case w ho w as submit t ed t o t he correct ion of t he myelomeningocele and VPS simult aneously. Eight een pat ient s (58% ) needed at least one reintervention to change the VPS, because of meningit is in 14 of t hem. The f irst episode of meningit is occurred at a median age of 21 days (4 t o 49 days). Among pat ient s w it hout VPS, only 1 had one episode of meningit is. Epilepsy w as diag-nosed in 7 pat ient s (22.5% ); all had VPS and
pre-vious hist ory of meningit is. During t he st udy peri-od, t w o pat ient s show ed a t et hered cord and t hree ot hers, import ant spinal def ormit ies.
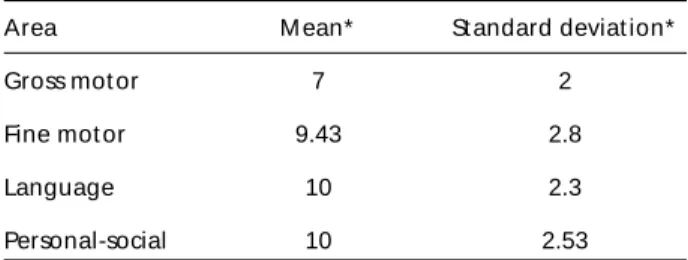
The f irst neurological evaluat ion at t he out pa-t ienpa-t clinic occurred w ipa-t h a median of 48 days of lif e (1 - 570 days), and t he pat ient s w ere f ollow ed up f rom 6 t o 68 mont hs (median = 24 mont hs). Of t hese, 21 (68% ) w ere evaluat ed at 1 year of age by Denver II screening t est , t hat show ed a great er delay on gross motor area, with a mean performan-ce corresponding t o t hat of a child of 7 mont hs; w hile in t he ot her areas (f ine mot or adapt ive, lan-guage and personal-social) t he mean age corre-sponded t o t hat of a 10 mont h-old child (see Table 2). The same w as seen in 13 pat ient s (42% ) evalu-at ed evalu-at 2 years of age (see Table 3), f or w hom t he mean age f or gross mot or f unct ion w as 6 mont hs low er t han f or ot her areas (f ine mot or adapt ive, language and personal-social). The language area, w hich is bet t er evaluat ed at t his age, did not show any delay.
Urologic evaluat ion by a pediat ric surgeon w as done in 19 pat ient s (61% ), w it h t he f irst exam be-ing perf ormed w it h a median age of 90 days of lif e. (2 days - 2 years) The pat ient s w ere f ollow ed f or 4 mont hs up t o 60 mont hs (median of 27 mont hs). Twelve patients (38.7%) had the diagnosis of neuro-genic bladder made by urodynamic met hods, w it h a median of 12 mont hs of age (1 - 64 mont hs). The 7 pat ient s w it hout t his diagnosis w ere t hose w ho w ere not submit t ed t o urodynamic st udy.
Fourt een pat ient s (45% ) w ere submit t ed t o imaging st udies (US and/or uret rocyst ography), hy-dronephrosis and vesico-uret heral ref lux w ere diagnosed in 3 of t hem. Treat ment consist ed of intermittent catheterization for these last 3 patients and also f or 4 more pat ient s w ho had import ant vesicle residues. One pat ient had been under int er-mit t ent cat het erizat ion since he w as 6 days old due t o early global vesicle f ormat ion. The associat ion of ant icholinergic medicat ion w as necessary f or 7 pat ient s and w as st art ed at t he median age of 26 mont hs (4 - 58 mont hs). One pat ient required t he combinat ion of doxozym w it h oxybut ynin and anot her one t he combinat ion of imypramine and oxybut ynin. Ten pat ient s had repeat ed episodes of urinary tract infection (UTI), with half of them being submit t ed t o int ermit t ent cat het erizat ion. All pat ient s w it h t he diagnosis of neurogenic bladder w ere t aking a prophylact ic ant ibiot ic against UTI.
Six pat ient s died, all bef ore t he age of 2 years (4 - 20 months): two of meningitis, 1 bronchoaspiration,
Table 2. Neurological evaluat ion by Denver II at 12 mont hs of age (n=21).
Area M ean* St andard deviat ion*
Gross mot or 7 2
Fine mot or 9.43 2.8
Language 10 2.3
Personal-social 10 2.53
* in mont hs
Table 3. Neurological evaluat ion by Denver II at 24 mont hs of age (n=13).
Área M ean* St andard deviat ion*
Gross mot or 15.6 6.9
Fine mot or 22.1 4.37
Language 23 3.1
Personal-social 22.3 3.9
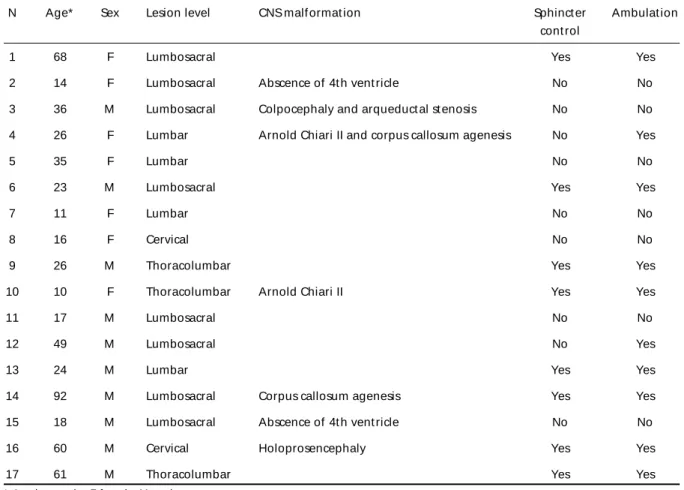
1 pneumonia and 2 due to an unknown etiology. At present , 17 of t he 31 pat ient s are being f ollow ed in our service, all of t hem w it h good preservat ion of renal f unct ion, 8 have sphinct er cont rol and 10 are able t o w alk (communit y ambulat ion) (Table 4).
DISCUSSION
The prevalence of myelomeningocele of 1.8 ca-ses/1000 liveborn neonat es f ound in our service is a lit t le higher t han t he value report ed w orldw ide, w hich is around 1/1000, but agrees w it h t he val-ues report ed in ot her Sout h America count ries1,2.
The preponderance of w hit e race f ound in our st udy may ref lect only t he race dist ribut ion of our populat ion. The apparent equal gender dist ribu-t ion is f alse, since if w e included ribu-t he 12 paribu-t ienribu-t s born in our mat ernit y w ho didnot ret urn t o nerological evaluat ion and w ere excluded of t he st u-dy, t he number of f emales w ould be higher t han t he number of males, as has been described by Greene at al11.
In 62% of our patients the level of the lesion was lumbar or lower, this probably being one of the
rea-sons w hy many pat ient s w ere able t o w alk, al-though patients with myelomeningocele at high le-vel can also achieve communit y ambulat ion w hen t hey receive good care, as report ed by Charney at all12. (Table 4). Environment al f act ors may play a
ro-le in t he higher risk of t he pat hologic embryo de-velopment, as occurred in 2 cases of gestational dia-bet es, w hich is know n t o act as a cof act or of NTD2.
The genet ic cont ribut ion t o malf ormat ion of neu-ral t ube is suggest ed by t he predominance of it s occurrence in t he f irst and second gest at ion. This emphasizes t he import ance of prevent ion of recur-rences in f amilies at higher risk t o have a second child affected by the same NTD malformation, what can be achieved by simple measures such as t he use of f olic acid bef ore an during pregnancy3-8.
The major reason w hy part of t he pat ient pop-ulat ion w as lost t o f ollow -up w as t he f act t hat 30% of t he pat ient s’ f amilies lived in t ow ns out -side Curit iba and it s met ropolit an region. M ost of t he mot hers had a st able st at us, since 24 (77.41% ) of t hem w ere married and t his f act or associat ed w it h a reasonable educat ional level are import ant
Tabela 4. M ain clinical f eat ures.
N Age* Sex Lesion level CNS malf ormat ion Sphinct er Ambulat ion
cont rol
1 68 F Lumbosacral Yes Yes
2 14 F Lumbosacral Abscence of 4t h vent ricle No No
3 36 M Lumbosacral Colpocephaly and arqueduct al st enosis No No
4 26 F Lumbar Arnold Chiari II and corpus callosum agenesis No Yes
5 35 F Lumbar No No
6 23 M Lumbosacral Yes Yes
7 11 F Lumbar No No
8 16 F Cervical No No
9 26 M Thoracolumbar Yes Yes
10 10 F Thoracolumbar Arnold Chiari II Yes Yes
11 17 M Lumbosacral No No
12 49 M Lumbosacral No Yes
13 24 M Lumbar Yes Yes
14 92 M Lumbosacral Corpus callosum agenesis Yes Yes
15 18 M Lumbosacral Abscence of 4t h vent ricle No No
16 60 M Cervical Holoprosencephaly Yes Yes
17 61 M Thoracolumbar Yes Yes
for the cognitive development, as has been demon-st rat ed by Bier et al13.
A prenat al diagnosis by US is dif f icult t o be es-tablished, and it usually identifies only the hydroce-phalus and t heir dist ort ions, as w e saw in t he pres-ent st udy. To be visualized, t he def ect must be lo-cat ed in t he vert ebral column, since t he cyst ic-like sac can not be seen by US14,15. There is no
agree-ment about t he best rout e of delivery, but it seems t hat cesarean sect ion bet t er prot ect s t he sac mem-brane f rom rupt ure2,16,17. In t he present st udy t here
w ere no dif f erences in t he number of rupt ure of t he membrane bet w een cesarean sect ion and vagi-nal delivery. All neonat es w ere f ull t erm, in con-t rascon-t con-t o con-t he licon-t eracon-t ure w hich reporcon-t s a higher preva-lence of NTD among premat ure inf ant s. Also, 20% of t he inf ant s st udied w ere of low birt h w eight (≤2500gr), as also report ed by Aguiar et al3.
Only one of the patients had an Apgar score bel-low 6 at 5 minut es, a f act excluding t he possibili-t y of perinapossibili-t al asphyxia as possibili-t he cause of delayed de-velopment18. Head circumf erence w as w it hin
nor-mal values at delivery, alt hough hydrocephalus was already present, and decompensation occurred later on, after correction of the myelomeningocele. Hydrocephalus is present in nearly 90% of t he cas-es at t he age of 4 mont hs, as w as also t he case in t he present st udy13. Regarding ot her
complica-t ions, Chiari II malf ormacomplica-t ion, complica-t ecomplica-t hered cord, orcomplica-t ho-pedic and urologic def ect s w ere t he most prepon-derant , as also report ed in t he lit erat ure2,15.
Alt hough t he correct ion of myelomeningocele should be perf ormed as soon as possible, pref eren-t ially w ieren-t hin eren-t he f irseren-t 72 hours of lif e, in some of t he present pat ient s t he correct ion w as made up to 44 days of life. A ventriculoperitoneal shunt, indi-cat ed t o t he pat ient s w it h hydrocephalus, w as per-f ormed in 90% oper-f t hem in a second st age in order t o reduce t he chance of CNS inf ect ion2,19. Even so,
how ever, episodes of meningit is w ere responsible f or reint ervent ions in order t o change t he VPS in 14 pat ient s, usually bef ore one mont h of it s place-ment . The large number of CNS inf ect ions t hat occurred in our sample could be most ly explained by t he delay in correct ing t he myelomeningocele in many of t hem (af t er 72 hours)2,20-22. The mort
alit y rat e w as relat ively low despalit e delays in correct -ing t he NTD, t hanks t o t he use of prophylact ic ant ibiot ic20,22. The associat ion of epilepsy and
mye-lomeningocele in t he present st udy w as probably relat ed t o t he presence of VPS t hat compensat es
for hydrocephalus, plus previous episodes of menin-git is, also ment ioned by ot her aut hors23-25.
Denver II Test show ed t hat t he major delay in t he development al milest one of our pat ient s occur-red in t he gross mot or area, direct ly aff ect ed by t he myelomeningocele. The int elligence quot ient (IQ) w as not available f or most of t he pat ient s and t heref ore it w as impossible t o assess t heir cognit ive level but , based on Fobe et al, a normal IQ can be achieved up t o 80% of t he pat ient s21. Denver II
Screening Test in children at risk, in w hich t here is up t o one f ailure at t he age of 2 years, w as f ound an IQ>80, by WPSSI-R, in 70% of t hese children at the age of 5 years, according to Frankenburg et al.10
and Bruck et al. (personal comunicat ion). The
lan-guage area, w hich is bet t er evaluat ed at 2 years old did not show any delay, indicat ing t hat t he prob-lem mainly concerns t he gross mot or area.
It w as an agreeable surprise t o observe t hat , al-though the diagnosis of bladder dysfunction was ma-de w it h a ma-delay in many of t he pat ient s, all show ed preservat ion of renal f unct ion, and many of t hem w ere socially compet ent (dry f or 3 hours) (Table 4). We w ould like t o emphasize t hat t he lit erat ure rec-ommends intermittent catheterization during the first year of lif e, and even st art ing at birt h because t his procedure does not involve major side eff ect s, and is of great benef it . Thus, it should be rout inely used even in t he absence of bladder dysf unct ion26-28.
We could see t hat many of t he mot hers looked f or urologic evaluat ion only lat t er on, because of t heir concern about t heir children being unable t o leave diapers at t he age supposed t o do it .
The mort alit y rat e in our sample w as 19% , gre-at er t han t hgre-at described by Brau gre-at al. (10-15% ) and all of t hem happened bef ore 2 years, w hich is t he age of great er risk20.
In conclusion t he present st udy represent s only a small sample of children w it h myelomeningocele and it is necessary more st udies made in ot her cent ers in order t o have a bet t er idea of how are t he Brazilian children w it h t his pat hology. been managed. We w ould like t o ment ion t hat t he Bra-zilian government is planning to enrich wheat flour w it h f olic acid, as a prophylact ic measure t o pre-vent pregnant w omen f rom having an of f spring w it h myelomeningocele29. These children if w ell
REFERENCES
1. Grillo E, Silva RJM. Defeitos do tubo neural e hidrocefalia congênita: por quê conhecer suas prevalências? J Pediatria 2003;79:105-106. 2. Northrup H, Volcik KA. Spina bifida and other neural tube defects. Curr
Probl Pediatr 2000;30:315-337.
3. Aguiar MJB, Campos AS, Aguiar RALP, et al. Defeitos de fechamento do tubo neural e fatores associados em recém-nascidos vivos e natimor-tos. J Pediatria 2003;79:129-134.
4. Czeizel AE, Dudas I. Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. N Engl J Med 1992;327:1832-1835.
5. Czeizel A E. Prevention of congenital abnormalities by periconcep-tional multivitamin supplementation. BMJ 1993;306:1645-1648. 6. Werler MM, Shapiro S, Mitchell AA. Periconceptional folic acid
expo-sure and risk of ocurrent neural tube defects. JAMA 1993;269:1257-1261. 7. Daly S, Mills JL, Molloy AM, Conley M, Lee YJ. Minimum effective dose of folic acid for food fortification to prevent neural-tube defects. Lancet 1997;350:1666-1669.
8. Kadir RZ, Sabin C, Whitlow B, Brockbank E, Economides D. Neural tube defects and periconceptional folic acid in England and Wales: ret-rospective study. BMJ 1999;319:92-93.
9. Glascoe FP, Byrne KE, Ashford LG, Johnson KL, Chang B, Strickland B. Accuracy of the Denver II in developmental screening. Pediatrics 1992;89:1221-1225.
10. Frankenburg WK, Dodds J, Archer P, Shapiro H, Bresnick B. The Denver II: a major revision and restandardization of the Denver Developmental Screeneing Test. Pediatrics 1992;89:91-97.
11. Greene WB, Terry RC, DeMasi RA, Herrington RT. Effect of race and gender on neurological level in myelomeningocele. Dev Med Child Neurol 1991;33:110-117.
12. Charney EB, Melchionni JB, Smith DR. Community ambulation by children with myelomeningocele and high-level paralysis. J Pediatr Orthop 1991;11:579-582.
13. Bier JB, Morales Y, Liebling J, Geddes L, Kim E. Medical and social fac-tors associated with cognitive outcome in individuals with myelomeningocele. Dev Med Child Neurol 1997;39:263-266. 14. Dumas JL, Pascaud E, Novello G, Ronayette D, Rousseau J. Place de l’
écho-encéphalographie dans les myéloméningoceles. Ann Pédiatr (Paris) 1992;39:53-55.
15. Skari H, Bjornland K, Bjornstad-Ostensen A, Haugen G, Emblem R.
Consequences of prenatal diagnosis: a preliminary report on neonates with congenital malformations. Acta Obstet Gynecol Scand 1998;77:635-642. 16. Merril DC, Goodwin P, Burson JM, Sato Y, Williamsom R, Weiner CP.
The optimal route of delivery for fetal meningomyelocele. Am J Obstet Gynecol 1998;179:235-240.
17. Hill AE, Beattie F. Does cesarean section delivery improve neurologi-cal outcome in open spina bifida? Eur J Pediatr Surg 1994;4(Suppl 1):S32-S34.
18. Comitee on Fetus and Newborn of American Academy of Pediatrics and Comitee on Obstetric Practice of American College of Obstetricians and Gynecologists. Use and abuse of the Apgar Score. Pediatrics 1996;98:141-142.
19. Rolle U, Gräfe G. About the rate of shunt complications in patients with hydrocephalus and myelomeningocele. Eur J Pediatr Surg 1999;9(Suppl 1):S51-S52.
20. Brau RH, Rodríguez R, Ramírez MV, González R, Martínez V. Experience in the management of myelomeningocele in Puerto Rico. J Neurosurg 1990;72:726-731.
21. Fobe J, Rizzo AMPP, Silva IM et al. QI em pacientes com hidrocefalia e mielomeningocele. Arq Neuropsiquiatr 1999;57:44-50.
22. Charney EB, Melchionni JB, Antonucci D. Ventriculitis in newborns with myelomeningocele. AJDC 1991;145:287-290.
23. Hack CH, Enrile BG, Donat JF, Kosnik E. Seizures in relation to shunt dys-function in children with meningomyelocele. J Pediatr 1990;116:57-60. 24. Noetzel MJ, Blake JN. Prognosis for seizure control and remission in
chil-dren with myelomeningocele. Dev Med Child Neurol 1991;33:803-810. 25. Talwar D, Baldwin MA, Horbatt CI. Epilepsy in children with
meningomyelocele. Pediatr Neurol 1995;13:29-32.
26. Churchill BM, Abramson RP, Wahl EF. Dysfunction of the lower uri-nary and distal gastrointestinal tracts in pediatric patients with know spinal cord problems. Pediatr Urol 2001;48:1587-1629.
27. Kaefer M, Pabby A, Kelly M, Darbey M, Bauer SB. Improved bladder function after prophylactic treatment of the high risk neurogenic blad-der in newborns with myelomeningocele. J Urol 1999;126:1068-1071. 28. Wu H, Baskin LS, Kogan BA. Neurogenic bladder dysfunction due to
myelomeningocele: neonatal versus childhood treatment. J Urol 1997;157:2295-2297.