Arq Neuropsiquiatr 2005;63(2-B):530-531
1Clinical Department Hematology Service; 2Pathology Department;3N e u rology and Psychiatry Department, Botucatu Medical School, São Paulo State University - (UNESP), Botucatu SP, Brazil
Received 6 September 2004, received in final form 24 November 2004. Accepted 24 January 2005.
Dra. Lucilene S.R. Resende - Hemocenter Division / Botucatu Medical School - 18618-000 Botucatu SP - Brasil. E-mail: luan_resende@uol.com.br
ISOLATED RICHTER’S SYNDROME
IN CENTRAL NERVOUS SYSTEM
Case report
Lucilene S.R. Resende
1, Carlos Eduardo Bacchi
2, Luiz Augusto L. Resende
3,
Roberto Colichio Gabarra
3, Ligia Niéro-Melo
1ABSTRACT - Diffuse large cell non Hodgkin’s lymphoma associated with chronic lymphoid leukemia (CLL), or Richter’s syndrome, is a rare and serious complication. Isolated Richter’s syndrome in the central nervous system is very rare; only 12 cases have been reported. We describe a 74-year-old patient with diffuse large cell non Hodgkin’s lymphoma in the right frontal region with the appearance of multiform glioblastoma. KEY WORDS: Richter’s syndrome, central nervous system.
Sindrome de Richter isolada em sistema nervoso central: relato de caso
RESUMO - Linfoma não Hodgkin difuso de grandes células em paciente portador de leucemia linfóide crôni-ca (LLC), ou síndrome de Richter, é complicrôni-cação rara e grave nesta leucemia. Síndrome de Richter isolada no sistema nervoso central é muito rara, tendo sido encontrados apenas 12 casos descritos. Descrevemos paciente de 74 anos, que apresentou linfoma não Hodgkin difuso de grandes células em região frontal direita, simulan-do glioblastoma multiforme.
PALAVRAS-CHAVE: síndrome de Richter, sistema nervoso central.
The occurrence of a diffuse large cell non Hodg-k i n ’s lymphoma in a chronic lymphocytic leuHodg-kemia (CLL) patient was described by Richter in 19281; this
became known as Richter’s syndrome after 19642.
It is the most serious CLL complication3. Isolated
Ri-c h t e r’s syndrome in the Ri-central nervous system ( C N S ) is very rare, only 12 cases have been described3 - 9, 5
of them with isolated leptomeningeal involvm e n t4 , 6 , 9,
and the other 7 with parenchimal involvement. The aim of this paper is to re p o rt an additional case with isolated CNS Richter’s syndrome with ri-ght frontal lobe parenchimal involvement.
CASE
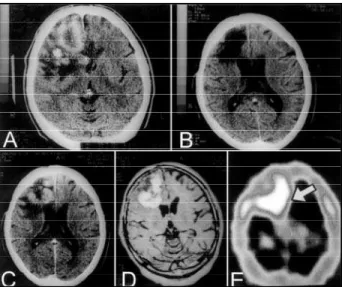
A 74-year-old white male had previously diagnosed CLL, presenting only leucocytosis (lymphocytosis) for 6 years; he had been receiving medical support in anoth-er sanoth-ervice with occasional use of chlorambucil, when he began to show mental confusion, bewilderment, and gait disorders. Cranial computerized tomography (CT) scan revealed an expansive process in the right frontal re g i o n Fig 1A. Extirpation of the lesion was indicated supposing
Arq Neuropsiquiatr 2005;63(2-B) 531
x a n t h o c h romic, with 10 ery t h o c y t e s / m m3, 7 l e u c o c y t e s / m m3 (95% lymphocytes; 5% monocytes), 203mg/dl protein, 49mg/dl glicosis, and negative Nanquin ink. Simultaneous diagnosis of CLL and diffuse large cell non Hodgkin lym-phoma of the CNS were established (Richter’s syndro m e ) . The patient received chlorambucil (4mg/day, continuous use), intrathecal chemotherapy (methotrexate = 12mg, cytarabine = 70mg, dexamethasone = 2mg - once a w e e k for 3 consecutive weeks), plus radiotherapy of the right c e rebral hemisphere (total of 3600 cGy within 4 weeks). CT scan after radiotherapy showed no tumor remnants in CNS, and revealed only a local porencephalic cyst (Fig 1B). Treatment of CNS lymphoma was stopped but tre a t-ment of CLL continued (chlorambucil). Five months lat-er the same neurological symptoms re a p p e a red. A slight-ly xanthochromic CSF showed 39 ery t h ro c y t e s / m m3, 2 leu-cocytes/mm3, 412 mg/dl protein, 52 mg/dl glicosis, and negative Nanquin ink. Imaging of CNS by CT scan, mag-n e tic resomag-namag-nce imagimag-ng (MRI), amag-nd cerebral perfusiomag-n with S e s t a m i b i - 9 9 m Tc (SPECT scan) revealed tumor relapse in the right frontal region [Fig 1C,D, E]. The choice was right f rontal lobectomy, perf o rmed without incident. He was d i s c h a rged receiving dexamethasone (4 mg/day), aceta-zolamide (500 mg/day), and carbamazepine (400 mg/day). He presented good evolution, practically free of neuro-logical sequels (with only brief periods of mental con-fusion). He died at home while sleeping on the 14thday post-operative, before any other adjuvant therapy.
DISCUSSION
R i c h t e r’s syndrome occurs in at least 1 to 10% o f CLL cases6, and is the most serious complication of
this disease3. The usual presentation is sudden c l i n
i-cal deterioration, assymetric adenomegaly, espleno-m e g a l y, fever, weight loss, increased lactate dehy-d rogenase, andehy-d monoclonal gammopathy. A l t h o u g h extra-nodal involvement is possible, isolated topog-raphy is extremely uncommon5 , 6 , 8. In the 12 CNS
cas-es, the lesion was meningeal in 5, and pare n c h imal in 7, as in our patient.
The malignant characteristics of cerebral large cell lymphoma probably resulted in a neuro rr a d i o l o-gical aspect similar to multiform glioblastoma. Ly m-phoma of cerebral parenchima is very serious. Our patient died only 7 months after surg e ry, radiother-apy, and intrathecal chemotherapy.
T h e re is evidence that prolymphocytic CLL trans-formation, blastic CLL crisis, and blastic transfor-mation of low grade non Hodgkin lymphomas can present closely related manifestations, signifying neoplastic pro g ression. Thus the malignant cells in the cerebral lymphoma of our patient could have developed as a subclone of his CLL4,8,9.
REFERENCES
1. Richter MN. Generalized reticular cell sarcoma of lymph nodes associa-ted with lymphatic leukemia. Am J Pathol 1928;6:285-299.
2. Lortholary P, Boiron M, Ripault J, Manus A, Bernard J. Leucémie lym-phoïde chronique secondairement associée à une réticulopathie maligne (syndrome de Richter). Nouv Rev Fr Hematol 1964;4:621-644. 3. O'Neill BP, Habermann TM, Banks PM, O'fallon JR, Earle JD. Primary
central nervous system lymphoma as a variant of Richter's syndrome in two patients with chronic lymphocytic leukemia. Cancer 1989; 15: 1296-1300.
4. Lane PK, Townsend RM, Beckstead JH, Corash L. Central nervous sys-tem involvement in a patient with chronic lymphocytic leukemia and non-Hodgkin´s lymphoma (Richeter´s syndrome), with concordant c e l l surface immunoglobulin isotypic and immunophenotypic markers. Am J Clin Pathol 1988;89:254-259.
5 . Bayliss KM, Kueck BD, Hanson CA, Matthaeus WG,A l m a g ro UA. Richter's s y n d rome presenting as primary central nervous system lymphoma: trans-formation of an identical clone. Am J Clin Pathol 1990;93:11 7 - 1 2 3 . 6. Robertson LE, Pugh W, O´Brien S, et al. Richter´s syndrome: a report
of 39 patients. J Clin Oncol 1993;11:1985-1989.
7. Mahé B, Moreau P, Bonnemain B, et al. Isolated Richter's syndrome of the brain: two recent cases. Nouv Rev Fr Hematol 1994;36:383-385. 8. Gilles FJ, O´Brien SM, Keating MJ. Chronic lymphocytic leukemia in
(Richter´s) transformation. Sem Oncol 1998;25:117-125.
9 . A g a rd G, Hamidou M, Leautez S, Garand R, Grolleau JY. Localisation neuro-méningée d´um syndrome de Richter. Rev Méd Interne 1999;20:64-67.